




The objective of this study was to determine if the influence of an occlusal imbalance caused in the molars of rats originates scoliosis of the spine.
Material and methodsThe study sample consisted of 36 Wistar rats, 4-months- old that were divided into three equal groups. A spine X-ray was obtained from all rats prior to the experiment. In the first experimental group a 0.5mm occlusal stop was placed at the upper right first molar for two weeks. After this period was completed, a spinex-ray was taken. Subsequently another occlusal stop was placed on the opposite sidein order to level the stopsduring two weeks and afterwards, the columnwas radiographically assessed once again. The second experimental group received an occlusal stop in the upper right first molar for 4 weeks and x-rays were obtained. In the control group no occlusal stop was placed.
ResultsAccording to the initial Cobb angle of the first experimental group (n= 12), the average was 1.42° ± 1.31° in the spinex-rays; after the occlusal stop was placed on the upper right molar for two weeks the group showed a column deviation of 15.17° ± 6.7°; subsequently a second occlusal stop was placed on the opposite side to balance the occlusion and after another two weeks the column almost returned to its original position (3.17° ± 2.48°). The second experimental group (n = 12) prior to the start of the experiment showed an average Cobb angle of 1.17° ± 1.19°; after two weeks with the unilateral occlusal stop it increased to 13.67° ± 10.61° and after four weeks it was 22.33° ± 12.19°. In the control group (n = 12) without any stop, the column remained stable.
ConclusionsThe present study demonstrated that through an occlusal imbalance the spine may be altered, causing scoliosis and as soon asthe alterationis eliminated, column alignment is evident.
El objetivo de este estudio fue determinar si la influencia de un desequilibrio oclusal ocasionado en los molares de ratas, origina escoliosis de la columna vertebral.
Material y métodosLa muestra del estudio consistió en 36 ratas Wistar de cuatro meses de edad, las cuales fueron divididas en tres grupos iguales. A todas las ratas se les tomó una radiografía de columna antes de comenzar el experimento. Al primer grupo experimental se le colocó un tope oclusal de 0.5mm a la altura del primer molar superior derecho durante dos semanas. Concluido este lapso se les tomó una radiografía de columna. Posteriormente, se les colocó otro tope oclusal del lado contrario por dos semanas para nivelar los topes, después de lo cual se volvió a evaluar radiográficamente la columna. Al segundo grupo experimental se le colocó un tope oclusal en el molar superior derecho por cuatro semanas y se tomaron radiografías. Al grupo control no se le colocó ningún tope oclusal.
ResultadosDe acuerdo al ángulo de Cobb inicial del primer grupo experimental (n = 12), el promedio fue de 1.42° ± 1.31° en las radiografías de la columna; se les colocó un tope en el molar superior derecho por dos semanas, con lo que el grupo mostró una desviación de la columna a 15.17° ± 6.7°; posteriormente se colocó un segundo tope oclusal del lado contrario para balancear la oclusión y transcurridas otras dos semanas la columna casi regresó a su posición original (3.17° ± 2.48°). El segundo grupo experimental (n = 12) antes de comenzar el experimento presentó un promedio del ángulo de Cobb de 1.17° ± 1.19°; a las dos semanas con el tope oclusal unilateral incrementó a 13.67° ± 10.61°) y a las cuatro semanas hasta 22.33° ± 12.19°. En el grupo control (n = 12) sin tope alguno, la columna se mantuvo estable.
ConclusionesEl presente estudio demostró que el provocar un desequilibrio oclusal puede alterar la columna vertebral ocasionando escoliosis y en cuanto se elimina la alteración, la alineación de la columna es evidente.
The history of the disorders and injuries of the muscular-skeletal system goes back to antiquity, specifically to the year of 1741 when Nicholas Andry established the art of preventing and correcting skeletal deformities in children.1 A common muscular-skeletal disorder is back pain, which is very frequent and may be caused by multiple factors, among which are traumatisms, herniated disks, infections, tumors and scoliosis. Scoliosis is a deformity without a clear aetiology, it is therefore considered to be multifactorial. Some hypotheses have been formulated regarding thepatho-physiological mechanisms of such column deformity: malformations, failures in vertebral segmentation, muscle imbalance.2 From Dentistry's point of view, it has been suggested that due to an imbalance of the dental arches either by lack of teeth or by dental malpositions- there is a possibility of producing scoliosis.3 The diagnosis of this condition is unknown by most dentists.
