




Hypohidrotic ectodermal dysplasia (HED) is a rare genetic condition. It is of recessive autosomic character and linked to the X chromosome, encompassing a heterogeneous group of disorders involving ectoderm-derived tissues. Males are affected by the disease and females play the role of carriers. This disease presents a typical triad: hypohidrosis, oligodontia and hypotrichosis. This article examines the clinical case of a patient who exhibited characteristic signs of HED: dry skin, scarce hair eyebrows and eyelashes, wrinkles and peri-oral and peri-orbital hyperpigmentation, prominent lips and nasal bridge and decreased lachrymal secretion. Intra-oral examination revealed multiple tooth absences, presence of only eight teeth in the upper jaw and two teeth in the lower jaw, all with shape alterations and presence of diastemata. Early recognition and dental treatment of HED carrier individuals referred to oral alterations is of the utmost importance, not only to achieve favorable esthetics and functionality but also to allow the decrease facial growth alterations in a short time.
Displasia ectodérmica hipohidrótica (DEH) es una enfermedad genética rara de carácter autosómico recesivo ligado al cromosoma X, abarca un conjunto de desórdenes que envuelven tejidos derivados del ectodermo, siendo afectados el sexo masculino e portadores el sexo femenino. Presentan una tríada típica: hipohidrosis, oligodoncia e hipotricosis. Se reporta el caso clínico de un paciente con signos característicos de DEH: piel reseca, cabellos, cejas y pestañas escasos; arrugas e hiperpigmentación perioral y periorbitales; labios y puente nasal prominentes y disminución de secreción lagrimal. Al examen intraoral se observaron ausencias múltiples de piezas dentarias, con presentación de sólo ocho dientes superiores y dos inferiores, todos ellos con alteración de forma y presencia de diastemas. El reconocimiento y tratamiento odontológico precoz de los individuos portadores de DEH, referidos a alteraciones bucales es de vital importancia no solamente por ofrecer un aspecto funcional y estético favorables sino también porque permite en corto plazo reducir alteraciones en el crecimiento facial.
Ectodermal dysplasias are a heterogeneous group of alterations characterized by the abnormal development of ectoderm-derived tissues. Over 150 types of this disorder are known, the most common are hydrotic and hypohidrotic types. Hypohidrotic ectodermal dysplasia is the most frequent and severe variety.1,2
Hypohidrotic ectodermal dysplasia, also known as Christ-Siemens-Touraine syndrome, was first described by Wedderbun in 1838.2-5 Is a rare, genetic disease of recessive autosomic character linked to the X chromosome at the EDA1 gene located at the locus Xq12-q13.1.4-6 Males are affected by this disease and females are carriers.1-5 Its prevalence is about 1 case per 100,000 births.7 HED presents child mortality rate of about 2-20%, depending on timely diagnosis and treatment.8
Affected subjects exhibit a series of clinical characteristics with a typical triad: hypohidrosis, oligodontia and hypotrichosis. Afflicted subjects might exhibit the following manifestations: salivary and sweat glands alterations, scaling of the skin, fever episodes, asthma, breathing diffi culties, hearing loss, wrinkles around the mouth and orbits, peri-orbital hyperpigmentation, prominent lips, narrow and hypoplastic maxilla, heat intolerance, strabismus, conjunctivitis, premature cataracts, and in some cases polydactyly and syndactyly.1,2,8,9
Most frequent oral alterations are: oral xerostomia, alteration in number of teeth, such as complete agenesis, hypodontia, oligodontia, and amelogenesis imperfecta, shape alterations with frequent cone- shape teeth and/or microdontia both in primary and permanent dentition,7,9 moderate to severe presence of taurodontia, mainly in upper molars in cases when these teeth are present.2,10
Panoramic X-rays are the most commonly used auxiliary examinations in this type of anomaly. These X-rays help determine presence of tooth buds and dental anomalies which can be cases of oligodontia, teeth with shape alterations, especially coneshaped teeth, and severe generalized horizontal bone resorption. In most cases, present teeth are upper incisors, upper and lower canines, with lesser presence of premolars.2,3,11 Therefore, ectodermal dysplasia carriers will benefit from early diagnosis and treatment. For this reason, the target of the present project was to report the case of a typical clinical case detected during a routine dental visit.
CASE REPORT11 year old Caucasian male patient. Patient was detected during a routine clinical examination conducted at the Craniofacial Anomalies Rehabilitation Hospital, Sao Paulo, Brazil. Diagnosis was emitted after taking patient's history and conducting a general clinical examination.
Patient's history revealed continuous presence of unknown-origin hyperthermia as well as absence of teeth.
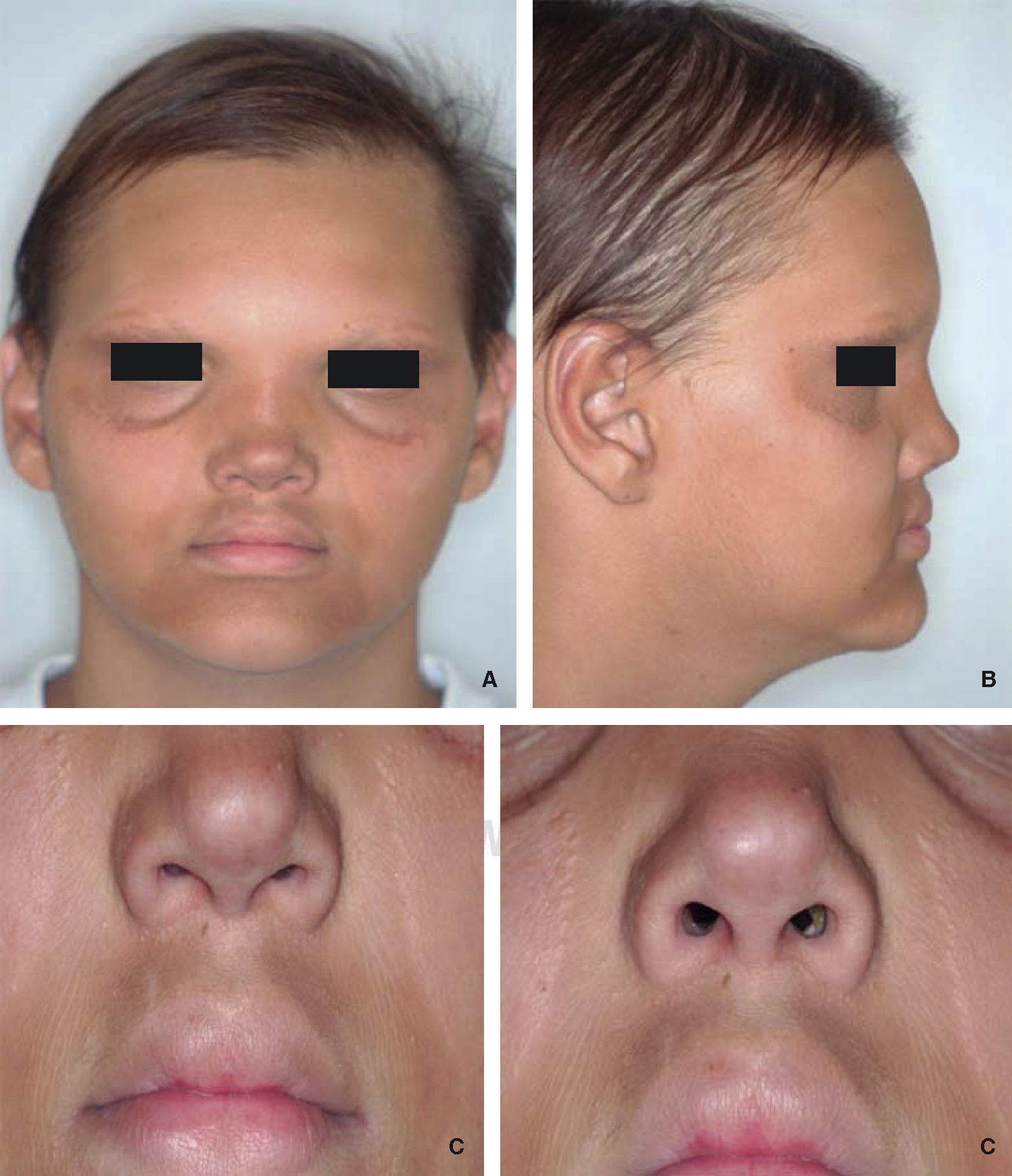
Clinical examination revealed hypohidrosis, with dry, delicate skin, decreased lachrymal secretion, scarce and very fine hair, eyelashes and eyebrows (hypotrichosis), prominent lips and nasal bridge, prominent forehead, presence of peri-oral and peri-orbitary wrinkles, periorbital and peri-oral hyperpigmentation, small sized nose with nostril hypoplasia (Figure 1).

Intra-oral examination established absence of many teeth, presence of all four upper incisors, all them with shape alterations in the crown, severe cone- shaped alterations in lateral incisors and presence of diastemata between them, cone shaped upper first premolars (right and left), upper first molars (right and left) as well as lower lateral incisors.
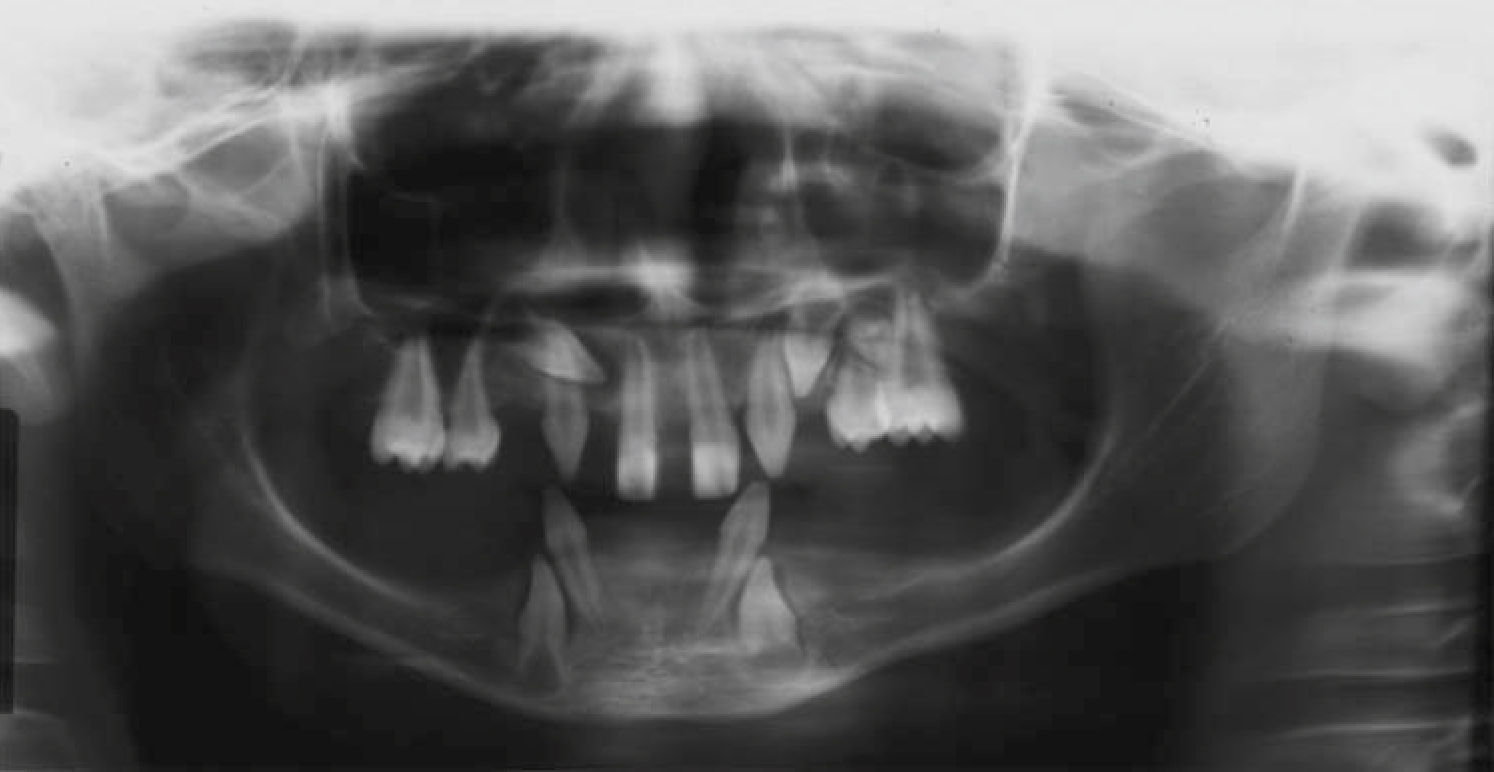
The patient was subjected to initial X-ray assessment, panoramic X-rays were taken as well as maxillary full occlusal computerized X-rays (Figures 2-4). Radiographic assessment revealed multiple tooth ageneses. Additionally to teeth observed at the intra-oral examination, erupting upper canines (right and left) were present, as well as a tooth bud at the level of the first upper left premolar; erupting lower canines were equally present, both with possibility of crown shaped alterations; generalized bone resorption was observed in both arches.



HED is an alteration which allows easy and timely diagnosis due to its characteristic presentation: hypohidrosis, hypotrichosis, and multiple tooth absences (oligodontia)12,13 as presented in the present clinical case.
Before the child's first year of life, one of the most worrying characteristics for the parents is the presence of hypohidrosis, which causes constant high temperature episodes; the child experiences a sensation of heat of unknown etiology, which prompts the parents to seek specialized care. During children's early ages, pediatricians have difficulties in establishing a diagnosis because they encounter normal patterns such as hyperthermia from birth onwards, nails can appear normal, there is no marked teeth eruption and hair is sparse.12-14
From the second year of life onwards, diagnosis of carriers of this alteration becomes easier. Dentists are the medical professionals most required in these cases, since they are the first to be consulted on multiple tooth absence and shape alterations which affect esthetic and functional aspects, and mainly the patient's quality of life.12-14
The case here presented informed of clinical and radiographic characteristics of a male patient. This is in accordance with literature reports which describe this condition as a gender-related recessive autosomal disorder.3,15
There are HED reports in scientific literature on clinical cases with different characteristics and alterations such as: poor dental occlusion with presence of diastemata, microdontia, shape alterations in crown and root, extensive and early tooth decay, enamel hypoplasia, altered pulp chambers, oligodontia, persistence of primary teeth, delays of permanent dentition eruption.2,7,11,12,13,15 Additionally, literature reports HED cases with presence of cone-shaped teeth, with decrease of mesio-distal dimension, as well as anodontia.6,13,15 Several of these characteristics concurred with those observed in the present case.
Within the scope of HED, scientific literature refers studies and clinical cases with different characteristics and alterations.
Some of the auxiliary examinations used to detect this type of alterations are extraoral X-rays, either panoramic or computerized. Full periapical occlusal X-rays are also commonly used so as to be able to determine the presence of tooth buds, bone resorption, bony profile, and placement of teeth in upper and lower jaws. With the help of these references, literature reports that lateral incisors, premolars and second and third molars are the permanent teeth most often absent in HED carrier subjects. Most stable teeth are upper central incisors, as well as upper and lower canines and first molars.3,11,13 Upper lateral incisors are the most commonly absent unstable teeth, followed by lower central incisors. Teeth most affected by morphologicall alterations also are upper central incisors and canines.14,15
The case here presented exhibited presence of all four upper incisors, with shape alterations, coneshaped teeth, erupting upper canines with apparent cone-shape, upper first premolars and first molars with taurodontia, tooth germ of the second left upper premolar. In the lower jaw presence of lateral coneshaped incisors and erupting lower canines with apparent cone-shape alteration. Severe horizontal bone resorption could also be observed in both jaws.
FINAL CONSIDERATIONSAfter establishing diagnosis, parents or tutors must be made aware of problems such as lack of sweating, so as to monitor heat and hyperthermia, dermatological and oral alterations. The importance of a multi-disciplinary approach must also be stressed, especially for dentists, so they always are willing to accept new challenges, that is to say, they must be trained to emit an early diagnosis when observing one of these patients during a routine consultation. Dentists must also be ready to rehabilitate a patient so as to achieve clear positive changes, not only in the functional and esthetic aspects but also with respect to patient's emotions and quality of life.