







Diagnostic indexes are important to predict dental arch size and to suggest the most appropriate treatment plan for each patient. Pont designed a method to determine the width of an ideal dental arch, based on the mesiodistal measurements of the crowns of the upper incisor; besides he provided formulas to obtain norms. The purpose of this study was to determine if Pont’s index norms match the results obtained after non-extraction orthodontic treatment. A cross-sectional, descriptive and comparative study was performed to 54 study models. The statistical analysis showed that there’s a significant difference between Pont’s index norms and the measurements obtained from the models.
Los índices para diagnóstico son importantes para predecir el tamaño del arco dental y proponer el plan de tratamiento más adecuado para cada paciente. Pont, diseñó un método para determinar el ancho de un arco ideal, basado en las medidas mesiodistales de las coronas de los incisivos superiores; además proporcionó fórmulas para obtener normas. El objetivo de este estudio fue determinar si las normas del índice de Pont son iguales a los resultados obtenidos después de un tratamiento de ortodoncia sin extracciones. Se realizó un estudio transversal, descriptivo y comparativo a 54 modelos de estudio. El análisis estadístico mostró que existe diferencia estadísticamente signifi cativa entre las normas del índice de Pont y las mediciones obtenidas en los modelos.
Many malocclusions are a direct result of inheritance although similarities cannot always be estimated between parents and offspring because frequently, the parents have already lost dental organs when making a comparative evaluation between dentitions. There are basically two general factors considered which can contribute to similarities between relatives: genetic factors and environmental factors.1
However, the etiology of crowding or interdental spacing is not fully understood. Hooton suggested that crowding was probably the result of an evolution trend towards a more reduced size of the facial skeleton without the corresponding decrease in dental size. Brash stated that hereditary crowding was the result of a mixture between races or ethnic groups that were not physically similar. Other investigators suggested that environmental factors such as a soft diet or loss of arch length due to caries were more important than genetic factors. 2,3
The truth is that crowding is the result of a discrepancy between the combined width of teeth and the arch perimeter and that this depends on numerous factors such as shape, length and width.4,5 Let’s recall that in the mixed dentition stage there is usually an increase in dental and alveolar arch width in the anterior region as the permanent incisors erupt.6
There is a great variety of indexes for clinical orthodontic diagnosis used to predict the size of the dental arch and help us choose the treatment plan more suited for each case.1 All of this due to the fact that dental crowding may be related to arch width or length with disproportionately big teeth or a combination of factors.
For orthodontic diagnosis study models are of the outmost importance and also the analysis that are applied to them to obtain an adequate dental relationship on their basal bones and also, their intermaxillary relationships.
Numerous indexes have been suggested as a guide for the clinician to determine the amount of expansion required to achieve an ideal arch width.5 Thanks to study model analysis dental arches can be studied.6 The importance of this evaluation method for the maxillary orthopedic diagnosis and treatment planning has been overrated in the past. The disadvantage of odontometry is that it is basically a correlation analysis in which the dental arch width and length are evaluated mathematically in relation to tooth size.
There is a certain correlation between the dental arch length, its width and the mesiodistal dental material that has been defined by several authors by means of indexes. The most commonly used in German speaking countries are the Pont’s, Linder’s, Harth’s and Korkhaus’ analysis. This kind of analysis compare the value of each case with the classical value of normal dentitions.7–9 In more recent years, some authors have considered that this method has little diagnostic usefulness. However, in spite of all the criticism to prevent them from being applied, it is still widely used in the maxillary orthopedic practice.9 Nevertheless, it is convenient to remember that the determination of the discrepancy between tooth size and arch length requires a more or less precise prediction of the mesiodistal width of the permanent dentition, in this case, the four upper incisors.10
It is expected that during orthodontic treatment every tooth will be aligned in such a way that the combined widths of the teeth will be identical to the dental arch and that it will be well positioned in the basal bone,11 always avoiding overexpansion which frequently relapses.12
The marked differences between the dental arch, the basal arch and the alveolar arch perimeters must not affect the esthetics or compromise the function and occlusal stability.
Study model analysis consists then in studying the space in the dental arch in the three planes of space in the upper and lower arches as well as the intermaxillary relationships.13 One of the great advantages of study model analysis is that it makes it possible to detect the deviations of disgnathias.14
It was in 1909 when Pont (and Izard as well)15 designed a method to determine the width of an ideal arch based on the mesiodistal widths of the upper incisor’s crowns. Pont suggested that the relationship between the incisal arch width combined with the transverse width (measured from the center of the occlusal surface of teeth) was ideally 0.8 in the premolar area and 0.64 in the first molar area.16
The theoretical value of the transverse width of the dental arch at the premolar and molar region depends, as it has been mentioned before, on the mesiodistal width of the four upper incisors.
The odontometric measurement points of the anterior and posterior width of the dental arch are one before the other in a case with proper occlusion in the upper maxilla and in the mandible, and they must be identical for both bones.2
The comparison of the theoretical value with the real value shows the standard deviations i.e. the cases of narrowness or excessive width of the dental arch.
The dental arch length is defined according to Korkhaus as the apothem directed from the labial of the central incisors to the connecting line of the measurement points that determine the anterior width of the dental arch. This measurement shows the sagittal position anomalies of the anterior teeth.2
In Pont’s analysis the theoretical values of the dental arch length are statistical correlational values that depend on the mesiodistal sum of the upper incisors. The mandibular sagittal length is usually 2mm shorter than the length of the upper maxilla. The anterior arch length is not only modified by the ill -position of the anterior teeth but also by the anomalies in the position of the first premolars. The correlation between the length and width of the dental arch is subject of great variation and changes according to facial shape. Hawley in 190414 recommended that the combined width of the six anterior teeth could be used as a circle’s ratio and that the teeth should be placed in that circle. Such construction would then help establish the facial shape but Angle recognized that a parabolic curve was a better option for arch form while also mentioning that «the best thing that an orthodontist can do is to establish normal relations between teeth and correct the general arch form, leaving each individual’s precise adjustment to natural forces which at the end, must prevail».
It is important to remember that Pont’s Index was established on French population only.4,9 Pont also suggested that there is a correlation between the shape of the skull (dolico, meso and brachycephalic) and the dental arch shape.
Nowadays the use of Pont’s Index remains, some professionals depend on it to determine the correct arch width and at the Orthodontic clinic of the Postgraduate Studies and Research Division at UNAM it is frequently used. Due to the fact that it has been recently suggested that this diagnostic method is of little use, it is important to know how convenient it is to apply a study model analysis according to the Pont’s Index considering that the values used in this analysis for an adequate arch width and length are related to the final results of orthodontic treatment.
Este documento es elaborado por Medigraphic Investigators from the University of Washington applied the Pont’s Index to patients who had received complete orthodontic treatment and abandoned retention for at least 10 years. No permanent tooth had been extracted in any of the patients. There were very poor correlations between the combined widths of the upper incisors and the final arch width in the premolar and molar areas and they came to the conclusion that measuring the mesiodistal widths of the incisors to determine the upper bimolar and intercanine widths has no value.3
Likewise, Stiffer tested the Pont’s Index in ideal Class I occlusions and reported no relationship between the Index and the molar and premolar width.5 In an evaluation of Pont’s Index Joondeph et al reported that in 20 subjects 10 years postretention there was poor correlation with Pont’s Index. Similar results were obtained by Worm et al, who examined 91 Navajo children and 133 dental students with ideal occlusions and less than 1mm crowding or spacing.5
It is due to all this facts that the interest to evaluate the study models of patients who finished a non-extraction orthodontic treatment emerged and to compare the numbers that the Pont’s Index determines as normal with the dental arch width and length of those same patients in such a way that similarities can be appraised with the Index so that its clinical use can be estimated.
The purpose of this investigation was to obtain the dental arch length, anterior and posterior width from study models at the end of a non-extraction orthodontic treatment to determine if the values of Pont’s Index are equal to the results obtained after orthodontic treatment.
MethodsThis study was transverse, descriptive and comparative. The sample consisted in study models of patients who finished a non-extraction orthodontic treatment from the years 1995 to 2000; the inclusion criteria consisted in selecting only study models with non-extraction finished orthodontic treatment, with no fractures. Models that presented characteristics such as supernumerary teeth, anodonthia, atypical tooth shape (conic, triangular or amorphous), microdonthia or macrodonthia were excluded. The sample finally consisted in 54 study models.
The variables taken into consideration were upper incisor sum, posterior dental arch width, dental arch length and anterior dental arch width. The values for Pont’s Index are based on the mesiodistal width of the upper incisors combining them with the molar and premolar transverse width. The equation for calculating Pont’s Index is:
- •
Anterior width:
Incisal sum x 100/85
- •
Posterior width:
Incisal sum x 100/65
- •
Dental arch length:
Incisal sum x 100/160
The comparison of the recollected data consisted in obtaining the incisal sum of the selected study models and with the equations suggested by Pont, the anterior dental arch width, the posterior dental arch width and the dental arch length were obtained.
Subsequently, real measurements were taken from the study models. The statistical method used was Student’s t.
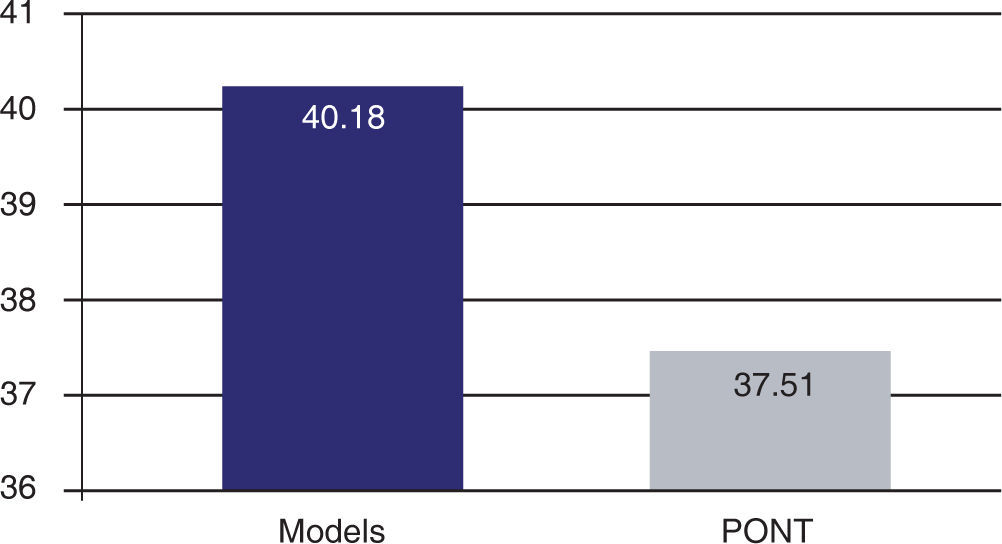
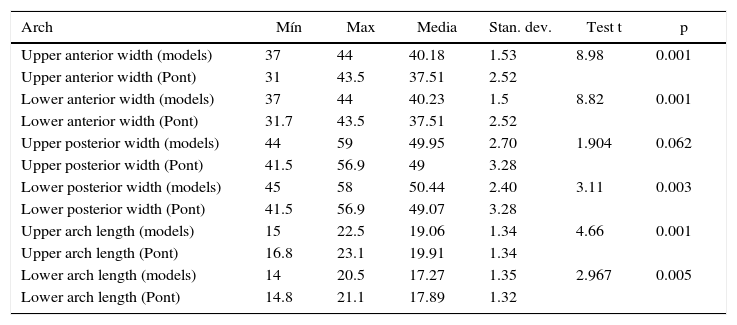
ResultsOn these variables it was discovered that there was a statistically significant difference between the study models and Pont’s Index (Figures 1-6).






The only case that showed no difference at 0.05 was the upper posterior width but it will be considered that p=0.065 is still statistically significant in this study (Table I).
Results.
| Arch | Mín | Max | Media | Stan. dev. | Test t | p |
|---|---|---|---|---|---|---|
| Upper anterior width (models) | 37 | 44 | 40.18 | 1.53 | 8.98 | 0.001 |
| Upper anterior width (Pont) | 31 | 43.5 | 37.51 | 2.52 | ||
| Lower anterior width (models) | 37 | 44 | 40.23 | 1.5 | 8.82 | 0.001 |
| Lower anterior width (Pont) | 31.7 | 43.5 | 37.51 | 2.52 | ||
| Upper posterior width (models) | 44 | 59 | 49.95 | 2.70 | 1.904 | 0.062 |
| Upper posterior width (Pont) | 41.5 | 56.9 | 49 | 3.28 | ||
| Lower posterior width (models) | 45 | 58 | 50.44 | 2.40 | 3.11 | 0.003 |
| Lower posterior width (Pont) | 41.5 | 56.9 | 49.07 | 3.28 | ||
| Upper arch length (models) | 15 | 22.5 | 19.06 | 1.34 | 4.66 | 0.001 |
| Upper arch length (Pont) | 16.8 | 23.1 | 19.91 | 1.34 | ||
| Lower arch length (models) | 14 | 20.5 | 17.27 | 1.35 | 2.967 | 0.005 |
| Lower arch length (Pont) | 14.8 | 21.1 | 17.89 | 1.32 |
The measurement of teeth has captured the attention of anthropologists and dental surgeons specially orthodontists who see in it the possibility of an exact and objective appraisal of dental variation. However, the reduced dimensions of the dental structures and crown wear entail not very precise measurements, they depend on the subject’s age and therefore, on the type of dietary habits of different populations in different eras.
Frequently, the problems that orthodontists have to face are due to a space discrepancy between the size of the maxillary bones and the tooth size and therefore, an analysis before beginning treatment is required.
There are several study model analysis but the disadvantage of odontometry is that it is essentially an exhaustive correlation analysis in which the dental arch length and width are mathematically evaluated regarding tooth sixe, just like the Pont’s Index does.
In this study, the anterior width (at premolar region) the posterior width (molars) and the dental arch length in study models of finished non-extraction orthodontic patients were measured. It was proven that there is a difference between the transverse arch length and the normal values suggested by Pont’s Index due to the anthropomorphic differences between races as it was previously demonstrated by Dalidjan and Joondeph; therefore, for our (mestizo) population, Pont’s Index is poorly applicable.
ConclusionsThe many advantages of study model analysis make it possible to detect deviations of the disgnathias (anomalies of the oral cavity and teeth that also affect the maxillary bones) in the three dimensions of space.
The lack of coincidence of the suggested values of Pont’s Index is due to the fact that the arch size of our population is broader than the one suggested by Pont. This reflects the need to design an index with such characteristics but performed in a similar population to the one that it will be applied on.
It is important to remember that racial variations also exist in teeth so Pont’s analysis may be considered an approximate guide to perform follow-up and control of the transverse dimension of the dental arch (mainly in the mixed dentition).
At the end of orthodontic treatment the most important thing is that every tooth is aligned and well-positioned in its basal bone while obtaining a good occlusal relationship that provides occlusal and esthetic stability.