



The purpose of this study was to verify if the angle formed by the SN plane with the Frankfort plane (Bimler factor 7) tends to open in long-faced facial patterns (dolichofacial) and to close in short-faced facial patterns (brachifacial).
Material and methodsThis was a comparative, retrospective, cross-sectional study. The study universe was initial digital lateral headfilms of patients who attended the clinic of the Department of Orthodontics at the Division of Postgraduate Studies and Research of the UNAM. The lateral headfilms were taken randomly from the period between August 2010 and August 2012. The sample consisted of 100 radiographs of patients between 18 and 30 years of age, 50 brachifacial and 50 dolichofacial; previously classified using Bimler facial index and confirmed with Ricketts facial taper.
ResultsFrom the 100 measured radiographs, 58 belonged to female patients and 42 to male patients. The average age was 27 years, with an age range from 18 to 30 years. In the 50 radiographs of dolichofacial patients, there was a range of 7 to 14° and in brachifacial patients, a range of 3 to 8° of the SN-FK angle or Bimler factor 7. In the 50 X-rays of dolichofacial patients an average of 11° was found and in the 50 X-rays of brachifacial patients an average of 5° was found.
ConclusionsOn the basis of the results hereby obtained it may be observed that the angle formed by SN-Frankfort planes increases in patients with a vertical growth pattern (dolichofacial) and decreases in patients with a horizontal growth pattern (brachifacial).
El propósito de este estudio es comprobar si el ángulo formado por SN con el plano de Frankfort (factor 7 de Bimler) tiende a abrirse en patrones faciales con cara larga (dolicofaciales) y a cerrarse en pacientes con patrones faciales de cara corta (braquifaciales).
Material y métodosEl presente es un estudio comparativo, retrospectivo, transversal. El universo de estudio, radiografías digitales laterales de cráneo iniciales de pacientes que asisten al Departamento de Ortodoncia de la División de Estudios de Postgrado e Investigación de la UNAM, las cuales fueron tomadas al azar en el periodo correspondiente de agosto del 2010 a agosto del 2012. La muestra de 100 radiografías laterales de pacientes entre 18 y 30 años de edad, 50 braquifaciales y 50 dolicofaciales; previamente clasificados con el índice facial de Bimler y confirmados con el cono facial de Ricketts.
ResultadosDe las 100 radiografías medidas, 58 pertenecieron a pacientes femeninos y 42 a pacientes masculinos. La edad promedio de los pacientes fue de 27 años, con un rango de edad de los 18 a los 30 años. De las 50 radiografías laterales de los pacientes dolicofaciales, existió un rango de 7 a 14° y en pacientes braquifaciales un rango de 3 a 8° del ángulo SN-FK o factor 7 de Bimler. De las 50 radiografías de los pacientes dolicofaciales se encontró un promedio de 11° y de las 50 radiografías de los pacientes braquifaciales se encontró un promedio de 5°.
ConclusionesCon base a los resultados obtenidos podemos comprobar cómo el ángulo formado por SN-Frankfort es aumentado en pacientes con patrón de crecimiento vertical (dolicofaciales) y como es disminuido en pacientes con patrón de crecimiento horizontal (braquifaciales).
The anterior base skull involves cephalometric structures that go from Nasion point (most anterior point of the fronto-nasal suture) to Sella point (center of the sella turcica).1
Inclination of the anterior base skull may be modified by factors such as morphogenetic anomalies that affect the skull, trauma suffered by the mother during pregnancy, severe illnesses during pregnancy, in utero position with localized pressure, trauma during birth and certain syndromes such as Turner syndrome (45 X0 chromosome constitution), Klinefelter syndrome (47 XXY chromosome constitution).2
In opinion of some authors such as Mollet, Gravely and Freeman, angular measurements that are performed taking as reference the S-N line are not fully reliable since Nasion point is located in the outer limit of the frontonasal suture and not in its own base; due to its location, this point suffers remodeling changes during growth. According to these authors, the inclination of the anterior base skull may give us a false idea of the value alteration related to it.3,4
However, there are many authors and analysis who have advocated for the use of the S-N plane as a reference plane for their measurements. Thus we find among others the analysis of Steiner, Schwartz, Downs, Björk, Bimler, Bergen, Lavergne, and Moshiri.5
In Bimler's cephalometric analysis the patient is not compared only with statistical standards but he or she is studied in accordance with the relations of his or her individual, morphological and functional components.6,7
For this purpose the whole complex of dentofacial relations is then divided into different regions and factors that are studied separately and with different meanings.
