





















This case report describes the treatment of a nine-year-old female patient with a history of dental trauma at age five in the incisors area. She had an early mixed dentition, class I molar relationships and moderate crowding. The maxillary central incisor had not erupted, so we determined radiographically that it was impacted in a horizontal position toward the midline, the lateral incisor was inclined and the canine mesially displaced with an impaction tendency against the lateral incisor. Orthodontic treatment consisted of the placement of initial 4×2 orthodontic fixed appliances and space opening. The periodontal surgery was performed in two stages. In the first stage the central incisor was surgically exposed. Subsequently in the second stage, the maxillary right deciduous canine was extracted, then periodontal surgery was performed to expose the impacted permanent canine. Finally, we tractioned each tooth into its proper position.
Este reporte de caso describe el tratamiento de una paciente femenina de nueve años de edad con antecedente de trauma dental a los cinco años de edad en el sector anterior. Clase I esquelética y perfil convexo. A la exploración intraoral se observó dentición mixta, clase I molar y apiñamiento moderado en la arcada superior e inferior. El incisivo central superior derecho sin erupcionar y con pérdida de espacio por la migración mesial del incisivo lateral; se determinó radiográficamente que el incisivo central superior derecho estaba impactado en una posición horizontal hacia la línea media, el incisivo lateral inclinado y el canino con desplazamiento hacia mesial, perdiendo la guía de erupción del canino temporal y con tendencia a la impactación contra el incisivo lateral. El tratamiento ortodóncico consistió en la colocación de aparatología ortodóncica fija de 4×2 (Edgewise slot 0.022×0.025) inicial y apertura de espacio. La cirugía periodontal se realizó en dos tiempos: en la primera fase se realizó la exposición quirúrgica del incisivo central para la colocación de un botón para la tracción ortodóncica. En la segunda fase, se extrajo el canino temporal superior derecho, seguido de la cirugía de exposición del canino permanente impactado. Finalmente se traccionó cada uno al arco en su adecuada posición.
Dental impaction in spite of the fact that it might be considered as a type of ectopic eruption, its main feature is the absence of eruption of one or more teeth in the oral cavity.1 In most cases a larger or smaller infraosseous path of the impacted tooth can be seen, but without making its appearance in the oral cavity; there is no alveolar emergency or clinical emergency.1,2 It may be observed in the deciduous dentition, although in this case it can be the result of re-impactions of usually traumatic etiology.1,2 Much more frequently, impacted teeth are observed in permanent dentition; the most affected are the third molar and the upper canine, which, because of their significance and clinical importance deserve special attention.1 However, it is imperative to formulate a proper definition in the overall context of the eruption alterations responsible for the development of malocclusal situations, whether in isolation or in combination with other factors.1,3
Although the upper canine tooth is the most frequently impacted, the impaction of the upper central incisor represents a problem at an early age that is detected when the tooth fails to erupt.1-3 This tooth erupts before the canine, so its lack of eruption is easily detected by parents.1
The etiology of central incisors impaction are supernumerary teeth, odontomas and trauma,1–3 and the causes for the alteration and displacement in the eruption of the upper canines has been of interest to researchers for many years.1,2
In the radiographic analysis it has been observed in many patients that if there is movement towards mesial of a great portion of the lateral incisor, it may have a secondary influence on the canine’s eruption pattern.1,3
The diagnosis of impaction of the incisors and their influence on the movement of the canine’s eruption path is determined by the background referred by the parents, in addition to the clinical and radiographic examination.1,2
Despite the fact that a chronological pause of approximately four years separates the eruption between the canine and the lateral incisor, its anatomical proximity gives us reason to establish a causal association between the migration of the lateral incisor due to an impaction of a central incisor and canine displacement associated with an unusual upper incisor impaction.
Materials and methodsCase presentationFemale patient of nine years of age comes for treatment to the Division of Postgraduate Studies and Research at the Faculty of Dentistry of the National University of Mexico (UNAM). The chief complaint concerned the lack of eruption of an upper tooth. She was physically healthy and had a history of dental trauma at five years of age in the anterior oral region.
DiagnosisAt extraoral exploration, it was observed a dolichofacial pattern, symmetrical oval facial form, convex profile, facial and dental midlines do not match, lower third slightly increased, medium lips and lip competence (Figure 1).
 frontal photograph, B) smile photograph, C) lateral photograph. A moderate facial asymmetry and a slightly convex profi le is observed in the photographs.")
Intraoral examination showed mixed dentition, molar class I and canine class I in primary dentition. The upper right central incisor was found not erupted and with loss of space due to the mesial migration of the lateral incisor (Figure 2).
 right lateral radiograph: a molar class I is observed and canine class I (of primary canines), B) frontal photograph: it is possible to observe the space loss for the eruption of the right central incisor and the inclination of the lateral incisor, C) left lateral photograph: a molar class I (permanent) and a canine class I (primary) are observed, D) upper and lower occlusal views: an ovoidal arch form is observed and lower anterior interproximal spaces.")
Initial intraoral photographs. Intraoral clinical inspection: A) right lateral radiograph: a molar class I is observed and canine class I (of primary canines), B) frontal photograph: it is possible to observe the space loss for the eruption of the right central incisor and the inclination of the lateral incisor, C) left lateral photograph: a molar class I (permanent) and a canine class I (primary) are observed, D) upper and lower occlusal views: an ovoidal arch form is observed and lower anterior interproximal spaces.
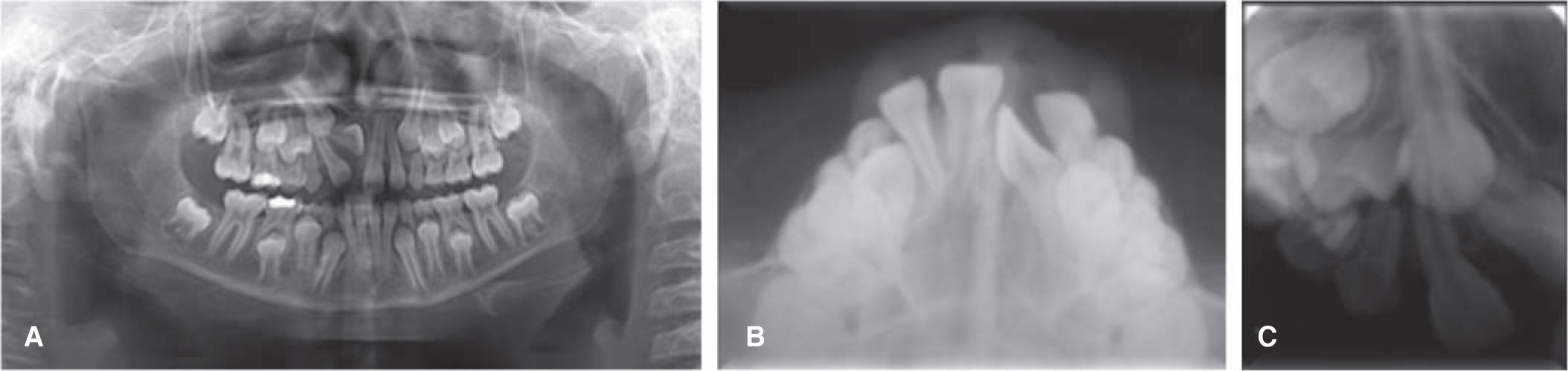
In the panoramic radiograph a mixed dentition is observed. It was determined that the upper right central incisor was impacted in a horizontal position, the lateral incisor was inclined and the canine was displaced mesially and had lost the eruption guide of the primary canine and had a tendency for impaction against the lateral incisor.
Root length was 2:1 in the majority of teeth with no apex formation; asymmetrical maxillary sinuses, mandibular condyles and ramus, without pathologies (Figure 3).
 Panoramic radiograph: the impaction of the upper right central incisor in a horizontal position can be observed and the canine’s mesial displacement with a tendency for impaction. B) Occlusal radiograph: the location of the central incisor is labia. C) Dentoalveolar radiograph where the displacement of the upper right canine and its tendency for impaction may be observed.")
Initial radiographs. A) Panoramic radiograph: the impaction of the upper right central incisor in a horizontal position can be observed and the canine’s mesial displacement with a tendency for impaction. B) Occlusal radiograph: the location of the central incisor is labia. C) Dentoalveolar radiograph where the displacement of the upper right canine and its tendency for impaction may be observed.
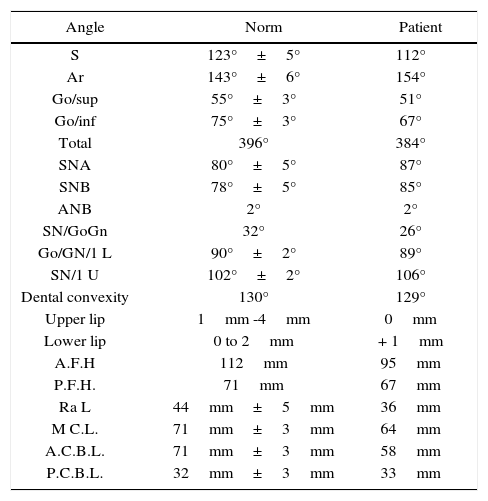
The results of the cephalometric analysis revealed a skeletal class I with horizontal growth tendency. Upper and lower incisors were in a correct position according to their basal bone (Figure 4andTable I).

Cephalometric analysis. Results from the Jarabak’s analysis where it was determined that the patient was a skeletal class I with a horizontal tendency of growth.
| Angle | Norm | Patient |
|---|---|---|
| S | 123°±5° | 112° |
| Ar | 143°±6° | 154° |
| Go/sup | 55°±3° | 51° |
| Go/inf | 75°±3° | 67° |
| Total | 396° | 384° |
| SNA | 80°±5° | 87° |
| SNB | 78°±5° | 85° |
| ANB | 2° | 2° |
| SN/GoGn | 32° | 26° |
| Go/GN/1 L | 90°±2° | 89° |
| SN/1 U | 102°±2° | 106° |
| Dental convexity | 130° | 129° |
| Upper lip | 1mm -4mm | 0mm |
| Lower lip | 0 to 2mm | + 1mm |
| A.F.H | 112mm | 95mm |
| P.F.H. | 71mm | 67mm |
| Ra L | 44mm±5mm | 36mm |
| M C.L. | 71mm±3mm | 64mm |
| A.C.B.L. | 71mm±3mm | 58mm |
| P.C.B.L. | 32mm±3mm | 33mm |
The following objectives were established at the start of the treatment: 1) traction of the impacted upper right central incisor and bring it into the dental arch, 2) to assess the position of the upper right canine with a tendency for impaction to determine the need for surgical exposure and orthodontic traction, 3) to maintain the skeletal class I and improve facial profile, 4) to keep the molar class I, 5) to achieve canine class I and a correct arch form in relation to the eruption of the missing permanent teeth, 6) to achieve adequate overbite and overjet, and 7) to get a stable and functional occlusion in the long term.
TreatmentOrthodontic treatment began in August 2010 and consisted on the placement of 4×2 fixed orthodontic appliances (Edgewise 0.022×0.025 slot) with initial 0.014 NiTi archwires in the upper and the lower arch and space opening for the upper right central incisor with an open coil (Figure 5).
 with 0.014 NiTi archwires and space opening for the upper right central incisor with open coil.")
By the second month, the first surgery for the exposure of the upper right central incisor was performed and a button was placed for orthodontic traction. Due to the complete rotation of the incisor the button was placed on the palatal side, so the prognosis for treatment success was considered reserved to unfavorable (Figure 6).

Fifteen days after suture removal orthodontic traction to the arch with elastic ligature was begun. This procedure was performed during four more months (Figure 7).

In the sixth month a 0.036” stainless steel accessory arch was placed in the accessory tubes of the molar bands and the incisor was tractioned with elastic ligature to the archwire. This procedure was performed for three more months (Figure 8).

By the tenth month, the complete crown of the upper right central incisor was noticeable, so an utility 0.016 stainless steel archwire was placed in the upper and lower dental arch. The open coil remained to preserve the space and buttons were placed on the labial side of the upper right central incisor and in the palatal surface of the central incisor. In the following appointment the accessory arch is removed and the upper left brackets are placed to make a movement of couple with elastomeric chains and align the incisor that was completely rotated. This procedure was performed for two more months and a radiographic control study was requested (Figure 9).

10th month: a 0.016 stainless steel utility archwire was placed on the upper and lower arches. The open coil was maintained for space preservation and a couple was made with elastomeric chains to align the upper right central incisor. This procedure was continued for two more months.
On the thirteenth month, radiographs are assessed and there is a bony defect around the upper right central incisor, the roots of the central incisor as well as the ones of the lateral incisor on the same side presented an important dilaceration, which is attributed to the trauma that the patient received in that area in the deciduous dentition. It was also noted that the contralateral canine had already fully emerged into the oral cavity and that the upper right canine was not able to erupt. The root was almost completely formed, and it was decided to refer the patient for the second exposure surgery for the upper right canine, which was also by the buccal area. A 0.016” NiTi archwire was placed in the upper arch and the same arch was left on the lower (Figure 10).
 upper right central incisor in the dental arch, B) radiographic evaluation where a bony defect was observed around the upper right central incisor and the root dilacerations on the central and lateral incisors. The root of the upper right canine is almost completely formed and with a tendency towards impaction.")
On the 13th month: A) upper right central incisor in the dental arch, B) radiographic evaluation where a bony defect was observed around the upper right central incisor and the root dilacerations on the central and lateral incisors. The root of the upper right canine is almost completely formed and with a tendency towards impaction.
Fifteen days later the second surgery for the exposure of the upper canine was performed and a button was placed for the traction (Figure 11).

Two weeks following the withdrawal of sutures, the canine traction was begun with an elastic ligature tied to a 0.036 stainless steel accessory archwire fixed to the accessory tubes of the bands of the upper molars.
In the following appointment, the accessory arch was withdrawn; the arc and brackets were placed on canines and premolars that had already completed its eruption. A stainless steel 0.016×0.016 archwire was placed with a box bend to traction the canine with elastic ligature. In the lower arch a 0,016 NiTi archwire was placed (Figure 12).

The following month, a bracket was placed on the canine, and it was included in the 0.016 NiTi archwire in the upper arch.
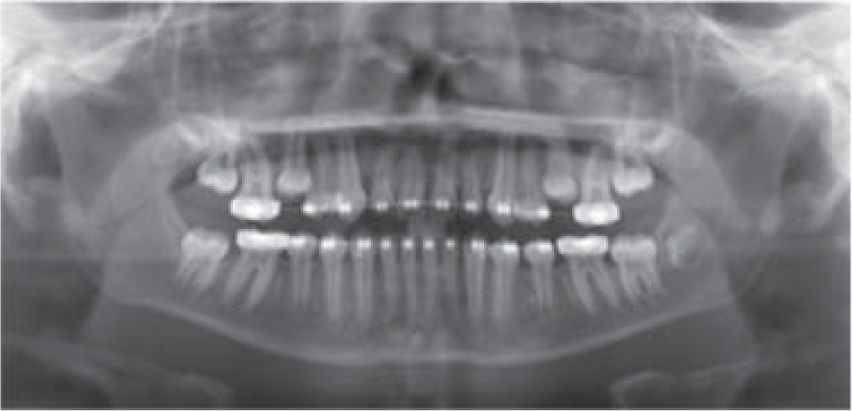
Two months later, a new control panoramic was requested, where it was observed a decrease of the bony defect around the upper right central incisor and good root parallelism. It was also noted the approximation of the second upper premolars to the oral cavity (Figure 13).

Three months later second upper premolars brackets were placed and the arch wire was placed over the brackets to extrude the premolars and get them closer to the oral cavity.
In the following appointment a 0.022 slot MBT bracket was placed in the upper right central incisor upside down to provide negative torque to the same tooth. 0.017×0.025 NiTi archwires were placed in both the upper and lower arches (Figure 14).
: the upper second premolars were completely erupted. A 0.022 MBT bracket was placed upside down on the upper right central incisor to provide negative torque. 0.017×0.025 NiTi archwires were placed.")
The following month, upper and lower 0.017×0.025 SS arches were placed with negative torque in the upper right central incisor.
In the next appointment 0.019×0.025 SS braided arches were placed on the upper and lower arch with triangular box elastics (1/8 heavy) for bite settling (Figure 15).
: Braided 0.019×0.025 upper and lower archwires with elastics for bite settling were placed.")
The patient completed her treatment in September 2012, with a treatment time of 25 months (Figure 16). Circumferential retainers were chosen for both arches.
Results upper right incisor and canine were aligned into the dental arch. Obtained molar and canine class I, B) obtention of ovoidal arch forms.")
The treatment was finished at 25 months of therapy, the position of the ectopic right upper central incisor was corrected and brought into the dental arch in the right position. The surgical exposure of the upper canine associated to the impaction of the central incisor was carried out in a second phase, as planned, achieving its correct alignment in the arch since radiographically it had already been identified a tendency towards impaction that was thought to be present from the start. We eliminated crowding and aligned the arches, obtaining molar and canine class I.
Oval arch forms and an acceptable overjet and overbite were achieved. For the case detailing, individual negative torque was applied in the upper right central incisor and the bite was settled (Figure 16).
In the facial aspect no significant changes have been found, since one of the original objectives was to obtain minimal profile changes given that it was acceptable from the start (Figure 17).

In the final panoramic radiograph appropriate root parallelism and integrity is noted in addition to healthy support tissues. In the lateral head film dental inclination is observed and an acceptable profile (Figures 18and19, Table II).


Before and after treatment cephalometric data.
| Angle | Norm | Initial | Final |
|---|---|---|---|
| S | 123°±5° | 112° | 115° |
| Ar | 143°±6° | 154° | 156° |
| Go/sup | 55°±3° | 51° | 43° |
| Go/inf | 75°±3° | 67° | 75° |
| Total | 396° | 384° | 389° |
| SNA | 80°±5° | 87° | 88° |
| SNB | 78°±5° | 85° | 87° |
| ANB | 2° | 2° | 1° |
| SN/GoGn | 32° | 26° | 29° |
| Go/GN/1 L | 90°±2° | 89° | 86° |
| SN/1 U | 102°±2° | 106° | 107° |
| Dental convexity | 130° | 129° | 135° |
| Upper lip | 1mm -4mm | 0mm | - 1mm |
| Lower lip | 0 to 2mm | + 1mm | 0mm |
| A.F.H. | 112mm | 95mm | 109mm |
| P.F.H. | 71mm | 67mm | 76mm |
| Ra L | 44mm±5mm | 36mm | 49mm |
| M B L. | 71mm±3mm | 64mm | 68mm |
| ACBL | 71mm±3mm | 58mm | 60mm |
| P.BCL | 32mm±3mm | 33mm | 34mm |
According to Ricketts’ 7 areas of superimposition the changes that have happened were observed in relation to the patient’s growth (Figure 20).
Discussion Ricketts superimposition: pretreatment and postreatment observed changes. It is observed that there was growth and minimal changes on the profile, B) 7 areas for assessment according to Ricketts: observed changes in the beginning and at the end of treatment.")
Injuries in the facial area are very common in childhood and with a high prevalence they affect the anterior maxillary area of the
oral cavity.1,2 According to some authors, one of every three children suffers from some type of trauma to the deciduous teeth of the anterior segment.2–4,8
Studies have shown that patients with a history of trauma in deciduous teeth presented intrusion, dilacerations and retention of permanent incisors as sequelae of trauma.2,3,8
According to several authors, the intrusive luxation of deciduous teeth may cause anomalies in the permanent dentition, due to the proximity between the apex of the deciduous tooth and the germ of the permanent tooth.2–4
This type of injury can cause rupture of the gingival margin seal, bruising of the alveolar bone and breakdown of the periodontal ligament fibers, of the cement and affect the nervous and vascular system provided by the pulp.2,5–7 When the germ of the permanent tooth is affected damage can be caused to the coronal portion of the tooth causing hypocalcification, enamel hypoplasia and alterations in the anatomy of the crown. At root level, duplication, dilacerations and interruption of root formation can occur.2,8,9 There can also be disorders in eruption, malformations similar to odontomas and impacted tooth germ.2,9,10
As could be observed in this patient, the consequences of trauma caused the retention of the permanent incisor and caused the tendency towards impactionof the canineonthesame side. When the incisor was tractioned and brought into the arch, it could be observed with more detail the root dilaceration of the central and lateral incisors radiographically observed as an increase in root angulation. When this disorder occurs in the period of tooth formation, there is a change in the position of the mineralized portion in relation to the structure that remains of the tooth.8,10 This curvature may occur at any development site of the tooth, depending on the stage of root formation when the trauma ocurrs.8–10 Trauma can affect the development of the tooth when it occurs between the ages of 4 to 6 years. At a younger age, the crown may be affected.8-10 It is important to mention the emotional impact that causes in the aesthetics the absence of an anterior tooth in children and adolescents and it becomes a challenge where the orthodontist must act in a timely manner.10
It was given to the patient’s parents different treatment options for the management of the retention of the central incisor, the inclination of the lateral incisor and the tendency towards impaction of the upper right canine. The first option was the removal of the central incisor and restoration with a provisional fixed or removable prosthesis until it could be rehabilitated with an implant. Another treatment option was the removal of the central incisor, alignment, leveling and space closure by replacement of the central incisor with the lateral incisor and subsequently include the canine in the arch. Afterwards, it would have been necessary to prosthetically restore the lateral incisor to match the anatomy of a central incisor. The last option, and the one the patient’s parents decided to perform, was that of the surgical exposure of the central incisor, space opening and orthodontic traction of the incisive and the canine as a conservative treatment option. The prognosis was reserved due to the inclination and the position of the upper right central incisor. This last option was successful for the patient. By being conservative the removal of a permanent tooth was prevented and the integrity of the tissues was maintained, so a long-term stability is expected.
ConclusionsThe following considerations must be taken into account while treating this type of cases:
- 1.
The solution of the impaction of a central incisor, the correction of the position of the lateral incisor and canine of the same side, must be carried out according to a proper diagnosis and treatment plan.
- 2.
At all times the position of the canine should be monitored radiographically due to the tendency towards impaction that occurs in these cases. Patients with impacted central incisors should be informed of the possibility of the impaction of the upper canine of the same side and that it requires monitoring.
- 3.
Treatment of impacted incisors with dilacerated roots is a clinical challenge, since the acquisition of negative torque is not expressed in an appropriate manner if the root of the adjacent teeth is superimposed. When the dilaceration is severe, it may require endodontics and apicectomy to provide the required torque and proper alignment.
- 4.
The subsequent radiographic and clinical analysis of stability and periodontal health of the incisor with a dilacerated root is very important after orthodontic traction and even after the removal of the appliances.