








Case report of a 19.6-year-old male patient who presented a skeletal class I with neutral growth, a class II division 1 dental malocclusion protrusion and proclination of upper and lower incisors, upper moderate and lower mild crowding. He also presented an overjet of 5mm and a 3mm overbite, the maxillary dental midline was deviated to the right. A squared maxillary arch and an oval mandibular arch. The objectives were to maintain the profile and skeletal class I, eliminate crowding and correct the teeth axial axis, to obtain bilateral canine class I and maintain a bilateral class II molar relationship, to obtain an adequate overbite and overjet, correct the midline and obtain a good balance and occlusal function. Treatment consisted in extraction of the maxillary first bicuspids and fixed orthodontic appliances according to the philosophy and technique of Roth. Retention was a removable upper retainer and a fixed one on the lower arch.
Reporte de un caso clínico de un paciente masculino de 19.6 años de edad, quien presentó una clase I esqueletal con crecimiento neutro, una maloclusión clase II división 1, protrusión y proinclinación de incisivos superiores e inferiores, apiñamiento moderado superior y leve inferior, sobremordida horizontal de 5mm y sobremordida vertical de 3mm, línea media maxilar desviada a la derecha. Una forma de arcada maxilar cuadrada y arcada mandibular oval. Los objetivos fueron: mantener el perfil y la clase I esquelética, eliminar apiñamiento y corregir el eje axial de los dientes, conseguir clase I canina bilateral, mantener la clase II molar bilateral, conseguir adecuada sobremordida vertical y horizontal, centrar línea media, obtener buen balance y función oclusal. El tratamiento consistió en extracciones de primeros premolares superiores y aparatología ortodóntica fija de acuerdo con la filosofía y técnica de Roth. La retención utilizada fue removible superior e inferior, así como retenedor fijo inferior.
Of all the patients who attend the Orthodontics Clinic at the Department of Orthodontics of the Division of Postgraduate Studies and Research at the UNAM, Angle class II malocclusions occupy almost 40% of the total number of patients.1
The treatments prescribed by the Roth's philosophy and technique, for class II malocclusions are performed in accordance to the elaboration of a diagnosis and treatment plan that may vary in relation to the age at which patients are attended. Currently the number of adult patients who require orthodontic treatment has increased gradually so that the correction for this kind of malocclusions focuses on correcting, compensating or camoufl aging the malocclusion that these patients present and who have already completed their growth stage.
To perform the correction of class II malocclusions in adult patients, extractions may include two maxillary premolars and two mandibular premolars.2 Extractions of only the upper premolars are indicated when there is no crowding or cephalometric discrepancy in the mandibular arch.3,4 These are probably the most extracted teeth for orthodontic purposes (according to the diagnosis of the orthodontic philosophy that applies for each treatment), because they have a convenient location between the anterior and posterior segments.
The variation in the sequence of extractions includes upper or lower, first or second premolars and are recommended by different authors for the great variety of techniques available today.5–10
In general, the skeletal features that are present in a class II malocclusion are not the primary determinant of how it should be treated by two or four bicuspid extractions, but rather making a complete diagnosis and evaluate the determinants for each case.4
CLINICAL CASEMale patient, 19.6 years of age, presents at the Orthodontics Clinic of the DEPeI, Faculty of Dentistry UNAM, with reason for consultation: «fix my the teeth because they were crooked».
Upon the initial extraoral clinical exam, he exhibited a symmetrical mesofacial pattern with straight profile and lip harmony (Figure 1).

The intraoral examination revealed that the patient presented a bilateral class II molar relationship and canine class II, moderate upper and lower anterior crowding, maxillary midline deviated to the right, overjet of 5mm, overbite of 3mm, the arch had a square shape in the maxilla and the oval-shaped arch in the mandible. The periodontal tissues were found healthy (Figure 2).

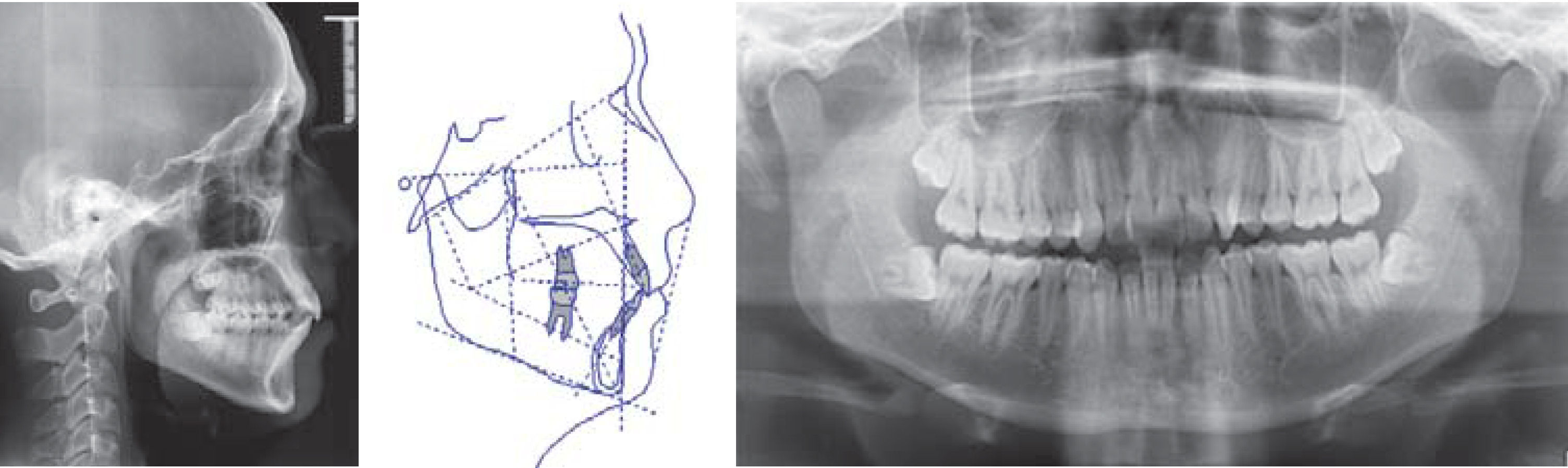
According to the analysis of the cephalometric studies, the maxillary proportions were appropriate and he presented a skeletal class I, neutral growth as well as dentoalveolar proclination and protrusion.
The panoramic X-ray reveals the presence of included upper and lower third molars, as well as acrown-rootratio of 1:2, 28 erupted and functional teeth. No apparent pathologies were observed (Figure 3).

In the model analysis a result of dental discrepancy was obtained in relation to the available space of -7mm in the upper arch and -3mm in the mandibular arch (Figure 4).
Treatment goals
The objectives were to maintain the profile and the skeletal class I since there was facial harmony. The goal was to eliminate overcrowding and in addition achieve correction of the axial axis of the teeth to obtain stability, as well as achieving the bilateral canine class I and maintaining the existing bilateral molar class II. Within the objectives it was also planned the correction of the overbite and overjet, as well as the midline to get a balance and an improvement in the occlusal function.
Treatment alternativesWe analyzed various procedures to carry out treatment, by selecting the one that served in a better way the proposed objectives.
As a first treatment option, it was proposed the extraction of the first maxillary and mandibular premolars and as a second alternative, the removal of the second maxillary premolars. The last proposal and the one that suited more our goals of treatment was upper first premolar extractions aided by interproximal stripping of the lower incisors to achieve the correction of the axial inclination of the anterior teeth, as well as solving the dental crowding.
Treatment sequenceAccording to the technique, .022 x .028” slot Roth prescription orthodontic appliances, were placed. As anchorage it was indicated to use a transpalatal arc, followed by the extractions. Following the technique indications, phase I was carried out by leveling with round nickel titanium archwires. Subsequently DKHL archwires were placed for phase II, space closure. During phase III rectangular archwires were placed for final torque and tipping, which were obtained through the prescription. Settlement was achieved using short elastics.
For retention a lower fixed retainer was placed from canine to canine, in addition to an upper and lower circumferential retainer (Figure 5).
RESULTS
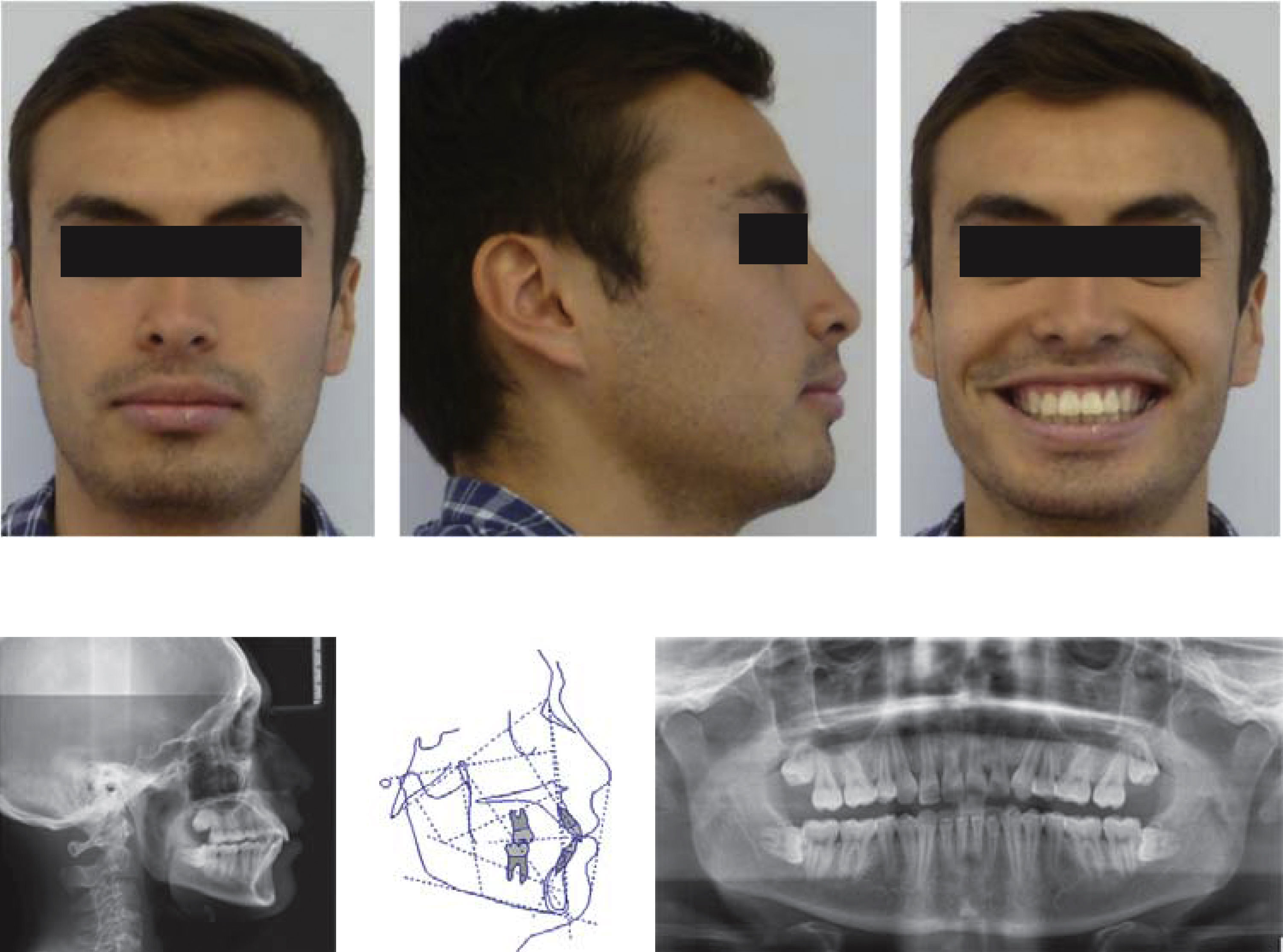
As observed in the extraoral photographs, it was possible to maintain the profile and skeletal class I, and in this way fulfill the objectives of the treatment plan (Figure 6).

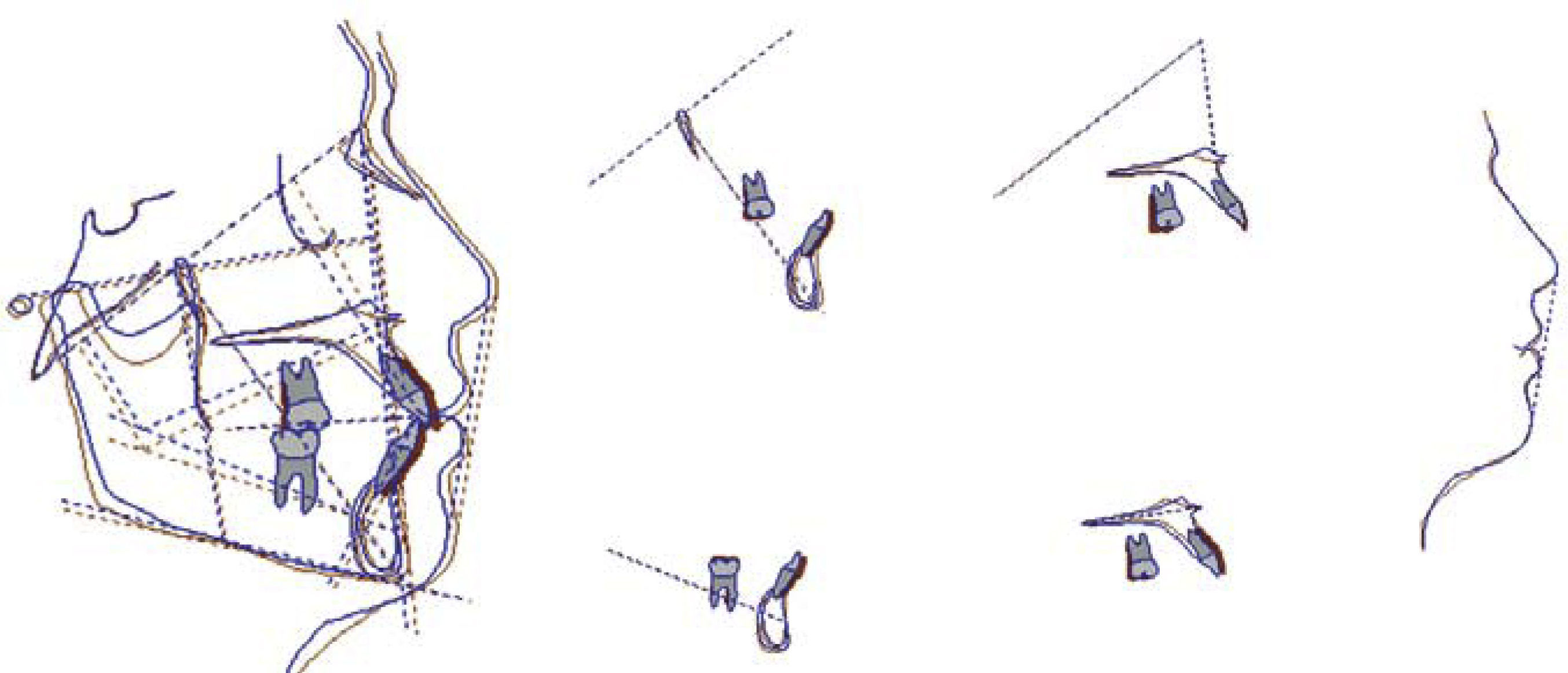
Likewise, the correction of the axial axis of the teeth was made as it can be observed in figure 7.

In the final intraoral photographs it is possible to assess that midline correction was obtained as well as bilateral canine class I, bilateral molar class II. The crowding was corrected, in addition to the overbite and overjet.
The patient referred being satisfied with theobtained results (Figures 8 and 9).


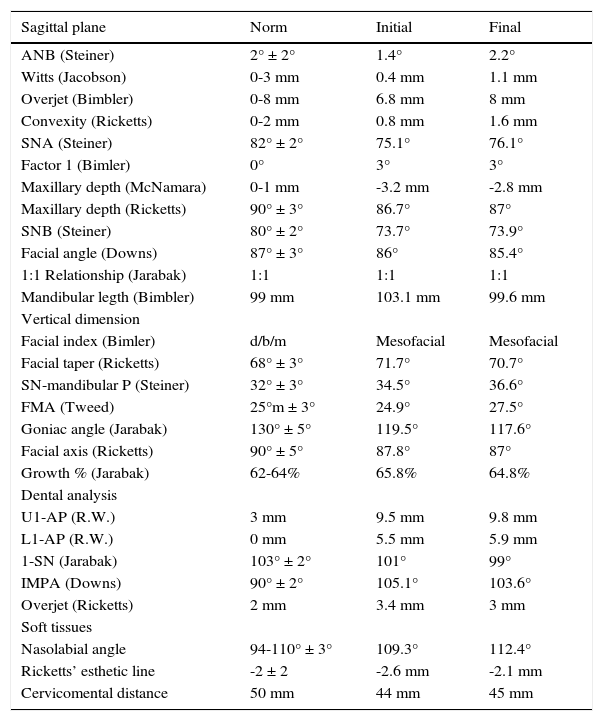
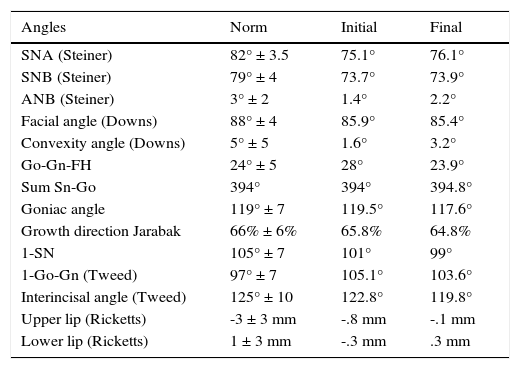
In the summary of cephalometric measurements the resulting changes from orthodontic treatment are shown. Correction was achieved of the inclinations of the upper and lower incisors giving as a result the future stability of the case. In the analysis of soft tissues, an increase in the nasolabial angle was observed (Tables I and II).
Initial integrated analysis cephalometry.
| Sagittal plane | Norm | Initial | Final |
|---|---|---|---|
| ANB (Steiner) | 2° ± 2° | 1.4° | 2.2° |
| Witts (Jacobson) | 0-3 mm | 0.4 mm | 1.1 mm |
| Overjet (Bimbler) | 0-8 mm | 6.8 mm | 8 mm |
| Convexity (Ricketts) | 0-2 mm | 0.8 mm | 1.6 mm |
| SNA (Steiner) | 82° ± 2° | 75.1° | 76.1° |
| Factor 1 (Bimler) | 0° | 3° | 3° |
| Maxillary depth (McNamara) | 0-1 mm | -3.2 mm | -2.8 mm |
| Maxillary depth (Ricketts) | 90° ± 3° | 86.7° | 87° |
| SNB (Steiner) | 80° ± 2° | 73.7° | 73.9° |
| Facial angle (Downs) | 87° ± 3° | 86° | 85.4° |
| 1:1 Relationship (Jarabak) | 1:1 | 1:1 | 1:1 |
| Mandibular legth (Bimbler) | 99 mm | 103.1 mm | 99.6 mm |
| Vertical dimension | |||
| Facial index (Bimler) | d/b/m | Mesofacial | Mesofacial |
| Facial taper (Ricketts) | 68° ± 3° | 71.7° | 70.7° |
| SN-mandibular P (Steiner) | 32° ± 3° | 34.5° | 36.6° |
| FMA (Tweed) | 25°m ± 3° | 24.9° | 27.5° |
| Goniac angle (Jarabak) | 130° ± 5° | 119.5° | 117.6° |
| Facial axis (Ricketts) | 90° ± 5° | 87.8° | 87° |
| Growth % (Jarabak) | 62-64% | 65.8% | 64.8% |
| Dental analysis | |||
| U1-AP (R.W.) | 3 mm | 9.5 mm | 9.8 mm |
| L1-AP (R.W.) | 0 mm | 5.5 mm | 5.9 mm |
| 1-SN (Jarabak) | 103° ± 2° | 101° | 99° |
| IMPA (Downs) | 90° ± 2° | 105.1° | 103.6° |
| Overjet (Ricketts) | 2 mm | 3.4 mm | 3 mm |
| Soft tissues | |||
| Nasolabial angle | 94-110° ± 3° | 109.3° | 112.4° |
| Ricketts’ esthetic line | -2 ± 2 | -2.6 mm | -2.1 mm |
| Cervicomental distance | 50 mm | 44 mm | 45 mm |
UNAM cephalometric analysis.
| Angles | Norm | Initial | Final |
|---|---|---|---|
| SNA (Steiner) | 82° ± 3.5 | 75.1° | 76.1° |
| SNB (Steiner) | 79° ± 4 | 73.7° | 73.9° |
| ANB (Steiner) | 3° ± 2 | 1.4° | 2.2° |
| Facial angle (Downs) | 88° ± 4 | 85.9° | 85.4° |
| Convexity angle (Downs) | 5° ± 5 | 1.6° | 3.2° |
| Go-Gn-FH | 24° ± 5 | 28° | 23.9° |
| Sum Sn-Go | 394° | 394° | 394.8° |
| Goniac angle | 119° ± 7 | 119.5° | 117.6° |
| Growth direction Jarabak | 66% ± 6% | 65.8% | 64.8% |
| 1-SN | 105° ± 7 | 101° | 99° |
| 1-Go-Gn (Tweed) | 97° ± 7 | 105.1° | 103.6° |
| Interincisal angle (Tweed) | 125° ± 10 | 122.8° | 119.8° |
| Upper lip (Ricketts) | -3 ± 3 mm | -.8 mm | -.1 mm |
| Lower lip (Ricketts) | 1 ± 3 mm | -.3 mm | .3 mm |
Malocclusions can be treated in several ways according to the characteristics associated with the problem, such as the anteroposterior discrepancy, age and complications of each patient.11
In this case, the patient was treated in accordance with Roth's philosophy and technique, with extractions only of first premolars, because no significant discrepancies existed, or severe crowding of the mandibular archwhich coincides with what was proposed by Strang in1957 and Bishara in1995.3,4
It was necessary to place double transpalatal bars to support the retraction of the anterior segment, however, despite we obtained acceptable results, loss of posterior anchorage was present and it limited the full retraction of the anterior segment and the consequent mesialization of the first upper molars even while maintaining throughout phase I and II of treatment the double transpalatal bars; this was due to the normal sliding mechanics of the anterior and posterior segments as reported by Sichuan in 2011. There is a movement relationship of the anterior maxillary teeth with the posteriors of 1:1.3, i.e. more mesialization occurs than retraction.12
The latter would have justified the use of labial miniimplants in order to achieve all necessary retraction and avoid mesialization of the posterior segment, given that there are studies that support the advantages of the use of these devices as maximum anchorage.13
One of the main facial considerations in this patient when we decided to perform extractions of the upper premolars was to maintain the profile and the position of the upper lip. At the end of the treatment changes were minimal in the position of the upper lip after removal of the upper premolars and the retraction of the upper incisors.
Another factor that helped maintain the profile was the position of the upper incisors, which had minimal changes in their labio-palatal inclination. These results are consistent with those reported by the studies of Bokas and Scott in 2006.14,15
There are yet to be available retention data of medium or long term stability in this case, however, we must be prepared to contain a possible relapse due perhaps to the proclination of the upper teeth and the retroclination of the lower anterior teeth, which would increase the overjet as reported by Fidler in 1995.16
To avoid this problem, it is suggested that according to the employed technique to perform fibrotomies of the teeth involved in the treatment.17–19
CONCLUSIONSTo achieve the desired results there are several diagnostic methods that support the obtaining of an individualized treatment plan and in this way achieve the visualized objectives.
Extractions in some cases remain a useful tool to achieve a proper occlusion, however, they must be planned properly.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia