
















Cleft lip and palate is the most common craniofacial malformation of the world's population, causing a great impact on society since it compromises both aesthetics and function. Presurgical orthopedic treatment at an early age limits the consequences of this anomaly.
ObjectiveTo describe two cases of male newborn patients diagnosed with unilateral and bilateral cleft lip and palate that underwent early pre-surgical orthopedic treatment.
MethodsInitially Friedman's stimulation plate was used to confront the alveolar ridges less than 5mm to continue subsequently with the formation of the nasal wings which were depressed.
ResultsThe alveolar fissures were closed completely in both cases in addition to lengthening the columella, increasing the size of the depressed nostril, as well as improving the perioral muscle tone thus enhancing the results of the cheiloplasty.
ConclusionsEarly preoperative treatment in infant patients with cleft lip and palate is a successful alternative for achieving closure of lip-alveolar-palatal clefts, with the aid of a skilled operator and committed to treatment parents.
El labio y paladar hendidos es la malformación craneofacial más común en la población mundial, causando un gran impacto en la sociedad porque compromete tanto la parte estética como funcional. La ortopedia prequirúrgica es un tratamiento que interviene en edades tempranas para la disminución de las secuelas de esta anomalía.
ObjetivoDescribir dos casos de pacientes género masculino recién nacidos con diagnóstico de labio y paladar hendidos unilateral y bilateral completo a quiénes se les realizó tratamiento temprano con ortopedia prequirúrgica.
MétodosSe utilizó inicialmente placa estimuladora de Friedman para afrontar los procesos alveolares a menos de 5mm, para continuar posteriormente con la conformación de las alas nasales que se encontraron deprimidas.
ResultadosSe cerraron las fisuras alveolares completamente en ambos casos, se estimuló el cierre de la fisura del paladar, además de elongar la columnela, aumentar el tamaño de la ventana de la nariz que se encontró deprimida y se logró la tonicidad muscular perioral adecuada para mejorar los resultados de la queiloplastia.
ConclusionesEl tratamiento temprano prequirúrgico en los pacientes recién nacidos con labio y paladar hendidos, es una alternativa exitosa en el cierre de la fisura labio alveolopalatina, con la ayuda de un operador habilidoso y unos padres comprometidos con el tratamiento.
Cleft and lip palate is the craniofacial anomaly with the highest incidence; it represents approximately 1:500 of global population and in Mexico, 1:700 alive newborns,1,2 depending on racial and geographic conditions. These malformations are defects that compromise both the anatomical and functional part with great aesthetic involvement. Additionally, the psychological component influences the family and social environment. The etiological basis of this disorder includes the interaction of several factors such as: drug ingestion in the first trimester of pregnancy (anticonvulsants, benzodiazepines, salicylates); infectious factors such as viral and bacterial diseases; nutritional deficits and irradiation which has demonstrated its teratogenic effect.
Pre-surgical orthopedics has evolved and improved with the passage of time. According to clinical results in the long term, interdisciplinary work has brought a significant reduction in the sequelae of the LPH because orthopedics diminishes the aesthetic and functional complications that these patients suffer from.