On the other hand, it has been reported in the literature that 30 to 40 per cent of low back pains may be caused or aggravated by a dental malocclusion.4 It has also been suggested that the temporomandibular jointsmay be affected by overloads. Therefore it is necessary that the occlusion is balanced since if this equilibrium is lost due to multiple extractions or dental malpositions, it may result in an instability that may cause muscular atrophy which in turn causes the cranium to rotate and produces an overload in the vertebral spine5 which may give rise to back pain as an effect of muscle imbalance.6,7 The objective of this study was to determine if the influence of an occlusal imbalance caused in the molars of rats, originates scoliosis.
MATERIALS AND METHODSSample selectionThe study sample consisted of 36 Wistar rats, 4 months of age, which were divided into three groups (Bioteriorio UAM-X, Mexico City). Two experimental groups of twelve rats each were formed and the remaining third constituted the controlgroup which received no treatment.
Preparation for anesthesiaFor obtaining the X-ray (Kodak, USA) and placing the occlusal stop, the rats were anesthetized with 10% xylazine and ketamine hydrochloride equivalent to 1000mg ketamine; each rat was weighed for a correct dosage of the anesthetic which was mixed in a 50-unit insulin syringe in a proportion of 1 unit of ketamine hydrochloride and 1 unit of xylazine per 10g of weight. The injection was intraperitoneal for which the needle was inserted lateral to the median line, next to the vertex of the bladder and distal to the liver and stomach (procedure approved by the Ethical Committee of Animal rooms of the Intercontinental University).
Occlusal stop placementThe height of the occlusal stop was controlled by fabricating it over a flat surface outside the mouth in order to obtain a half-millimeter height. This was checked with a double metal tip compass. A silicon mold was made to provide the exact measurement and it was placed on the surface of the upper right molar with the purpose of causing an occlusal imbalance due to premature contact.
The experimentalgroup E2 [N = 12] remained with an occlusal stop in the upper right molar for a period of two weeks. Then a second spine X-ray was obtained and the changes produced by the premature contactwere assessed.
Subsequent to the spine X-rays a second stop was placed in the upper left molar to produce an occlusal balance in the 12 rats in the experimental group (E2). The stop had the same height characteristics as the first occlusal stop previously placed, while the third experimental group (E3) remained with a single unilateral occlusal stop. This continued for two weeks and once again, spine X-rays were obtained from all rats. The control group did not receive any occlusal stop.
Spine X-ray procedureSpine X-rays were performed to all three groups with a conventional X-ray machine before inducing any occlusal change (T0) and after the rats were under anesthesia. Each rat was placed on a Styrofoam bed, face up. While holding its head upwards to avoid torsion in the column, the upper and lower extremities were held in a parallel way to avoid measurement errors of the vertebral column. The two experimental groups received a 0.5 mm-heightresin (3M, Monrovia Ca, USA) occlusal stop in the upper right molar.
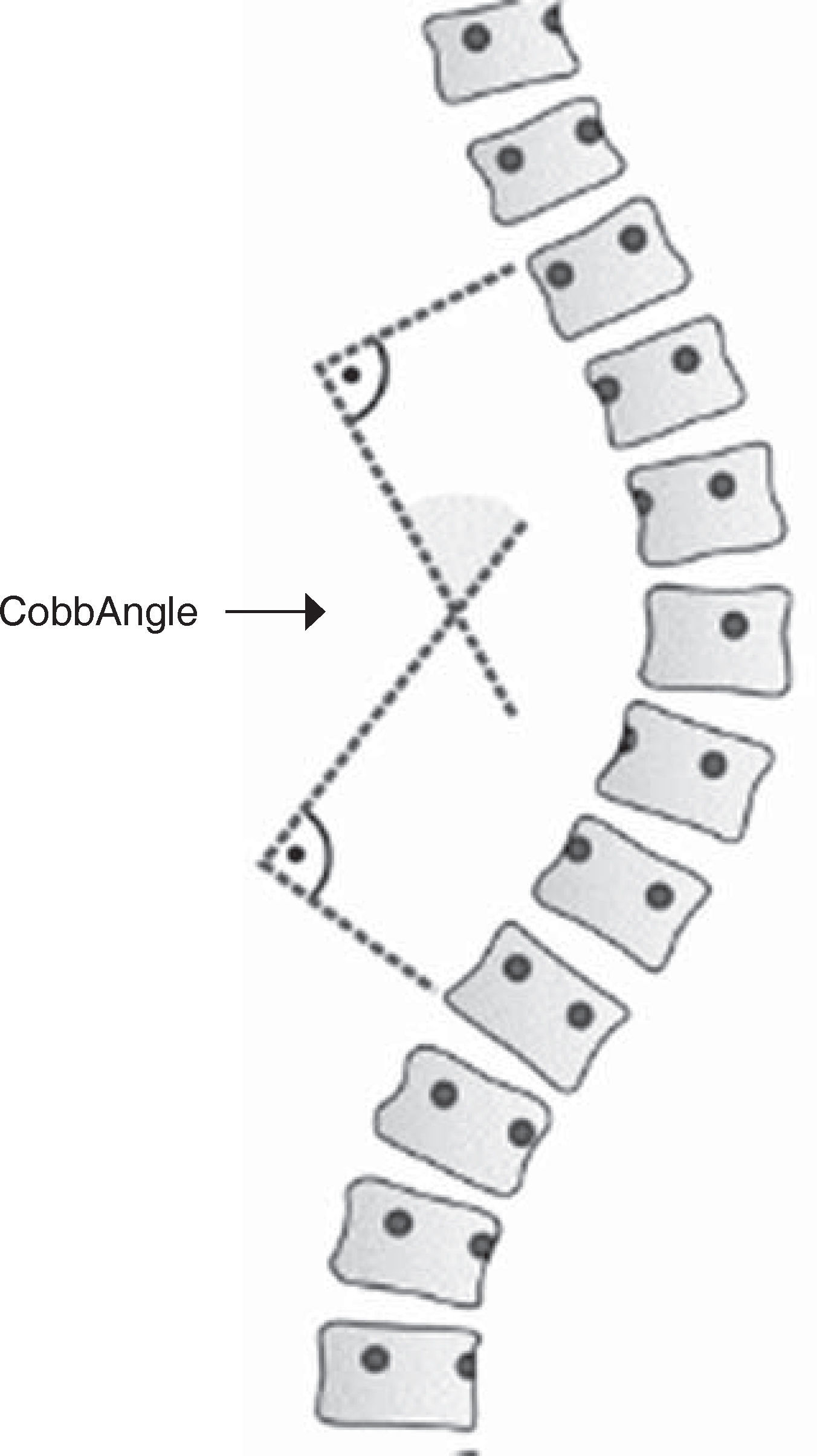
Scoliosis assessmentIn order to determine the presence of scoliosis in the studied rats the Cobb angle was used. To obtain this angle a first line was drawn through the upperrim of the upper vertebrae and the lowerrim of the lower vertebra of the scoliosis. Then another set of lines was drawn at an angle of 90° with respect to the previous lines. The intersection of these last two lines is called Cobb angle (Figure 1).8
Management and care of the animals
Without exception, the rats were observed carefully along all tests included in the study, from the start point until the end of the experiments and without varying the intake of food and water so that the rats were kept in good health.
Statistical analysisThe statistical test used in this study was the analysis of variance (ANOVA). Through the Fisher and Tukey test the existence of significant differences between the vertebral columns of the different groups of rats was determined.
RESULTSThe results of the study showed that from the moment in which the first series of X-rays were traced for measuring the Cobb angle, in those rats that did not receive any occlusal attachment -control group -the spine remained straight, without any change, after four weeks (Figure 2).

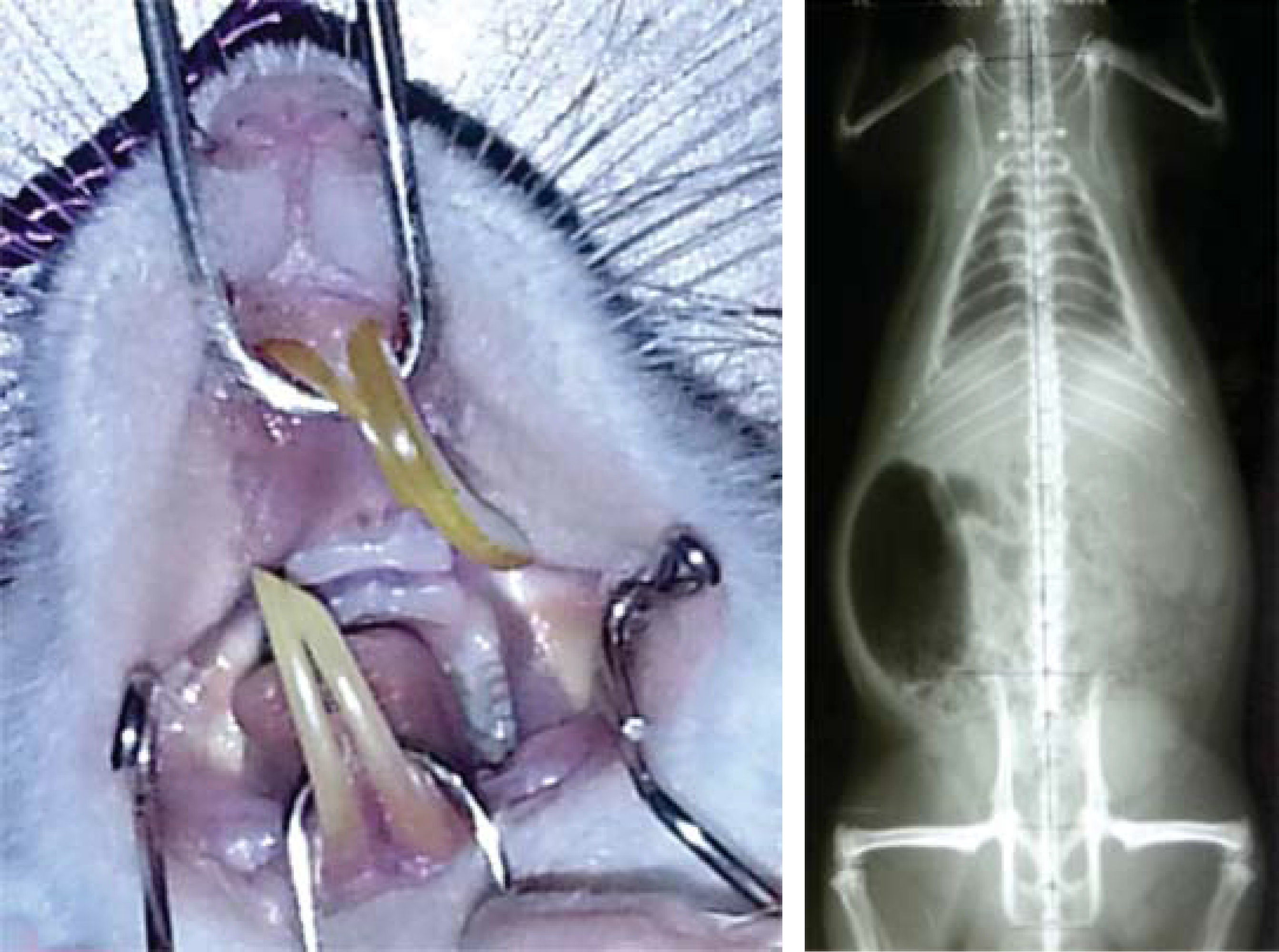
On experimental group (E2), - which received an occlusal stop on the upper right first molar- once two weeks had passed, a second set of spine X-rays was performed. Changes with no distinguishable pattern were observedin the vertebral columns of rats.
By measuring the Cobb angle it was demonstrated the change in degrees that the columnpresented where scoliosis may be observed in the X-rays (Figure 3).

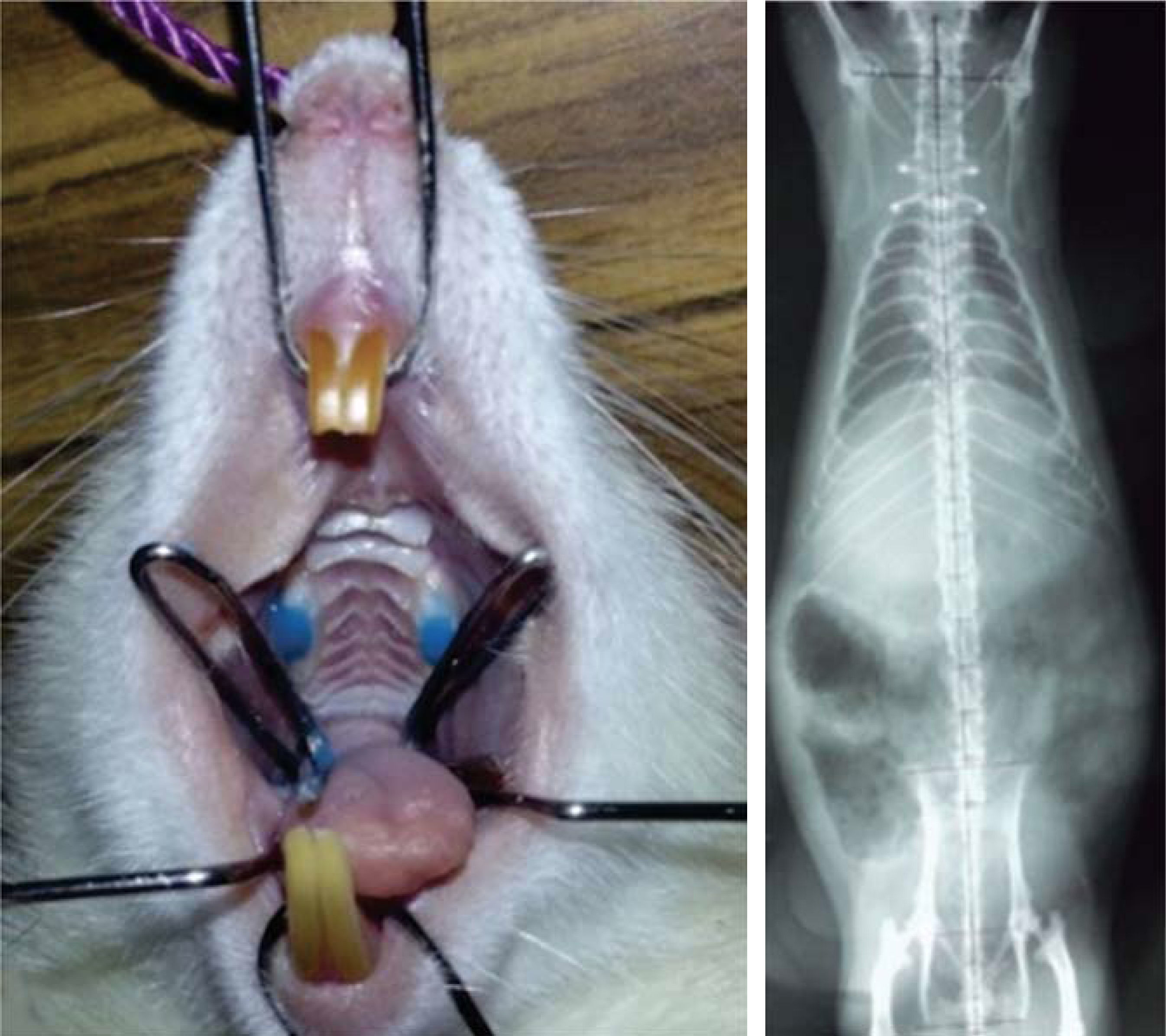
On experimental group (E2), after two weeks with a unilateral occlusal stop, a second occlusal stop was placed in the opposite upper molar and was left there for another two weeks. Afterwards, a third series of X-rays were performed and they showed that the vertebral column had re-aligned itself almost entirely (Figure 4).

However, in experimental group three (E3) that received only a unilateral occlusal stop it was observed that after four weeks the scoliosis was more severe (Figure 5).

During the four week period of the experiments, the control group (E1) - which did not receive any occlusal stops- remained stable with the spine in 2° (according to the Cobb angle).
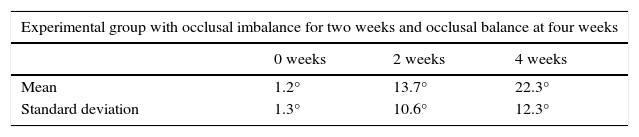
Experimental group (E3) began with an average of 1.17° in the spine, a single unilateral occlusal stop was placed and after two weeks of having caused the occlusal imbalance the angulation was 13.67°. After four weeks the spine was not able to adapt to this imbalance, by which the tilt of the spine rose to 22.33° (Table I).
Experimental group (E2) began with an average of 1.42° angulation of the column at the beginning of the study. After two weeks of having a single occlusal stop the average increased to 15.17° tilt in the spine; subsequently an occlusal stop was placed on the opposite molar for two weeks and the spine returned to 3.17°, perhaps because the occlusal imbalance was eliminated.
Due to the change presented by average of the experimental groups a standard deviation was found for both groups. The result of the standard deviation increased after two weeks in both groups, since until that moment a single occlusal stopremained on them. In the first group a standard deviation of 1.19° was obtained at the start of the study. After two weeks it rose to 10.61° and ended upincreasing to 12.19° after four weeks with a single occlusal stop.
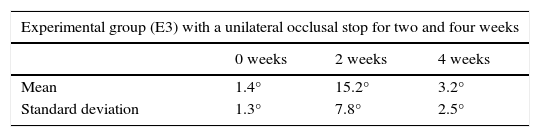
The second experimental group had a standard deviation of 1.31° at the start of the study and at the end of two weeks it increased to 7.83° but contrary to the first group, this figuredecreased after four weeks because an attempt was made to try to return the spine to its original form. The spine ended with an angulation of 2.48°.
Therefore, it may be observed that in the experimental group with a single occlusal stop at two and four weeks the dispersion was not as dramatic as in the group with two occlusal stops since there is greater variability between two and four weeks (Tables I and II).
Cobb angle average measured in degrees in the experimental group (E3) with a unilateral occlusal stop during four weeks.
| Experimental group with occlusal imbalance for two weeks and occlusal balance at four weeks | |||
|---|---|---|---|
| 0 weeks | 2 weeks | 4 weeks | |
| Mean | 1.2° | 13.7° | 22.3° |
| Standard deviation | 1.3° | 10.6° | 12.3° |
In this study an occlusal imbalance was produced by means of a resin stop on the occlusal surface of rat molars in order to determine if this originated an alteration at spine level. While assessing the spine of rats through the Cobb angle, after two weeks of having placed the occlusal stop, it was observed in the X-ray an alteration that caused scoliosis. It was decided then put a stop on the opposite molar to assess whether the balance of the imbalance would have an impact over the scoliosis which showed a significant decrease in the spine deviation. However, the unilateral occlusal stop for four weeks resulted in greater degree of scoliosis, so this study showed that by balancing the occlusion, the column alteration improved.
Considering the results of this study, we may suggest that occlusal problems may be related to the spine due to the imbalance that occurs in the masticatory musculature and its relationship with adjacent muscles. In dental practice it is very common to find a high incidence of pain in the muscles of the neck, back, lower and upper extremities, in addition to the temporomandibular joint.9 Some previous studies have demonstrated a relationship between occlusion and scoliosis10 in patients with plagiocephaly,11 in class III malocclusions with a Cobb angle of 30 to 50° tilt,12 in class II malocclusions13,14 and in unilateral crossbites.15
The occlusal alteration caused by the stop placed in rats showed that after two weeks evident changes were produced in the column.16–18 However upon stabilization of the occlusal imbalance the degree of scoliosis improved for what it has been suggested since many years ago that by stabilizing the occlusion in a timely manner, the head position is stabilized at the same time16–18 as the column alteration may reach the Sacro-iliac region.19 On the other hand, it has been suggested that for those patients who suffer from craniomandibular dysfunction an evaluation of the spinal column should be considered.20
The occlusal stop by producing instability in the occlusion and in the masticatory muscles causes an alteration in the spine. This is probably due to the fact that the musculature causes an inclination of the first cervical vertebra which will affect the inclination of the adjacent vertebras thus producing destabilization of the cervical spine with an alteration on the muscular function of the neck. This distributes an overload on one side which affects the orientation of the dorsal and lumbar vertebrae causing an alteration of the column and finally scoliosis.21 Scoliosis effects involvethe neural system between the trigeminal nerve and the nerves of the cervical spine.22
CONCLUSIONS- a)
The results of this study suggest that an occlusal imbalance may cause misalignment of the spine and scoliosis.
- b)
Upon eliminating the occlusal imbalance, an alignment of the column is evident again.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia
Graduate of the Orthodontics Specialty.
Former professor.