



To determine the relationship between traumatic occlusion and abfractions and their role in pulp disease.
IntroductionIn many teeth lesions might have their onset at the cement and enamel junction; caused by loss of hard tissue, these lesions might appear at vestibular or lingual sides, and are frequently accompanied by tooth sensitivity.
Material and methodsCross-sectioned observational study with analytical component. Size of sample and inclusion materials: subjects exhibiting dental abfraction caused by traumatic occlusion, who suffered some pulp consequence. Excluded from the study were patients suffering caries, erosions, fillings, previous orthodontic or endodontic treatment, fractures fissures, or dento-alveolar trauma.
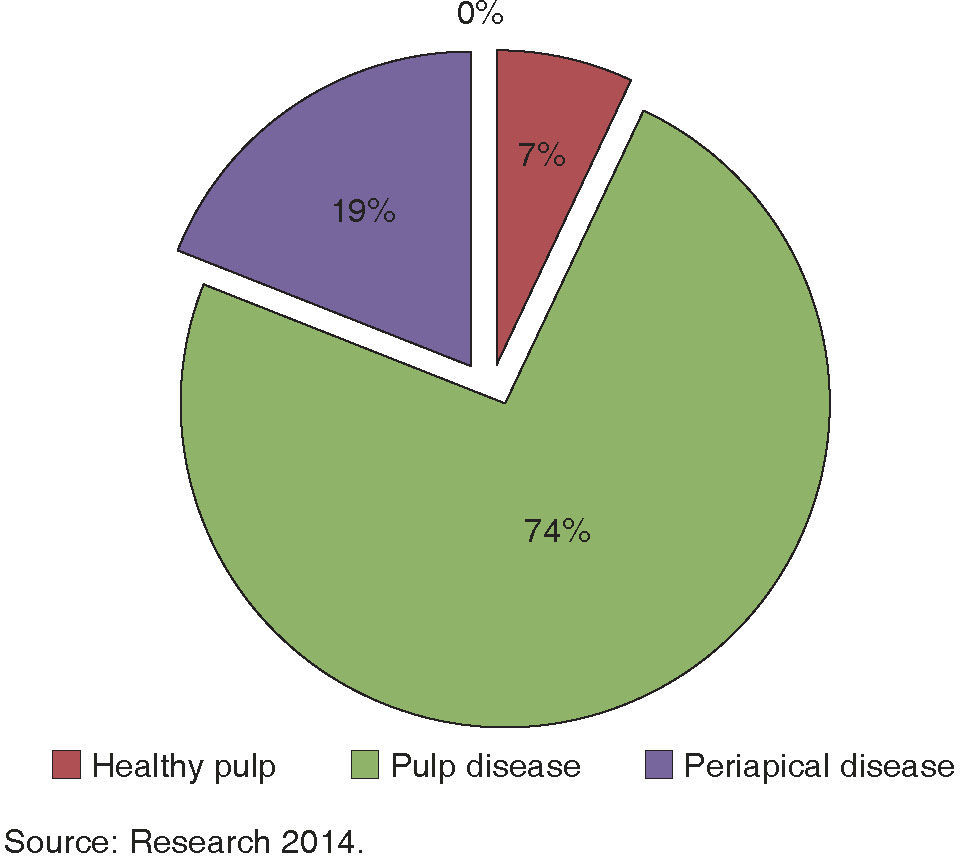
ResultsThe study included 85 patients, out of them 22 exhibited abfractions, gathering a total of 64; 78% showed wear facets. Upper premolars exhibited most prevalent abfractions; 7% presented healthy pulp, 74% pulp disease and 19% periapical compromise.
ConclusionsA relationship was found among variables of traumatic occlusion and abfraction, the aforementioned, in combination with other factors can lead dental pulp to suffer pathological conditions.
Determinar la relación entre la oclusión traumática y abfracciones; su rol en las afecciones pulpares.
IntroducciónEn los órganos dentarios, se puede manifestar una lesión por pérdida del tejido duro en la unión amelocementaria ya sea en vestibular o lingual, pudiéndose acompañar generalmente de sensibilidad dentinaria.
Material y métodosEstudio observacional de corte transversal y componente analítico. Tamaño de la muestra y criterios de inclusión: sujetos que presentaron abfracción dental producto de oclusión traumática y que tuvieron alguna consecuencia pulpar. Se excluyeron aquéllos que presentaron caries, erosiones, obturaciones, tratamiento de endodoncia u ortodoncia, fractura, fisura, o por traumatismo dentoalveolar.
ResultadosSe estudiaron 85 pacientes; 22 presentaron abfracciones, obteniéndose un total de 64. El 78% mostró facetas de desgaste. Los premolares superiores fueron los más prevalentes de abfracciones. En la etiología de la oclusión traumática, las interferencias oclusal fueron más prevalentes. El 7% presentó pulpa sana, 74% afección pulpar y 19% periapicales.
ConclusionesSí existe una relación entre las variables oclusión traumática y abfracciones, éstas, en combinación con otros factores, pueden conducir a la pulpa dental a un estado patológico.
In human beings, soft and hard tissues are of the utmost importance, therefore any factors that might cause them to change will affect the integrity of their structure and function. With respect to teeth, lesions can appear at the enamel-cement junction in both vestibular and lingual aspects; these lesions are frequently accompanied by tooth sensitivity, this non-infectious entity is called abfraction (Figure 1); it is caused by eccentric occlusal forces which lead to dental flexion,1,2 it is presently known as flexural stress, tensile stress or compression syndrome, since the lesion is evidence of a set of signs (loss of wedgeshaped tooth structure and repeated restorations’ fracture and detachment) as well as symptoms (dentin hypersensitivity) when the lesion is active.2

In those cases when traumatic occlusion causes tension, teeth experience two types of tension: traction or elongation and compression or flattening. In these cases, cervical enamel prisms collapse, that is to say tensile stress, concentrate on the cervical fulcrum.3,4 Due to the fact that hydroxyapatite crystals are unformed and vulnerable, they exhibit lesser mineralization and greater porosity;4 additionally due to absence of cells, they cannot self-regenerate when their integrity is compromised,5 and then, a process of dentin and enamel fracture is initiated, which in dentin can reach 3 to 7 μ2. This process produces microscopic loss which exacerbates as the lesion progresses. It can be microscopically observed shaped as a deep wedge with cracks and striations, with rough angles ranging from 45 to 120 degrees and well defined margins. They can appear in multiple surfaces of a single tooth, and are rarely circumferential in shape.6 According to affected tissue, they are grouped into three types: I :only enamel is affected, II: Enamel and dentin are affected, III: it practically reaches the pulp chamber.7
Cervical lesions in teeth do not stop there, they expose dentin as a result of the loss of natural protection tissues such as enamel, or gingival and root cement; lesions progress to soft tissues of the tooth such as dental pulp.8 Hypersensitivity can take place when protecting hard tissues of the tooth, especially dentin which is more soluble and soft than the enamel;9 this can be due to exposition of dental tubules which have lost their natural sealing, and upon nearing the dental pulp, their diameter increases along with dentin permeability. This is concordance with Bräanström's10 hydrodynamic theory, which results in a movement of dentin fluid which in turn causes stimulation of a great amount of nerve ends in the peripheral area of the pulp cavity, a fact which would explain the intensity of the pain.8 Pain is defined as an unpleasant emotional and sensitive experience associated to real or potential tissue damage.11 Hypersensitivity is described as a sensation of acute pain elicited in response to an evaporative, tactile, chemical or osmotic stimulus, which cannot be attributed to any other defect or oral condition. This situation is reported in a wide margin of the population (4 to 57%) especially in adults (20 to 40 years) as well as in females.10
Finally, it has been mentioned that there are forces and tensions which indicate that occlusal loads indubitably play a major role in development of lesions compatible with abfraction.12
The aim of the present study was to establish relationship between traumatic occlusion and abfractions as well as their role in pulp conditions in patients treated at the General Hospital of Merida, Yucatan, Mexico, during 2014.
MATERIAL AND METHODSThe present was a cross-sectioned, observational and analytical study. It was conducted in patients who sought dental treatment at the Southern area of the General Hospital, Merida, Yucatan Mexico, where a «people's medical service» is offered. This service provides comprehensive medical treatment to low income population of Yucatan or other Mexican states which might require treatment; service is not denied to anyone. Sample was taken during 2014. Sample size and inclusion criteria were the following: subjects exhibiting dental abfraction caused by traumatic occlusion and who experienced some pulp consequence. Cases excluded were the following: subjects exhibiting caries, erosions, fillings with any sort of temporary or permanent material, endodontic or orthodontic treatment, fractures, fissures, dentoalveolar trauma (concussion, intrusion, extrusion, etcetera).
Methodology: All patients submitted: 1) an informed and voluntary consent letter, which they read or was read to them; all their queries were answered cordially and with simplicity, no time was spared to achieve this important section of clinical research. Ethics Committee is in the process of formation. Participants were treated with dignity, respect, responsibility, justice, equity, confidentiality and at no charge. Once the patients understood the objective and methodology to be imparted, when they decided to participate they signed or printed their fingerprint. 2) A research cell was made up, with a questionnaire including demographic data of the patient (name, age, gender, place of origin etcetera. 3) By means of objective diagnosis and based on NOMS 013 (Norm of the Ministry of Health)13 for infection control, a USA DELTA® number 5 explorer was used, this instrument played the role of diagnostic tool. Cervical morphology of all teeth was examined in order to determine whether they presented any type of wedgeshaped non carious lesion along the cervical margins of the tooth, called abfraction. All details were noted in an odontogram (attached to the research identity card) to identify affected teeth, this was conducted with the two digit system. 4) Additionally, an occlusal examination was conducted (pathological or adaptation alterations caused in periodontal tissue and dental pulp as a result of undue and/or excessive forces produced by masticatory muscles according to criteria used by Peter Dawson to define traumatic occlusion).14 To this effect, a Miller® brand clamp as well as 80μ red and blue articulating paper (ROEKO®) were used in order to obtain precise relief of masticatory forces distribution at both maximum intercuspation and laterality, thus precisely and accurately marking premature contacts of occlusal interferences. Teeth exhibiting premature contact points were examined. That is to say, necessary interocclusal contacts did not take place simultaneously in centric occlusion. Obtained data of traumatic occlusion were noted in the same research identity card. 5. Once diagnosis of abfractions and traumatic occlusion was obtained, a questionnaire on symptomatology questionnaire was tailored according to instructions of the American Association of Endodontics (AAE),15 which includes pain history: frequency, duration, type of stimulus, type of pain and intensity, along with endodontic clinical tests which included: a) Thermal tests, (hot and cold, whether positive stimulus was elicited with hot water, or more specifically, with a hot gutta-percha point on the suspected tooth, and cold if it provided positive stimulus to Endo Ice® on a cotton hyssop applied to the suspected tooth for 4 seconds). Different responses to pulp afferents to thermal tests could determine pulp health or disease. b) Sensitivity with Visual Analog Scale where the patient observed graphic representation of a 10cm horizontal line where 0 is absence of pain and 10 maximum pain. The patient was instructed to mark a point in the line to note the amount of pain he experienced according to his individual perception, measuring thus the pain in centimeters from point zero (no pain) to where he marked his point; thus mild pain was established at 1 to 3cm, moderate pain from 4 o 7cm and severe pain at 8 to 10cm. c) palpation and d) percussion (palpation and percussion could show involved teeth, nevertheless, percussion could give positive response to pain in cases where there was a previous periapical lesion, thus indicating inflammation). It is necessary to conduct percussion in teeth adjoining the supposedly affected tooth. Nevertheless, this procedure did not clarify whether pulp or periodontium was affected, for this reason, all necessary pulp tests were conducted, and d) with diagnostic approach: staining and transillumination (to observe presence of caries, fissures or fractures) were conducted with dental lamp , placing a fibre optic light beam (Ardent®) at the vestibular, buccal and interproximal aspects of the suspected tooth, that is to say, the light beam was placed perpendicularly to the plane in which it was suspected to find a fracture or fissure, and measurement was taken from the other side. In order to establish exclusion criterion, it was of the utmost importance to ascertain it did not exhibit fissures of fractures.6 Periapical X rays were taken of all affected teeth pulps in order to establish pulp diagnosis.
Square chi goodness of fit test was used for two categories (with Yates correction).16 The following factors were compared: 1) number of patients with abfractions with respect to age groups, 2) whether teeth have or lack facets, and 3) periapical disease. This test was likewise used to compare patients with abfractions according to gender. The following was compared using chi square test for goodness of fit to uniform distribution or equal proportions;16 1) number of patients with abfractions among different age groups; 2) number of teeth with abfractions according to a) occlusal trauma etiology, b) condition, c) type of pulp disease, d) quadrant. Results of statistical tests were considered significant when p < 0.05 and statistical package SOPSS15 was used.17
RESULTSThe study comprised 85 patients, who exhibited 22 abfractions; 15 females (68%) and 7 males (32%), no statistically significant difference was found between genders (χ2 + 2.2273, p = 0.1356, g.I. = 1).
In these patients, 64 abfractions caused by occlusal trauma were obtained. According to location of cervical lesions, 59% were found in the supragingival vestibule and 41% presented lesions in the subgingival vestibule. Location of abfractions did not significantly differ according to whether they were in a supraor sub-gingival location (χ2 = 1.8906, p = 1.691, g.l. = 1).
On the other hand, 5 grade I abfractions were found (only enamel affected), 34 grade II abfractions were observed, (encompassing enamel and dentin) and 25 grade III abfractions were encountered (implicating enamel, dentin and chamber or root pulp).
Out of all these lesions, 78% showed wear facets and 22% did not, therefore a significant difference was found (χ2 = 19.1406, p < 0.0001, g.l. = 1).
With respect to teeth affected according to quadrant the following was found: Most prevalent was upper right with 34%, upper left 27%, lower left 29% and lower right 20%.
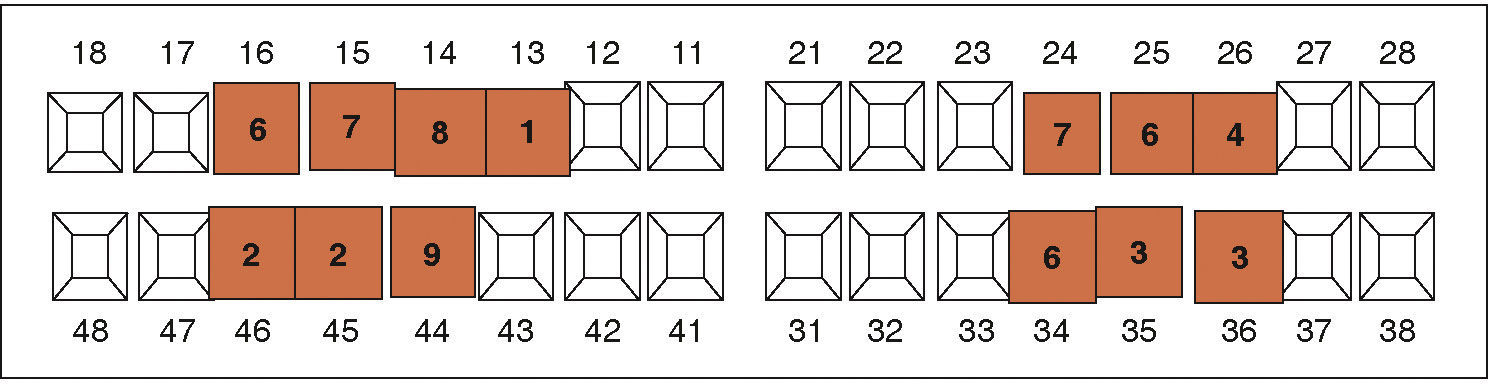
Figure 2 shows distribution of abfractions according to affected teeth, where no significant difference was found (χ2 = 3.8750, p = 0.2753, g.l. = 3). Nevertheless, it must be noted that upper premolars exhibited greater frequency of abfractions.

With respect to traumatic occlusion etiology the following was observed: premature contacts 28%, occlusal interference 64%, and lastly, bruxism parafunction 8%, thus, statistically significant differences were found (χ2 = 31.1563, p < 0.0001, g.l. = 2).
When considering abfractions according to age group, the following was found: age range 18-35, 35%; 36 to 50, 41%; 51 to 65, 27% and finally 66 to 80, 5% respectively. No statistically significant difference was found (χ2 = 6.0, p = 0.1116, g.l. = 3).
Figure 3 shows results among pulp conditions, statistically significant differences were found (χ2 = 47.4688, p < 0.0001, g.l. = 2).

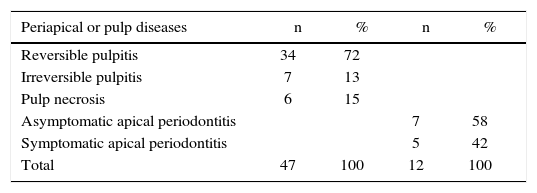
Table I shows periapical and pulp diseases.
Periapical and pulp disease in 59 teeth with abfractions and traumatic occlusion, Merida, Yucatan, Mexico 2014.
| Periapical or pulp diseases | n | % | n | % |
|---|---|---|---|---|
| Reversible pulpitis | 34 | 72 | ||
| Irreversible pulpitis | 7 | 13 | ||
| Pulp necrosis | 6 | 15 | ||
| Asymptomatic apical periodontitis | 7 | 58 | ||
| Symptomatic apical periodontitis | 5 | 42 | ||
| Total | 47 | 100 | 12 | 100 |
Source: 2014 Research.
Statistically significant differences were found according to pulp condition (χ2 = 32.2128, p < 0.0001, g.I. = 2) whereas in periapical disease no statistically significant differences were found (χ2 = 0.0833, p < 0.07729, g.l. = 1).
DISCUSSIONLatorre C et al3 reported the case of a 35 year old male, who exhibited 4 teeth with abfractions in all 4 upper premolars; functional examination of that patient revealed occlusal interferences in right and left sides with laterality movements, thus, traumatic occlusion was diagnosed. Endodontic diagnosis after assessing vitality of teeth was as follows: 24 teeth with vital pulp, 6 teeth with irreversible pulpitis, in coincidence with all 4 upper premolars, and 2 teeth with pulp necrosis. The clinical case reported by Latorre et al3 showed similarities with the present study in the fact that traumatic occlusion was related to teeth with higher abfraction prevalence, these teeth were upper premolars and additionally presented pulp conditions.
Mucenic S et al18 conducted a study on biomechanisms of abstractions; results revealed that when using loads of increased magnitude in vertical and traction positions, cervical areas received the greatest amount of tension, becoming thus prone and more sensitive to mechanical damage that manifests as abfractions. This concurs with our research when considering that abfractions of affected teeth are probably consequence of occlusal trauma.
Consolaro A19 in his literature review, mentions that abfraction is common, especially in young adults and in premolars, concurring with the present study which found that premolars were the most prevalent teeth with abfractions.
Amaiz Flores AJ20 in his literature review article mention Estefan et al, 2005, who expressed that non carious cervical lesions can be found in teeth exhibiting occlusal wear facets. This is in agreement with our study where a high percentage of occlusal wear facets was found in teeth with abfractions.
Likewise, Romero F1 mentions that out of 110 studied patients, 48 presented abfractions, and out of these, 81% exhibited abfractions at ages ranging from 45 to 59 years. This would indicate the existence of a statistically significant association between age and abfractions p < 0.005. This differs from the present study where age groups were not statistically significant. Conversely, we do concur with Romero1 in proposing that premolars are the teeth exhibiting greater number of abfractions. Nevertheless we do not agree with the fact that lower premolars are the most affected, since, in our study we found that upper premolars were the most affected.
In his thesis to earn a DDS degree, Segura Escudero JS21 studied 80 patients aged 18-60 years, who attended the Rapid Response Service of the School of Dentistry, National University of Mayor de San Marcos in Lima, Peru, in 2013. In that study he obtained results indicating that 66 patients (82.5%) exhibited non carious cervical lesions, observing that neither age nor gender of patients were of statistical significance. On the other hand, 39 patients exhibited abfractions out of the total of non carious cervical lesions. He also studied the relationship between abfractions and presence of interferences in left laterality movements, he reported significant difference between these two variables. Likewise, in our study, no significant difference was found with respect to age and gender. Likewise, in both studies (Segura/Mendiburu) number of abfractions and occlusal interferences differed significantly thus it can be assumed there is a relationship between abfraction frequency and presence of occlusal interferences, which represents a significant datum for the present study.
Cuniberti de Rossi NE, Rossi G12 in their book written in 2009, provide and explanation of abfractions geneses and their presence at subgingival level. Nevertheless, in the present study higher supragingival abfraction frequency was observed, allowing thus, a more feasible diagnosis.
CONCLUSIONSDental complications, either infectious or noninfectious, are a public health issue, since they affect high percentages of the population. Affected subjects frequently lack knowledge of the relationships existing in the different parts of the stomatognathic system.
It must be noted that abfractions are found with no statistically significant difference according to age and gender, that is to say, they are found equally in males and in females, and can appear at any age group.
In the present study, we found presence of relationship between the variables traumatic occlusion and abfractions; the latter, in combination with other factors, can cause disease of the dental pulp.
If left to pursue their natural course along with traumatic occlusion, abfractions can cause dentin hypersensitivity as well as other types of afflictions leading to pulp or periapical disease.
High prevalence of grade II and grade III abfractions was observed, which means that a high percentage of the population suffering from abfractions caused by occlusal trauma suffer some grade of dental hypersensitivity which could elicit unnecessary pain when ingesting food, talking, yawning, etc.; all the aforementioned bear influence in the subject’ s quality of life.
This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam
Full time professor at the School of Dentistry, Autonomous University of Yucatan, Mexico, Graduate degree in Research and Imaging.
General Physician, Graduate, School of Medicine, Autonomous University of Yucatan, Mexico.
Full time instructor and coordinator of Restorative Dentistry Specialty School of Dentistry of the Autonomous University of Yucatan, DDS, Specialty in Restorative Dentistry, Master's Degree in Dentistry.