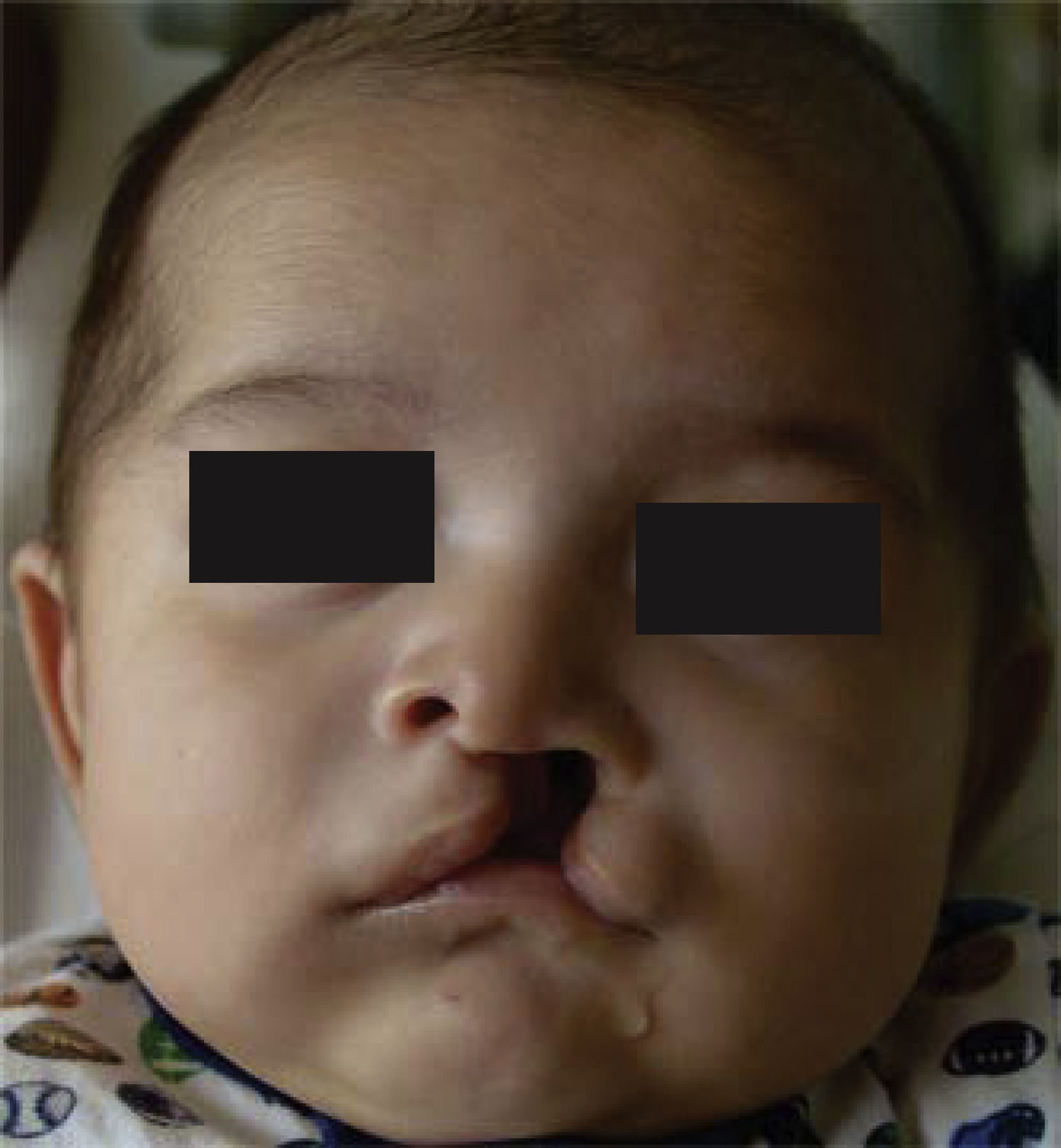
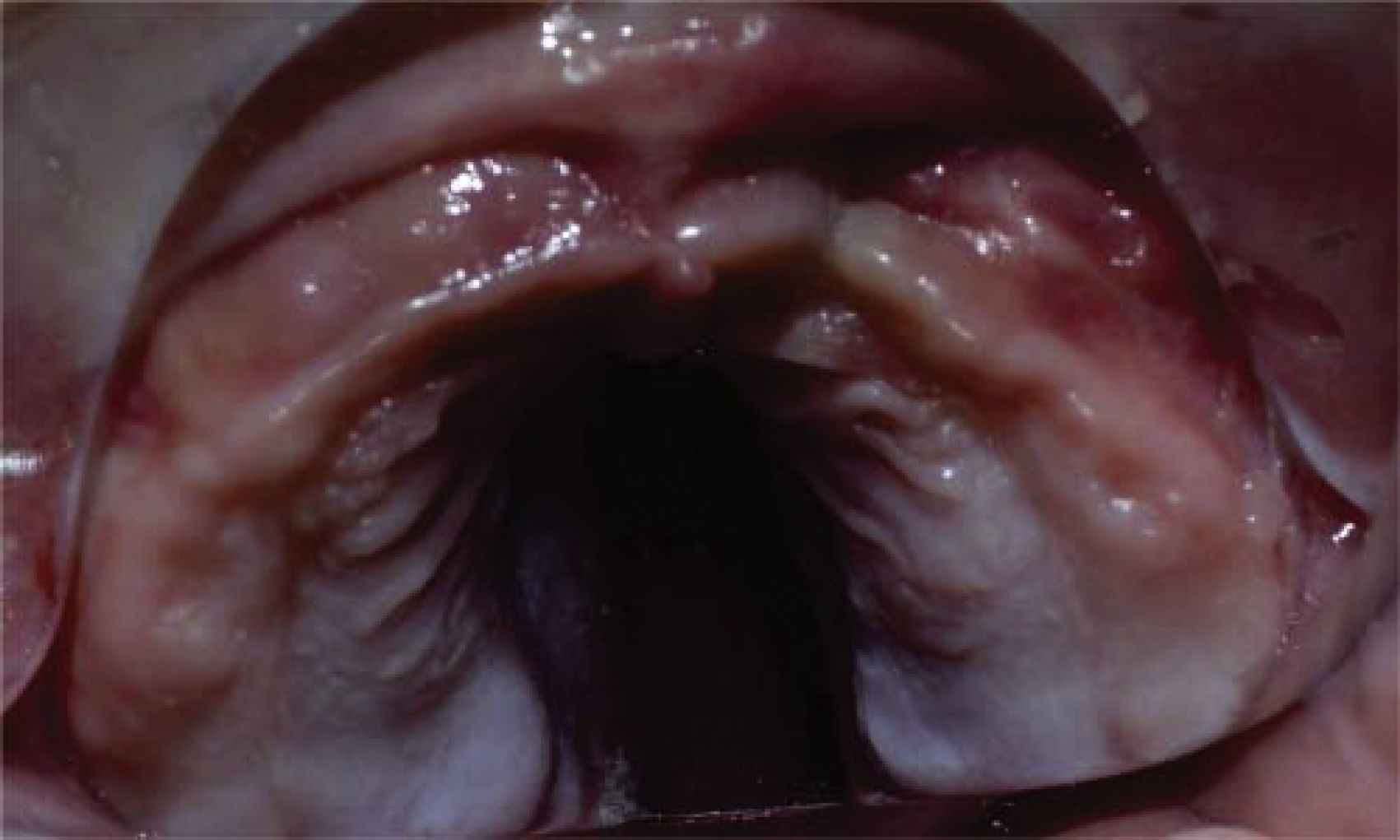
METHODSCase 1DiagnosisMale patient diagnosed with unilateral cleft lip and palate, who was brought in for consultation to the Clinic of Craniofacial Anomalies of the Center of Medical Specialties of the State of Veracruz «Dr. Rafael Lucio» (CEMEV). Upon clinical examination a 15mm complete alveolar-palatal-lip cleft, depression of the wing of the nose on the left side, a short and asymmetrical columnella and cleft palate with exposure of the vomer bone was observed (Figures 1-3).
Treatment goals


To shape the alveolar process and nostril, to move the concha major is towards the concha minor, to decrease the size of the alveolo-palatal fissure, to decrease complications during cheiloplasty and to improve the perioral musculature tone.
Treatment planThe patient's parents signed an informed consent where the diagnosis, treatment plan and possible complications were specified. The treatment plan consisted in obtaining an impression with condensation silicone in order to manufacture a Friedman obturator that would be used until the fissure decreased to less than 5mm. Then, treatment would continue in 2 months with the use of a nasal shaper joined to this plate. Appointments were scheduled every week to perform activations and changes according to the needs of the patient (Figures 4-7).
Case 2Diagnosis



Male patient, two months of age, who was admitted in the orthodontics service for assessment and treatment with pre-surgical orthopedics. Upon clinical examination a bilateral, complete cleft lip and palate was observed along with premaxillary protrusion, a short columnella, asymmetric and depressed nostrils (Figures 8 y 9).
