




















The goal of any orthodontic treatment is to achieve the desired movement of the teeth with minimal side effects. Mini-implants have biomechanical advantages that promote a more effective and efficient treatment. The use of orthodontic mini-implants for orthopedic maxillary expansion can considerably reduce undesired tooth movement. A clinical case report of a 13-year-old female who was diagnosed with a collapsed maxilla and treated with an acrylic device with an expansion screw anchored to two mini-implants placed in the palate and in the first molar for the expansion of the maxilla. The aim of this clinical case study was to analyze the separation of the maxillary suture by using orthodontic mini-implants, evaluate the transversal changes at the skeletal and dental level and the secondary effects induced in the teeth used as anchorage. Skeletal changes achieved in the patient treated with mini-implants were: maxillary width increased 3mm; regarding the dental changes, an increase in the intercanine distance of 3mm and an 8mm increase in the interpremolar and intermolar distance were observed. The secondary effect caused to anchorage teeth was buccal tipping of the first molars; in average, the right molar 1° and the left molar 4°. Orthodontic mini-implants are a reliable source for orthopedic anchorage since they provide acceptable skeletal changes with minimal side effects in teeth used as anchorage.
La meta de cualquier tratamiento ortodóncico es lograr el movimiento deseado de los dientes con un mínimo de efectos secundarios. Los miniimplantes proveen ventajas biomecánicas que permiten realizar un tratamiento más efectivo y eficiente. El uso de los miniimplantes ortodóncicos para la expansión ortopédica del maxilar puede reducir considerablemente el movimiento indeseable de los dientes. Se presenta el caso clínico de una paciente femenina de 13 años de edad con diagnóstico de maxilar colapsado, tratado con un dispositivo de acrílico con un tornillo de expansión, el cual fue anclado a dos miniimplantes colocados en el paladar y a los primeros molares para hacer la expansión del maxilar. El objetivo de este estudio del caso clínico fue analizar la separación de la sutura maxilar con el uso de los miniimplantes ortodóncicos, evaluando los cambios transversales a nivel esqueletal y dental, así como los efectos secundarios provocados en los dientes usados como anclaje. Los resultados esqueletales logrados en la paciente tratados con miniimplantes fueron: el ancho maxilar aumentó 3mm; con lo que respecta a los cambios dentales hubo un incremento de 3mm en la distancia intercanina y de 8mm en la distancia interpremolar e intermolar respectivamente. El efecto secundario provocado en los dientes usados como anclaje fue la vestibularización de los primeros molares; en promedio, el derecho se vestibularizó en 1° y el izquierdo en 4°.
ConclusiónLos miniimplantes ortodóncicos son una fuente confiable de anclaje ortopédico, ya que con ellos se pueden lograr cambios esqueletales aceptables con un mínimo de efectos secundarios en los dientes usados como anclaje.
In recent years, Implantology has been one of the areas with more growth in Odontology. Dental implants are useful tools in the study of mechanically-induced bone modeling and remodeling and are used to move bones of the craniofacial skeleton.1
In 1997, Kanomi2 stated the use of 1mm in diameter and 5mm length titanium mini-implants (Leibinger®, Freiburg, Germany) as orthodontic anchorage. This author considered that implants for orthodontic purposes must be small enough to be placed in any bone area and that the surgical procedure should be simple enough for the orthodontist to perform and they must be easy to remove.2 Afterwards, the Food and Drug Administration (FDA) approved the use of titanium mini-implants as orthodontic anchorage and in 2005, fifteen mini-implant systems were available in the market.
During the last few years, titanium mini-implants have been widely used in orthodontic treatment specially to provide absolute anchorage without the need of patient cooperation. These mini-implants can be loaded immediately because osseointegration is not needed beforehand and its cost is less than conventional implants.3–5
Mini-implants consist of a screwed endo-osseus section, a transmucous neck and a head; the most widely used forms are the cylindrical and the conic cylindrical with a 2-3mm diameter and a length that can vary from 6 to 14mm and an external 2mm band length. Some mini-implants have an internal and external slot to make ligation easy. Implant surfaces sometimes are treated to create rough areas that increase the osseintegrated area. These mini-implants may bear a load that ranges from 1 to 3 N (< 300 g).1,4,6
Placement site selection is critical and requires careful consideration of the hard and soft tissues, therapeutic indications, biomechanic needs, accessibility and patient’s comfort. From an orthodontic point of view alveolar bone, the retromolar area, maxillary tuberosity and the palate are the most frequently used areas to insert mini-implants.1,3,6
Mini-implants for orthopedic expansion must be placed in paramedical areas of the maxillary suture.3 Relatively low load forces (1 to 3 N) applied over endo- osseous implants inserted around the suture are ideal to perform expansion.7
There are three problems related to the correction of a collapsed maxilla: first is unwanted movement of anchorage teeth (molar buccal movement increasing the risk for dehiscences, gingival recessions and traumatic occlusion), second is the increase in vertical growth (especially in hyperdivergent patients) and the third one is to obtain a separation of the medial palatal suture in adult patients. Skeletal anchorage might help in solving those problems. However, more research is needed to establish a treatment protocol for orthopedic maxillary expansion using mini- implants.3,7
Case reportDiagnosisFemale patient, 12 years and eleven months old was referred to the Orthodontic Clinic of the Postgraduate Studies and Research Division of the Dental School at the National University of Mexico because she presented severe upper dental crowding.While answeringthe clinicalhistory it was found that she was in good health. Upon intraoral examination no pathological signs were observed and no pain or noises in the temporomandibular joint were registered.
Facial analysis revealed a dolicofacial patient with convex profile and depressed middle third (Figure 1); while in intraoral photographs (Figure 2) a bilateral molar class II is observed, canine class is not assessable o the right side and on the left side, there is a canine class II, a 2mm overjet and overbite is present and there is a right unilateral posterior crossbite and severe crowding in the upper anterior segment.


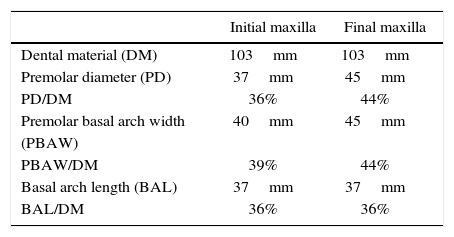
Howes8 analysis was performed since it relates dental size with the supporting structures (Figure 3andTable I) and due to the fact that the premolar basal arch width compared to the dental material was bigger than the premolar diameter, maxillary dental expansion can be considered.

In the panoramic radiograph (Figure 4) a 1:1 crown-root ratio is observed in most teeth (except in upper canines and molars), infraocclusion and short root of the lower right second premolar, four third molar dental germs and normal periodontal structures.

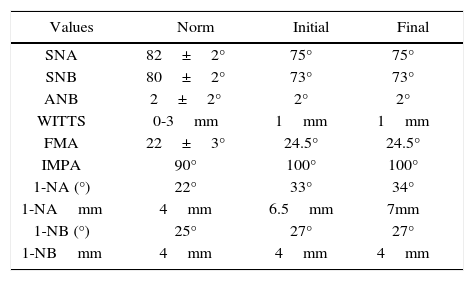
Cephalometric analysis revealed that the patient has a biretrusive skeletal class I, neutral growth biproclinations and upper dentoalveolar protrusion (Figure 5andTable II).

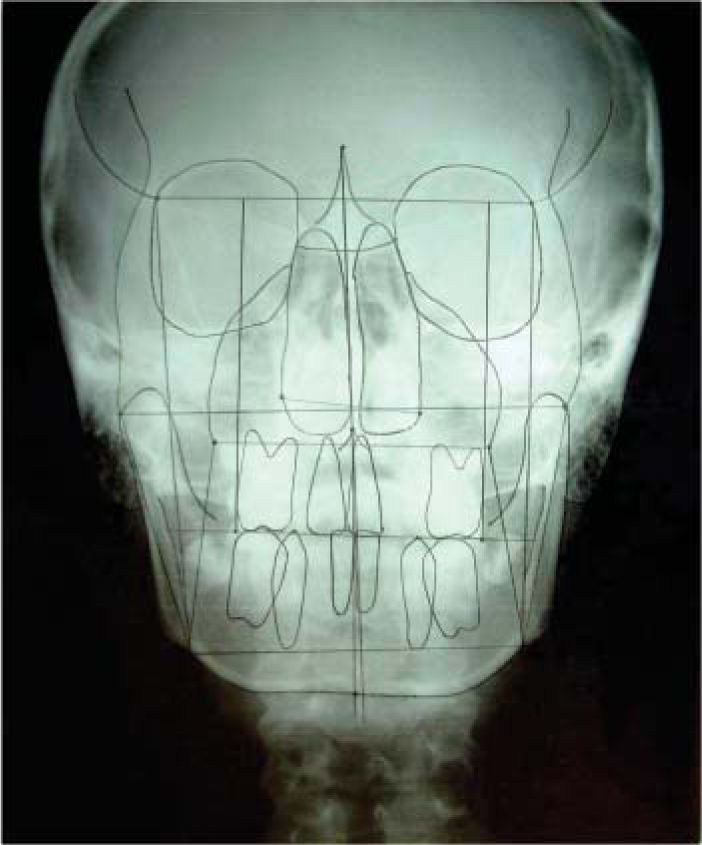
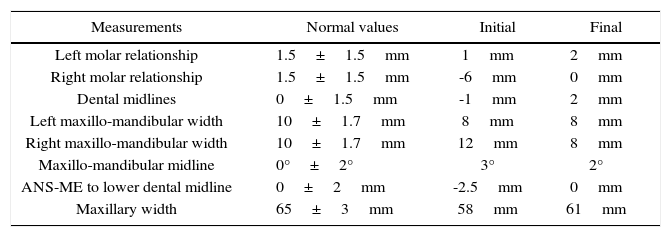
Posteroanterior radiographic analysis (Figures 19 and Table III) revealed that the patient has a collapsed maxilla, unilateral right posterior crossbite, non-matching dental midlines and mandibular deviation to the right.
Cephalometric values of the posteroanterior radiograph.
| Measurements | Normal values | Initial | Final |
|---|---|---|---|
| Left molar relationship | 1.5±1.5mm | 1mm | 2mm |
| Right molar relationship | 1.5±1.5mm | -6mm | 0mm |
| Dental midlines | 0±1.5mm | -1mm | 2mm |
| Left maxillo-mandibular width | 10±1.7mm | 8mm | 8mm |
| Right maxillo-mandibular width | 10±1.7mm | 12mm | 8mm |
| Maxillo-mandibular midline | 0°±2° | 3° | 2° |
| ANS-ME to lower dental midline | 0±2mm | -2.5mm | 0mm |
| Maxillary width | 65±3mm | 58mm | 61mm |
According to the obtained diagnosis, it was decided to perform a first treatment stage with maxillary orthopedic expansion to correct the collapse and a second treatment stage with fixed appliances to correct the dental problems.
Alternative treatmentsA collapsed maxilla may be treated with a Hyrax screw welded to bands or with a McNamara or Hass type expander. However in this case it was decided to treat the patient with an acrylic device with an expansion screw anchored by two mini-implants placed on the palate and to the molars to try to minimize the side effects that the before mentioned expanders have.
Treatment progressThe present article only describes the maxillary orthopedic expansion stage with two orthodontic mini-implants in the paramedian areas of the palatal suture.
Treatment was initiated by placing two mini-implants in the paramedian areas of the maxillary suture under sterile conditions and local anesthesia. The miniimplants used were 2.5×1.6×6mm self-thread Orthodontic Skeletal Anchorage System (OSAS de Dewimed®) (Figure 6).

After implant placement, impressions were taken with bands placed on the first molars to fabricate the acrylic appliance that contained the 7mm Hyrax screw (Dentaurum®). The appliance was cemented one week after implant placement and the miniimplants were embedded with fluid resin (Tetric Flow de Ivoclar®) (Figure 7).

Once the appliance was in place, the patient was given instructions to activate the screw 1/4 turn by night during three weeks and because it was observed that the force was insufficient, it was decided to activate 1/4 turn in the morning and 1/4 turn by night for two weeks. The length of the expansion screw was not enough so on week seven of treatment the appliance was removed and a rigid 0.060” vacuum-formed retainer and a week later the new appliance was placed with a new screw. The screw as activated during two more weeks, 1/4 turn in the morning and 1/4 turn by night. During this seven-week period records were taken with occlusal radiographs (one per week) and with study models (initial and final).
After expansion was achieved, the appliance was removed and a welded transpalatal arch was placed as anchorage.
ResultsThe obtained results were analyzed comparing intraoral photographs, dental study models, and radiographs (occlusal, lateral and posteroanterior) before and after the orthopedic maxillary expansion.
Extraoral photographs: facial changes are observed at smile where a transverse development of the upper arch can be observed and in the 3/4 photograph where the depressed middle third was improved (Figure 8).

Intraoral photographs: when comparing the occlusal photographs a transverse development of the arch can be observed and a 5mm increase in the inter-implant distance (Figures 9and10).


On the frontal and right lateral photograph a correction of the posterior crossbite was observed and the 2mm overbite was maintained (Figure 11).

Study models: When comparing the occlusal transverse measurements in the models (fossa to fossa) an 8mm increase was observed in the interpremolar and intermolar distance (Figure 12).
.")
At the comparison of the occlusal measurements in the models (cuspid-cuspid) a 3mm increase was observed in the intercanine distance and an increase of 8mm in the interpremolar and intermolar distance, these measurements agree with the ones taken fossa to fossa (Figure 13).
.")
In Howes analysis, an increase in the premolar diameter and a 5mm increase in the premolar basal arch width were observed (Table I).
The first molar’s buccal inclination was measured in the study models taking as a reference the method described by Oktay and Kiliç (2007).9 These authors add a fine line (1mm diameter) of barium sulfate solution that passes through the following structures:
- •
Gingival margin, mesio-bucal and mesio-palatal cusps of the upper right first premolar.
- •
Palatal vault.
- •
Mesio-palatal and mesio-bucal cusps and gingival margin of the upper left first molar.
After this procedure, they take a radiograph of the model and perform the measurements on it.
On this clinical case, the assessment of the buccal inclination of the first molars was performed directly over standardized photographs of the study models.
The reference points and planes used were:
- •
Tip of the mesio-buccal right and left cusp.
- •
Tip of the mesio-palatal right and left cusp.
- •
Right plane, line that passes the tip of the mesio-buccal cusp to the mesio-palatal cusp of the right molar.
- •
Left plane, line that goes through the tip of the mesio-buccal cusp to the mesio-palatal cusp of the left molar (α1 y α2) are the internal angles formed between the occlusal plane and the right and left plane respectively that determine the buccal inclination of the first molars. The right molar did not incline bucally while the left molar suffered a 6° inclination (Figures 14and15).


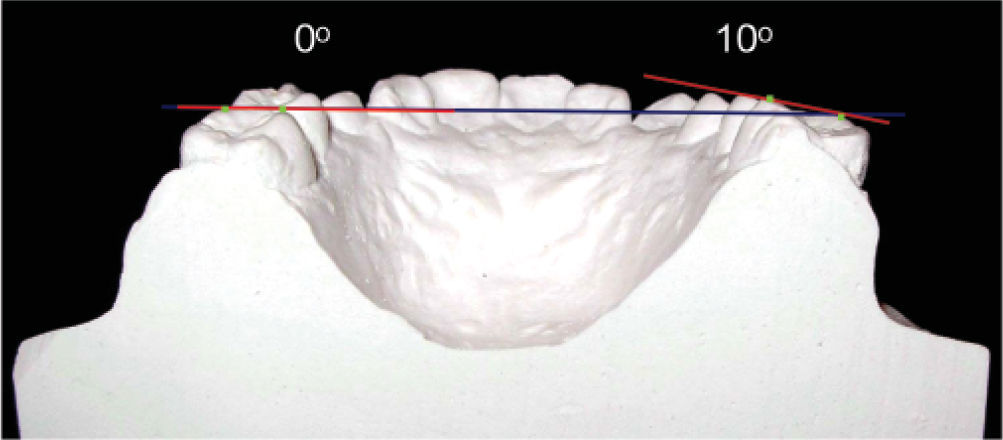
Another measurement of the study models was made to assess the buccal inclination of the first molars taking as a reference a horizontal plane that passed over the occlusal surfaces of the second molars since those teeth were not used as anchorage; and two vertical planes, one that passed over the buccal surface of the right first molar and another one that passed over the buccal surface of the left first molar. The external angles formed between the horizontal plane and the vertical ones were measured. The right molar tilted 1° and the left one, 2° (Figures 16and17).


Occlusal radiographs: the opening of the maxillary suture is observed. It was achieved in weeks 4 and 5 (Figure 18).

Lateral cephalogram: it revealed that there was no modification of the A point which means that there were no anteroposterior skeletal changes, the FMA angle remained constant with 24.5° which suggests that there was vertical growth control and the upper incisor only proclined 1° (Table II).
Anteroposterior radiograph: it shows that the maxillary width increased 3mm (Table III, Figures 19and20).
Discussion

Orthodontic mini-implants provide biomechanic advantages that permit a more effective and efficient treatment. These advantages have been reported and documented in the literature on many articles that describe this, especially in relation to absolute anchorage, anterior segment retraction, molar distalization, intrusion or extrusion movements, etc. However there are few articles in the literature that describe orthopedic maxillary expansion.
Orthodontic mini-implants may resolve three classic problems regarding a collapsed maxilla: first they can reduce unwanted movement of the anchorage teeth (molar buccal inclination which can increase the risk for dehiscences, gingival recessions and traumatic occlusion); second, they can accomplish a vertical growth control (especially in hyperdivergent patients) and third, they can achieve the separation of the midpalatal suture in some adult patients.3 Skeletal anchorage might be useful at solving these problems. Nevertheless, more research is needed to establish a treatment protocol for orthopedic maxillary expansion with mini-implants.3,7
Lee and his team in 2007 described a case report of a 20-year-old female patient with anterior open bite, prominent chin, facial asymmetry and severe maxillary collapse who was treated with rapid palatal expansion and surgery to correct the skeletal discrepancy. Rapid maxillary expansion was performed using four mini-implants placed in the palate (two at premolar level and the other two between the first and second molar). The anchorage teeth were the canines and the first molars, to which arms were welded to connect them to the mini-implants through resin; the expansion screw was welded to the arms but not to the mini-implants. After two months, the maxillary arch was expanded with good results. Cephalometric analysis of the posteroanterior radiograph showed that the maxillary width increased 4mm.
A very interesting fact about this case is that it showed that orthopedic expansion could be performed in a patient that had finished growing, however further research in that matter is needed.
The obtained results in this clinical case match the results achieved by Lee and his collaborators since in both cases the maxillary suture opened in approximately one month, orthopedic expansion of the maxilla was accomplished in two months and the maxillary width increased 3 to 4mm. However in the case presented by Lee and his group they only mention transverse skeletal changes and the advantage of the present case is that it additionally shows the cephalometric analysis of the lateral head film, which reveals that there were no changes in the vertical dimension since the FMA remained stable. Dental changes are also presented.
Wilmes and his team in 2010 assessed dental and skeletal effects caused by rapid maxillary expansion in 13 patients (seven females and six males, with an average age of 11.2 years). The patients were treated with a Hyrax screw anchored anteriorly to two mini-implants placed on the palate (at premolar level) and on the posterior region, to the first molars. They also used a facial mask for maxillary protraction. The evaluation of the dental changes was performed with scanned study models that were superimposed digitally. Necessary time for expansion was 4 to 14 days (average 8.7 days). The average for expansion in the first premolar region was 6.3±2.9mm and 5.0±1.5mm in the molar region. According to the results reported by Wilmes and his partners, maxillary expansion was achieved in less time compared to the present case; however expansion in the premolar and molar region was 8mm. Further studies are needed in this area to confirm or not these results.
ConclusionsThe use of orthodontic mini-implants for orthopedic expansion of the maxilla is a reliable source for orthopedic anchorage. Through mini-implants acceptable skeletal changes may be achieved with minimal side effects in anchorage teeth.
Several problems related to mini-implants have not been solved due to their short use in the history of orthodontic treatments so long term data are insufficient. Because of this, further investigation is required, particularly in relation to orthopedic applications.