Determination of each individual's characteristics is given to us by the so-called «analysis of factors»:
Factor 1 and 2 form the profile angle.
Factor 3, 4 and 5 are the elements of the basal angles (mandibular level).
Factor 4 defines maxillary inclination.
Factor 5 defines clivus inclination.
Factor 6 is the stress-axis of the teeth.
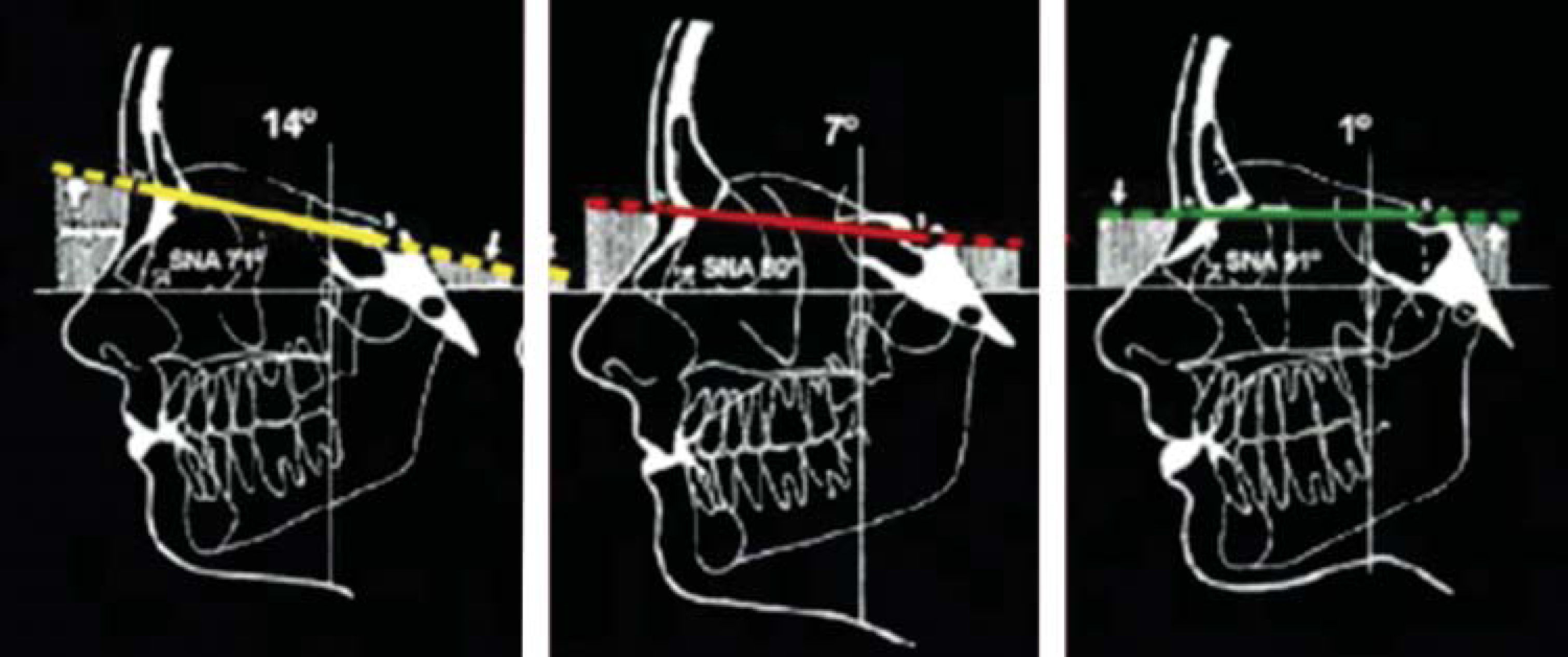
Factor 7 the inclination of the NS line, the anterior base skull with relation to the Frankfort plane.
Factor 8 ramus inclination.
Factor 9 the sphenoidal angle.
Factor 10 determines nasal protrusion.
The utility of the NS line is limited to obtain measures only in the same individual. Factor 7 has an average value of 7 degrees. Higher values belong to a vertical type, while lower values determinea horizontal type (Figure 1).

The average length of the skull base in males is 70.02mm, and in women, 67.84mm. The average angle between the anterior skull base (S-N) and the Frankfort plane (Po-OR) is 7.23° in men and 6.96° in women.
For all the above, it is important to check if there is a relationship between the facial biotype of the patient and an increase or decrease in the angle formed by the SN plane with the Frankfort plane (factor 7 Bimler).
JUSTIFICATIONIn view of the high prevalence of variations of skull base inclination and its direct impact on the diagnosis of malocclusions, we decided to take a sample of initial lateral headfilms of patients at the Department of Orthodontics of the Division of Postgraduate Studies and Research of the UNAM and determine if there was a relationship between facial biotype and the increase or decrease of the angle formed by the plane SN with the Frankfort plane or factor 7 Bimler, as mentioned by the author in his cephalometric analysis.
MATERIAL AND METHODSThis is a comparative study, retrospective, crosssectional study.
Study populationThe study universe was initial digital lateral headfilms of patients who attended the Department of Orthodontics at the Division of Graduate Studies and Research of the UNAM. The lateral headfilms were obtained randomly in the period from August 2010 to August 2012. The sample consisted of 100 lateral headfilms of patients between 18 and 30 years of age, 50 brachifacial and 50 dolichofacial that had been previously classified with Bimler facial index and confirmed by Ricketts facial taper which uses the facial and mandibular planes. When the angle formed by these planes is 68°, with a tolerance of 3°, the patient is mesofacial. If the values are higher than 71°, the patient would be classified as brachifacial, and if the angle is lower than 65°, the patient would be considered dolichofacial.
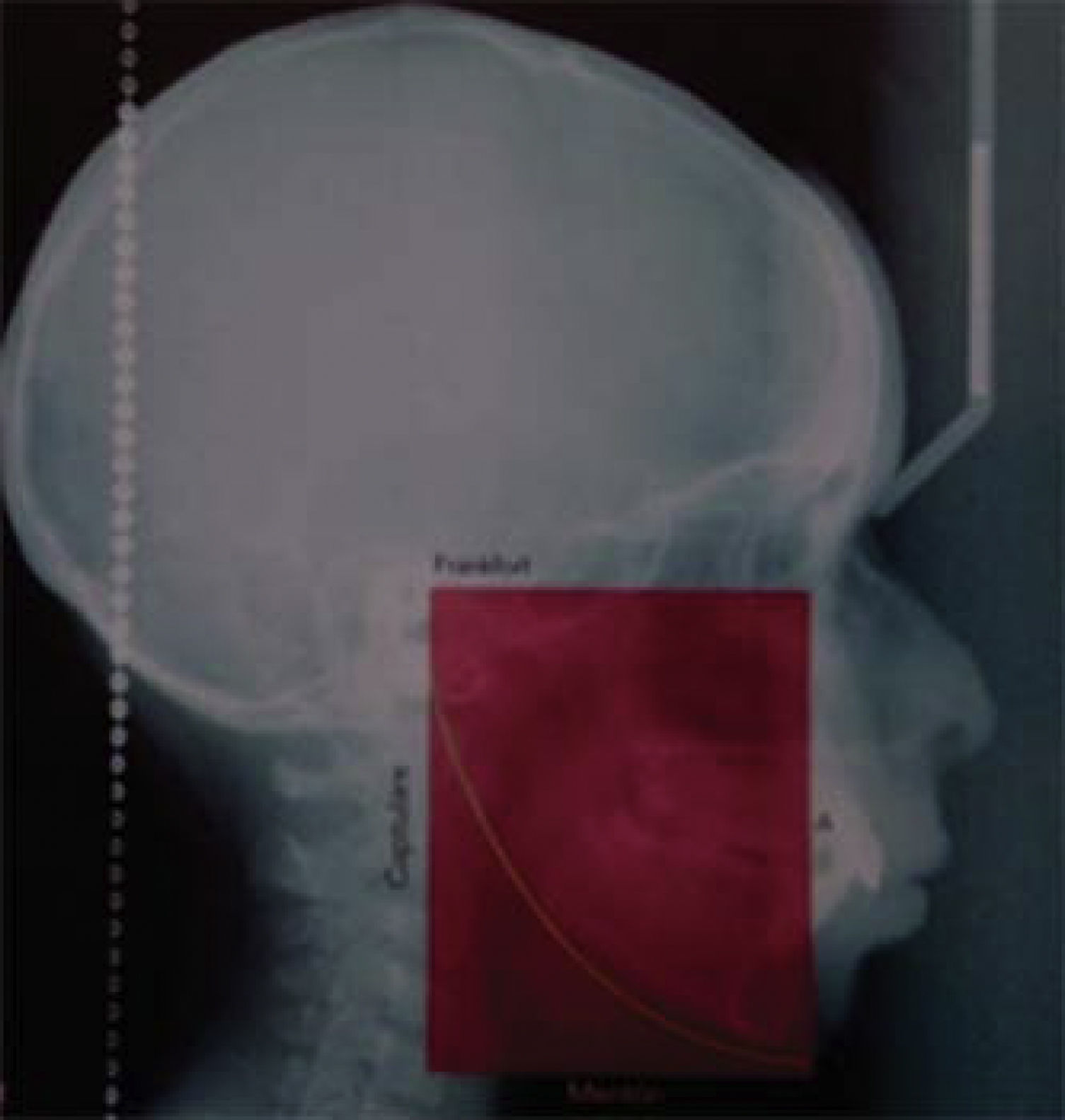
In Bimler facial index a box is formed using two sagittal and two horizontal planes. The sagittal planes are formed by drawing a perpendicular to Frankfort plane, the first, beginning at point A and the other at point C (Capitulare). The horizontal planes are Frankfort plane and a parallel to the same beginning at the lower rim of the chin symphysis.
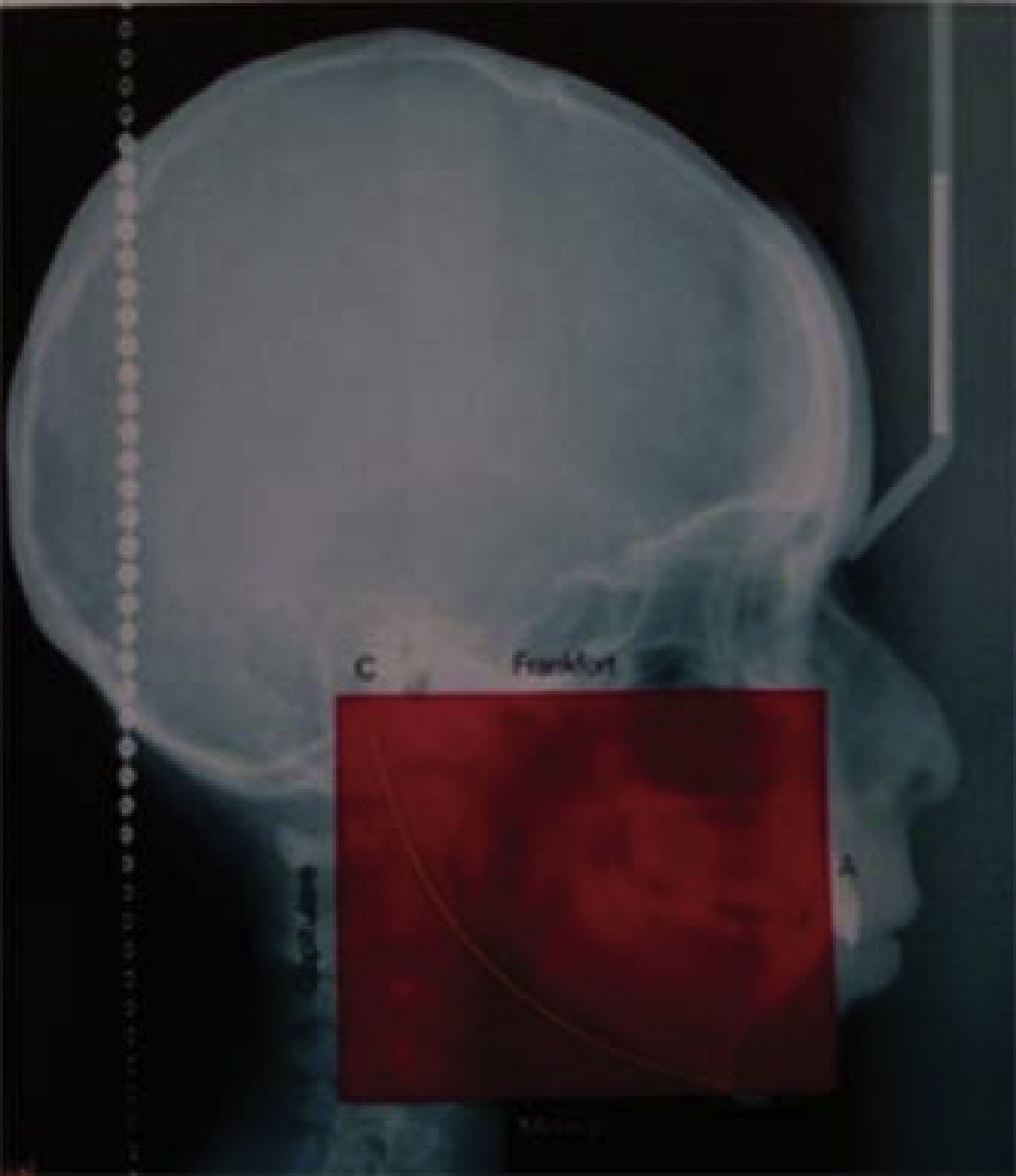
If the anterior height of this box is greater than the upper depth by more than one centimeter, the patient will be classified as dolichofacial (Figure 2), if it is shorter, the patient will be brachifacial (Figure 3).


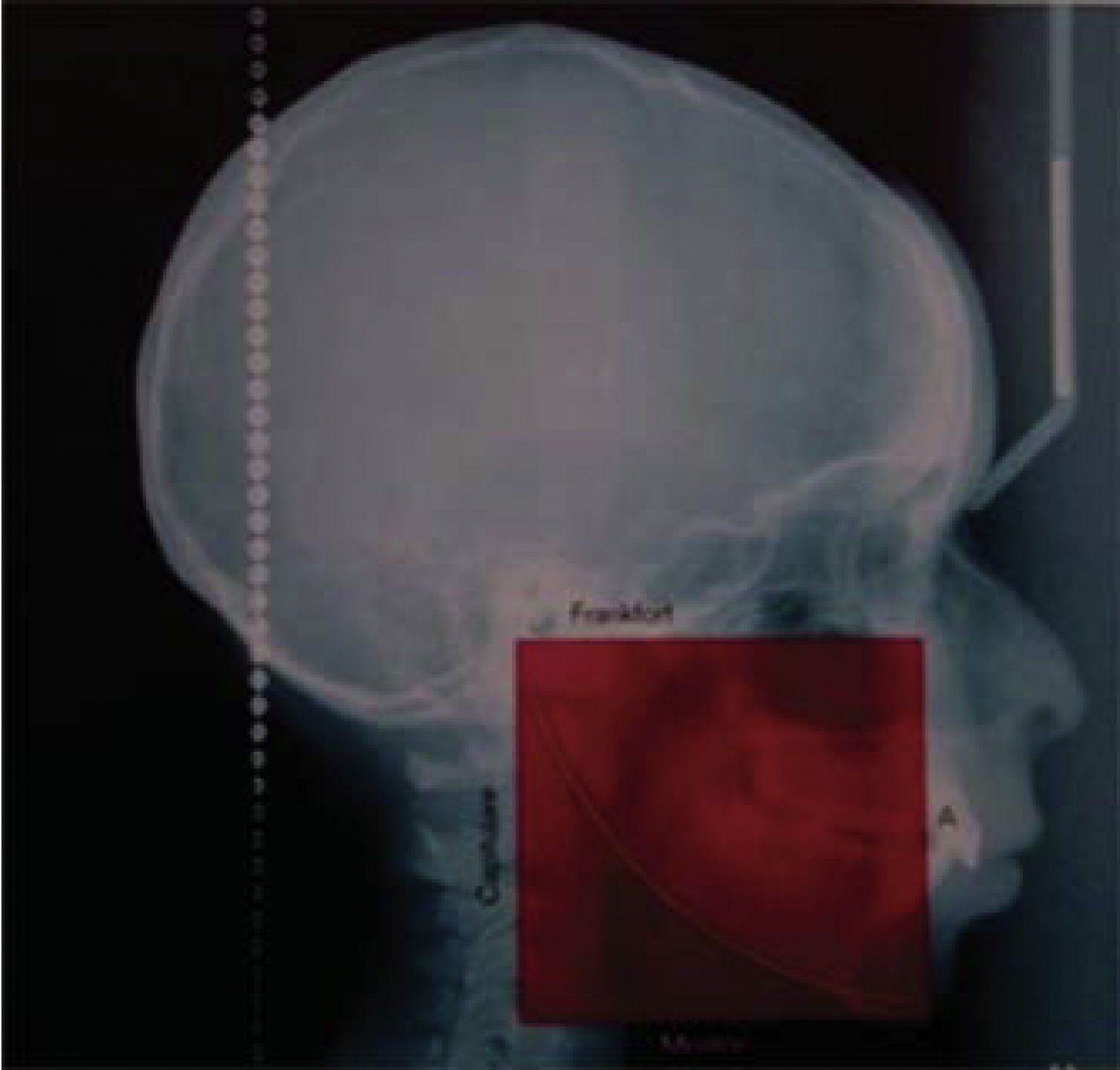
In the event that both measurements are equal or do not exceed more than a centimeter between them, the patient will be considered mesofacial (Figura 4).
Cephalometric points
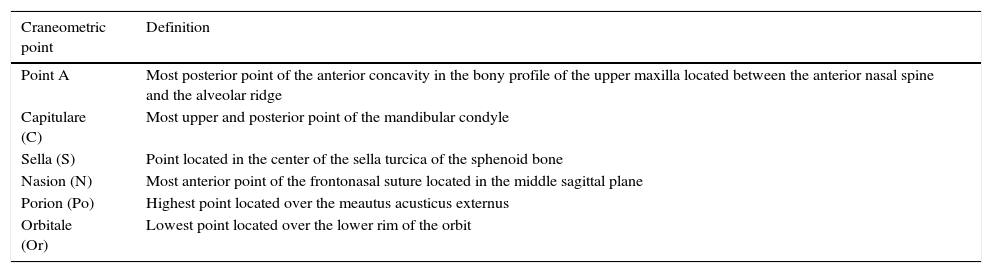
The cephalometric points used in this study were: point «A», Capitulare (C) Sella (S), Nasion point (N), Porion (Po) and Orbitales (Or) (Table I).
Craneometric points used in this study.
| Craneometric point | Definition |
|---|---|
| Point A | Most posterior point of the anterior concavity in the bony profile of the upper maxilla located between the anterior nasal spine and the alveolar ridge |
| Capitulare (C) | Most upper and posterior point of the mandibular condyle |
| Sella (S) | Point located in the center of the sella turcica of the sphenoid bone |
| Nasion (N) | Most anterior point of the frontonasal suture located in the middle sagittal plane |
| Porion (Po) | Highest point located over the meautus acusticus externus |
| Orbitale (Or) | Lowest point located over the lower rim of the orbit |
The measurements were made by a single operator who measured each radiograph twice after prior calibration.
The digital radiographs were taken with the Orthophos XG Plus machine with 75 kilovolt, 15mA. The exposure was 0.04sec.
After classifying the 50 radiographs in brachyfacial and dolichofacial patients and continued to measure the angle formed between the anterior skull base (S-N) and the Frankfort plane (Po-Or), also called factor 7 Bimler or compensatory factor.
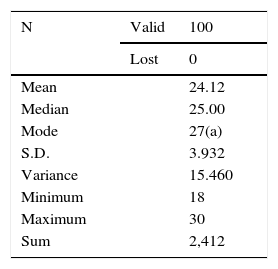
RESULTSOf the 100 radiographs that were measured, 58 belonged to female patients and 42 to male patients.
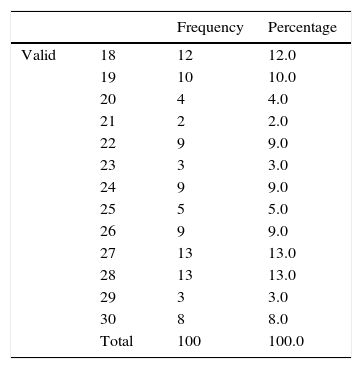
The average age of the patients was 27 years (Table II), with an age range from 18 to 30 years (Table III).
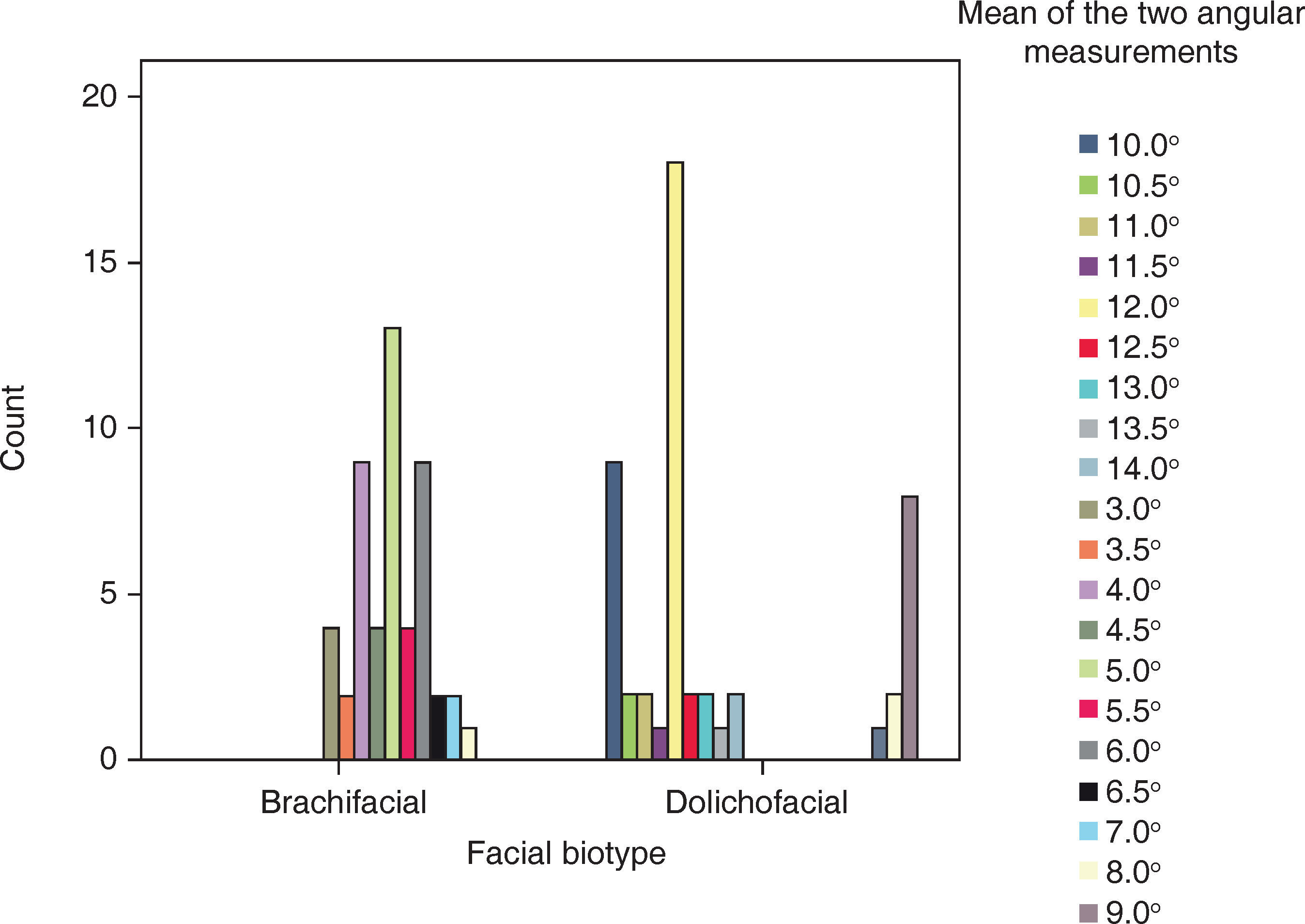
In the 50 radiographs of dolichofacial patients, there was a range of 7 to 14° and in the 50 radiographs of brachifacial patients a range of 3 to 8° was observed for the SN-FK angle or Bimler factor 7 (Table IV). For a wider representation of the results, figure 5 may be observed.
Contingency table according to the facial biotype and the average of the angle measurement.
| Count | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean of the two angle measurements | |||||||||||||||||||||
| Facial biotype | 10.0° | 10.5° | 11.0° | 11.5° | 12.0° | 12.5° | 13.0° | 13.5° | 14.0° | 3.0° | 3.5° | 4.0° | 4.5° | 5.0° | 5.5° | 6.0° | 6.5° | 7.0° | 8.0° | 9.0° | Total |
| Brachifacial | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 2 | 9 | 4 | 13 | 4 | 9 | 2 | 2 | 1 | 0 | 50 |
| Dolichofacial | 9 | 2 | 2 | 1 | 18 | 2 | 2 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 8 | 50 |
| Total | 9 | 2 | 2 | 1 | 18 | 2 | 2 | 1 | 2 | 4 | 2 | 9 | 4 | 13 | 4 | 9 | 2 | 3 | 3 | 8 | 100 |

In the dolichofacial patients an average of 11° was found and in brachifacial patients an average of 5° was obtained.
The data was analyzed with the SPSS 22 statistical package.
DISCUSSIONIn a study conducted by Quiroz in Venezuela in 1999 with a sample of 233 patients, it was found that the SN-FK angle is variable, in males it was 7.23° and in women, 6.96°. Riolo in another study found that in males it was 4.85° and in women, 5.43°.4
Thus the results are contradictory since Quiroz tells us that the SN-Frankfort or Bimler factor 7angle is higher in males and lower in women and according to Riolo it is the other way round. Seeing that there is no verifiable relationship in terms of sex and SN-Frankfort inclination, this study attempted to link the increase or decrease of Bimler factor 7 on the basis of facial biotype. The obtained results were equal to those of Bimler cephalometric analysis, according to factor 7: higher than 7° values belong to a vertical biotype, while lower values determined a horizontal type.
CONCLUSIONSBased on the obtained results it may be observed that the angle formed by SN-FK increases in patients with a vertical growth pattern (dolichofacial) and decreases in patients with a horizontal growth pattern (brachifacial).
Taking into consideration the facial biotype of the patient, we may know if the values of Bimler factor 7 will result to be increased or decreased and thus do not stigmatize the SN plane as «unreliable» or «unstable» but rather understand that this plane adopts such tilt in relation to Frankfort depending on the patient's biotype.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia