









The use of mini-implants has revolutioned biomechanics in orthodontics with better results as far as anchorage is concerned. We have no limits when using these attachments depending only on our imagination. Anterior deep bites in severe class II malocclusion patients are a common problem that causes orthodontists to focus therapy in biomechanics to eliminate the problem by extrusion of posterior teeth or intrusion of the anterior. In this case, we decided to correct the anterior deep bite by intruding the incisors using as anchorage two mini-implants. The case was compromised by periodontal disease with moderated loss of alveolar bone so we had to choose biomechanics with a stable anchorage to achieve our goals. In the end, the patient exhibited collateral effects that were solved successfully and the deep bite was eliminated with great results and stable periodontal health.
El uso de miniimplantes ha revolucionado la biomecánica de la ortodoncia con mejores resultados en cuanto al anclaje se refiere. No hay límites al momento de utilizar estos aditamentos, y depende únicamente de nuestra imaginación. Las mordidas profundas en la región anterior son un problema frecuente en los pacientes con clase II severa, lo que nos obliga a enfocar nuestra terapéutica en una mecánica a corregir el problema mediante la extrusión de los dientes posteriores, o bien, mediante la intrusión de los dientes anteriores. En este caso, decidimos corregir la mordida profunda anterior mediante la intrusión de los incisivos superiores, utilizando miniimplantes como anclaje. Este caso estaba comprometido con la enfermedad periodontal con pérdida moderada de hueso alveolar, por lo que se escogió una biomecánica con un anclaje más estable para lograr los objetivos del tratamiento. Al final, el paciente presentó efectos colaterales que fueron resueltos exitosamente, la mordida profunda fue eliminada con grandes resultados y su salud periodontal fue más estable.
Anterior deep bites in severe class II malocclusion patients are a common problem that causes orthodontists to focus therapy in biomechanics to eliminate the problem by extrusion of posterior teeth or intrusion of the anterior.1 Since different situations can cause an anterior deep bite it is of the outmost importance to establish a correct diagnosis of the etiology of the increased overbite which will guide our treatment plan.1
Similarly, we shall consider each person’s periodontal health since we know that intrusion is the most complicated of orthodontic movements. The quality of the periodontal tissues will determine the course of treatment without preventing us from doing such mechanics.1,2
The current situation in the demand for orthodontic service has been revolutionized since adults are increasingly more concerned about their health and aesthetics, leaving behind the concept of orthodontics as a discipline focused only on treating adolescent patients.2
However, this comes with the obligation to consider the characteristics adult patients given that on numerous occasions we are likely to encounter people with active periodontal disease and lack of several dental organs so an appropriate treatment plan must be developed in order to solve the orthodontic issues without exacerbating the existing problem.2,3
Within the biomechanics for orthodontic correction of deep bites, control of anchorage in the vertical dimension is considered of utmost importance if the correction is intended by intrusion of the anterior teeth especially in those patients with dolicofacial characteristics or «long face» since extrusion of posterior teeth might increase these facial features.1,4
Many devices have been considered and used for anchorage control including intra- and extraoral appliances. However, in intra oral appliances a relative loss of anchorage has been observed; and regarding the extra-oral devices we depend largely on patient cooperation for its proper use. In the past, skeletal anchorage systems such as mini plates, palatal plates and mini-implants have revolutionized orthodontic anchorage and provided a much more stable anchorage.1,4,5 Several investigations have shown that mini-implants offer one of the best options for this purpose due to the multiple advantages they offer, mainly: easy management and placement in various anatomical areas as well as their low cost.4
Mini-implants offer stable anchorage when performing bio-mechanical movements that should be monitored clinically and radiographically for force control and thus help to preserve periodontal health and stability. The intended orthodontic mechanics should consider the use of flexible wires to allow free intrusive movement of the anterior teeth or the use of segmented arches that allow free movement of the posterior and anterior segments separately and the use of low force elastics to reduce the adverse effects that intrusive movements may produce.5
Materials and methods52 year-old male patient attends the Orthodontics Clinic of the Postgraduate and Research Department of the Faculty of Dentistry at the National University of Mexico. He is diagnosed as a combined skeletal class II patient with bilateral canine class II, nonassessable molar class due to the absence of these dental organs and controlled periodontal disease. For the treatment plan, the placement of 0.018 slot Roth prescription fixed appliances in both dental arches, a surgical phase II with corticotomy of the upper anterior segment and placement of two 7mm (Dewimed) mini-implants at the level of cul-de-sac between the roots of 12-13 and 22-23 is decided (Figure 1).
Results
After starting with phase I of orthodontic treatment and achieving a correct alignment and leveling of the anterior segments (Figure 2) an adequate correction of the overbite was accomplished thus eliminating the anterior deep bite.

This was made by means of the absolute skeletal anchorage provided by the mini-implants with vertical force vectors for the intrusion of the maxillary incisors (Figure 3).

However, the lack of vector control and the kind of forces produced by the elastics caused slight proclination of the incisors as a sideffect; to correct the incisor proclination a 0.016×0.016 stainless steel archwire with contraction loops to retract the anterior segment (Figure 4).

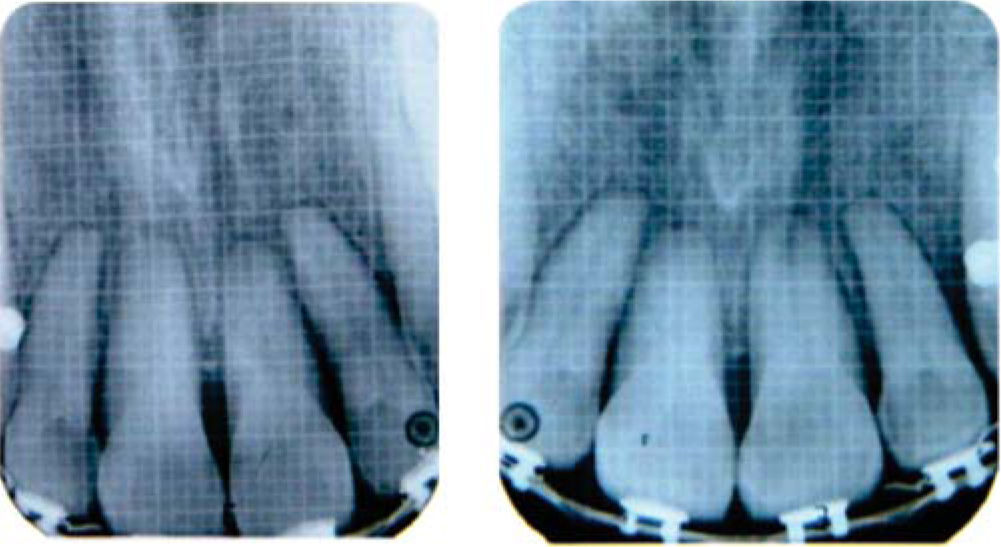
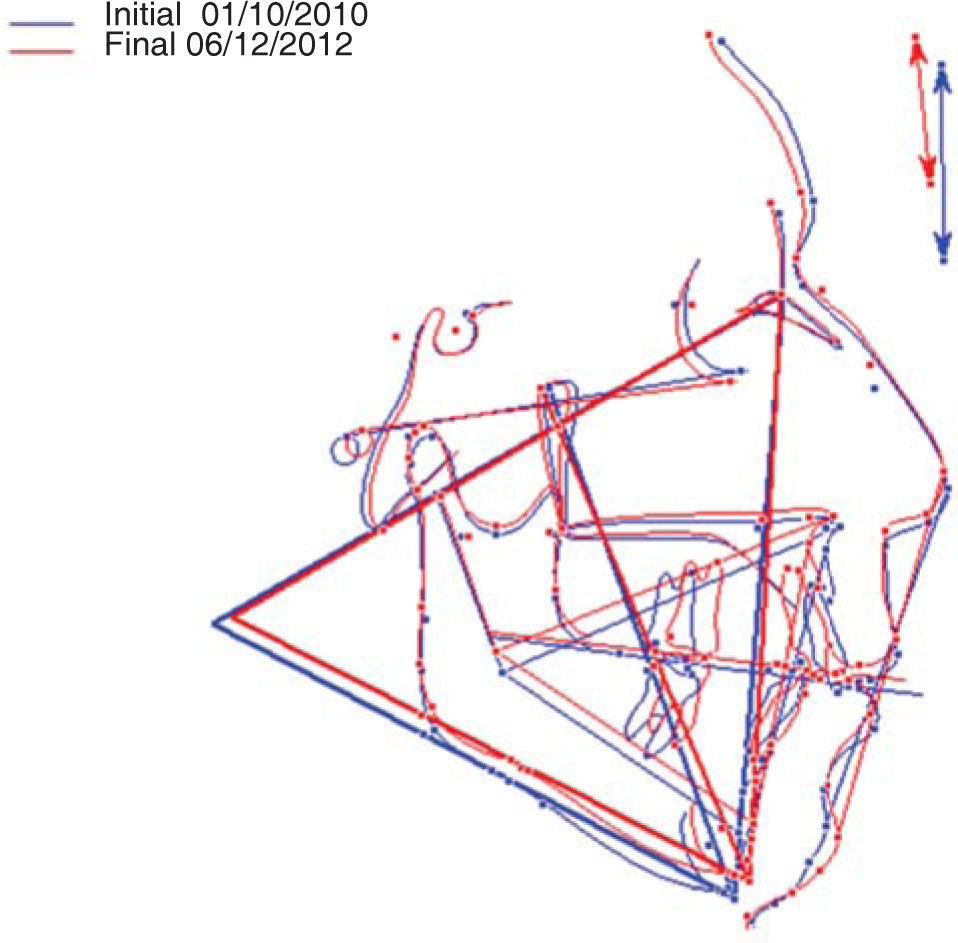
As a control measurement several radiographic and clinical images, initial and final cephalometric measurements of the anterior segments were taken to assess proclination and intrusion (Figures 5 to 7andTable I).



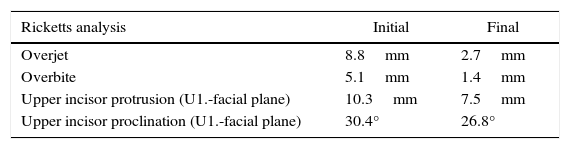
Cephalometric measurements regarding overbite and upper incisor position pre and postreatment (Ricketts analysis, VistaDent cephalometric measurement).
| Ricketts analysis | Initial | Final |
|---|---|---|
| Overjet | 8.8mm | 2.7mm |
| Overbite | 5.1mm | 1.4mm |
| Upper incisor protrusion (U1.-facial plane) | 10.3mm | 7.5mm |
| Upper incisor proclination (U1.-facial plane) | 30.4° | 26.8° |
However because of the treatment time along with the periodontal problems observed in the patient a hyperemia was observed in the dental organ # 21 which was refered to the endodontic clinic for treatment. On the other hand, the main problem of the overbite as well as of the overjet was corrected successfully (Figure 8).

Finally after having solved the main problem of the case, the occlusion was stabilized with the inherited restrictions that a periodontally compromised patient presents. Light force movements without excessive torque and tipping were performed to avoid complications in the periodontal health which is why an ideal occlusion is hardly obtained in this type of patients. However, alignment, leveling and stabilization of the case accomplish by themselves an important improvement in periodontal health and the occlusal function in these patients.
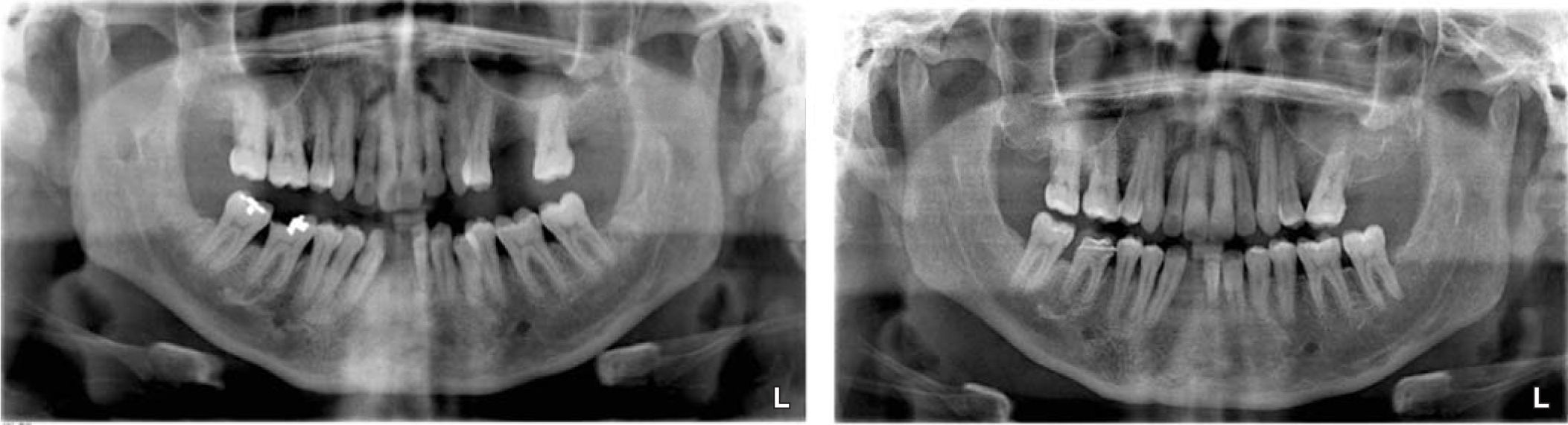
In the end, two different retainers were placed: fixed on the upper arch with a 0.014 stainless steel archwire on the labial surface of the teeth and a Hawley retainer with a provisional tooth to replace the dental organ # 41 on the lower arch. The initial and final panoramic X-rays were compared to assess the finishing of the case (Figures 9and10).


The stability and security that mini-implants provide when performing orthodontic movements that require an adequate anchorage control is evident when the results of the desired mechanics are observed. In cases such as the one presented herein who required special attention on the vertical dimension when conducting treatment for the excessive overbite, miniimplants are the best option to achieve intrusion of the anterior teeth.
Mini-implants have been reported as an option with many advantages for treatments that require a maximum anchorage to control biomechanic orthodontic movements.4,5 In those cases where the correction of a deep overbite is needed in a Class II adult patient it becomes necessary to focus treatment in correcting the overbite throght the intrusion of anterior teeth and not by extruding the posterior in order to maintain the vertical dimension as much as possible.1,5,6
It may be observed that the use of low force and high flexibility wires is of utmost importance when treating patients with periodontal disease even when it has been controlled with phase I periodontal treatment. This will allow us to perform light force movements that affect the least possible the periodontum stability in the afflicted areas.2,3,6 Likewise the use of round wires should be considered when performing intrusion movements to prevent the second and third order movements induced directly on to the bracket by the squared and/or rectangular archwire from affecting directly the tooth supporting tissues.1,6–8
That is why we recommend in periodontally compromised adult patients to focus on the best choice to correct deep bites that require greater care and attention when choosing the type of anchorage and orthodontic appliances needed for an increased stability in the final occlusion.
ConclusionsAccording to the observed results on this patients it can be established that mini-implants are an excellent choice when deciding on the necessary biomechanics and therapeutic options to correct anterior open bites in skeletal Class II patients. In addition to that, miniimplants offer many advantages from every point of view, however in cases where a maximum anchorage control and maximum vertical control are needed, they are the best option.
On the other hand, it is important to emphasize that the condition of periodontally compromised patients is not determinant for not receiving orthodontic treatment, on the contrary, it will provide them with a better functional periodontal and esthetic stabilization. And as far as biomechanics is concerned, intrusion movements in patients with bone loss accomplishes one of the objectives of periodontal treatment which is to regain bony level.