Treatment goals

To retract and align the premaxilla and shape adequately the alveolar process in addition to form the depressed nasal wings and stimulate closure of the palatal processes as well as to obtain better surgical outcomes.
Treatment planThe patient's mother signed an informed consent where the diagnosis, treatment plan and possible complications were specified. Treatment plan consisted in obtaining an impression with condensation silicone to make a Friedman obturator that would align and retrude the premaxilla using as auxiliary extraorally attached tapes placed at 45° so that they would exert a force direction and intensity suitable for that purpose.
Once this goal was achieved, conformation of the nasal wings was continued (Figures 10 and 11).
RESULTS

Duration of treatment with pre-surgical orthopedics in the first case was eight weeks (Figures 12-14) and in the second case, 16 weeks (Figures 15 and 16). Adequate formation of the alveolar process, elongation and improved symmetry in the columnella, stimulus for cleft palate closure was achieved as well as a better tone of the perioral muscles thus favoring a good surgical tissue management and achieving lip closure without tension with good functional and aesthetic results.
DISCUSSION




The concept of early pre-surgical orthopedics for children who suffer from CLP was initially developed by Mc Niel3 and Burston4 in the 50's decade in England, although it was not consolidated as a technique until several years later. In 1984 Matsuo et al5–7 used cartilage molding techniques in the neonatal period to effectively correct congenital deformities of the cleft lip and nostrils. Later, in 1990 Nakajima et al,8 described a device fitted to the contour of the nasal wing to maintain what had been achieved with the surgical correction of the lip and nose. But in 1999 Yeow et al,9 added that it should be used for at least 6 months after the correction of the lip.
It was not until 1999 that Grayson10,11 described the nasoalveolar molding technique which was very well accepted since it offered a new alternative for patients in the neonatal period, prior to the execution of the first surgery of the lip and nose. In the literature, several successful results are reported since it shapes adequately the wing of the nose and provides a more aesthetic and functional way of shaping and changing the position of the immature and malleable nasal cartilage thus lengthening the columnella.12,13
Nasal molders are accessories that were created with a biological basis supported on the theory of Roux14 which supports that there is an intimate relationship between shape, structure and function. Afterwards, Dr. Moss in the 60's promoted his theory under the concepts of a periostic and capsular functional matrix.15 That is the reason why before cheiloplasty, nasal molders modify the depression of the wing of the nosecaused by the fissure therefore improving the projection of the tip of the nose and slightly lengthening the columnella if used in early stages. Nasal molders are also used in after the primary rhinoplasty helping to prevent relapse of the conformed nasal wing, maintaining an open airway and limiting surgical adhesion that result from nasal secretions and scarring.16
Early orthopedics must be handled in three dimensions; vertical, sagittal and transverse. The nasal molder must be inserted into the obturator which stimulates the palatal processes and approaches them by presence of acrylic along with muscular forces. As a result, the nose is shaped and the deformation of the nasal wall is reduced as it stimulates and repositions soft tissues and nasal cartilage.17
Once the patient has been selected for the use of this technique, a protocol for the PNAM (presurgical nasoalveolar moulding) fabrication is followed. A silicone impression is obtained and pre-surgical treatment is begun preferably in the first ten days after birth and the design and inserting the PNAM is performed for molding the alar cartilage with a maximum duration of six months.10,18
These devices have other advantages: they approach the palatal processes improving archshape, the tongue is better positioned, there is a balance of the intraoral pressure and also facilitates the modification of the nasal tissues to improve the results in the first surgical procedure. Also, when used after the secondary rhinoplasty, they maintain the shape and position achieved, diminish the nasal stenosis of the nostrils, prevent the collapse of the nose, favors airway permeability and reduces surgical adhesions due to nasal secretions. But in order to achieve all this the parents cooperation is required as well as a correct manufacture and fitting of the appliance.18
CONCLUSIONSPresurgical orthopedics is an effective treatment in patients with CLP and when performed early favorable results may be achieved thus improving the quality of life of these patients.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia.