


To determine prevalence of temporomandibular joint disorders signs and symptoms of elderly adults in Medellin as well as related factors.
Material and methodsThe present was a crosssectional study conducted at the «Metrosalud» hospital network. The study was composed of 342 adult patients ≥ 65 years, (57.8% females) Variables: Socio-demographical and social support (Duke- 11); Self-perceived stress, mental health, self-perceived general health, satisfaction with respect to dental circumstances, self-perceived oral health, oral problems (previous 30 days), number of teeth present, presence of prostheses (upper/lower), Helkimo Anamnestic Index and clinical assessment. Prevalence of temporomandibular joint disorders- Helkimo Anamnestic Index was assessed with respect to health and socio-demographic variables, temporomandibular joint disorders was assessed according to clinical evaluation. Association between temporomandibular joint disorders-Helkimo Anamnestic Index and health indicators was evaluated as well as clinical temporomandibular joint disorders by means of logistic regression calculating crude and adjusted Odds Ratio with 95% (CI95%) confidence intervals.
ResultsPrevalence of severe symptoms was higher in males (32%), females exhibited higher prevalence of mild symptoms (18.8%); differences were found according to socio-demographic factors. Subjects reporting symptoms tended to report higher prevalence of poor oral and general health indicators. Higher association was found for patients with dental problems in the previous 30 days. (aOR 3.57; CI95% 1.80-7.08) in the case of women and, for men, the indicator was poor mental health (aOR 2.83; CI95% 1.31-6.09) Even though females exhibited greater risk of reporting TMJ related problems (except for the presence of articular noises) no statistical significant associations were found.
ConclusionsFurther epidemiological surveillance systems are required in order to suitably and clearly establish associations found in the present study.
Determinar la prevalencia de signos y síntomas de trastornos temporomandibulares en adultos mayores de Medellín y sus factores relacionados.
Material y métodosEstudio transversal en la red hospitalaria «Metrosalud». Participaron 342 adultos ≥ 65 años (57.8% mujeres). Variables: sociodemográficas y apoyo social (Duke-11); estrés autopercibido, salud mental, salud general autopercibida, satisfacción estado dental, salud bucal autopercibida, problemas bucales (últimos 30 días), número de dientes presentes, presencia de prótesis (superior/inferior); índice anamnésico de Helkimo y evaluación clínica. Se calculó la prevalencia de trastornos temporomandibulares-índice anamnésico de Helkimo según variables sociodemográficas y de salud y de trastornos temporomandibulares según evaluación clínica. Se estimó la asociación entre trastornos temporomandibulares-índice anamnésico de Helkimo e indicadores de salud y trastornos temporomandibulares clínicos mediante regresión logística calculando Odds Ratio crudas y ajustadas con intervalos de confianza al 95% (IC95%).
ResultadosLa prevalencia de síntomas severos fue mayor en hombres (32%) y de síntomas leves en mujeres (18%), con diferencias según factores sociodemográficos. Las personas que reportan síntomas tienden a reportar mayores prevalencias de malos indicadores de salud general y bucal. La mayor asociación se encontró para los problemas dentales en los últimos 30 días (ORa 3.57; IC95% 1.80-7.08) en el caso de las mujeres y para los hombres en mala salud mental (ORa 2.83; IC95% 1.31-6.09). Aunque las mujeres presentaron mayor riesgo de reportar problemas relacionados con la ATM (excepto para la presencia de ruidos articulares), no se encontraron asociaciones estadísticamente significativas.
ConclusionesSe requieren sistemas de vigilancia epidemiológica que permitan establecer con mayor claridad las asociaciones encontradas.
Demographic changes have been taking place in the last decades, especially in Latin America and the Caribbean. These changes show gradual increase of elderly people, identifying as elderly subjects above 65 years of age. This situation can be explained by cultural, political financial and social phenomena, among which we can count decrease in birth rates, increase of population life expectancy, decrease of mortality rates, control of infectious and parasitic diseases, improvement of sanitary circumstances, attenuation in population increase rhythm as well as migration processes.1–3
In Colombia it is anticipated that by 2020 elderly population will reach 10% of total population.4 This situation represents a challenge for the country with respect to social policies, resources, enforcement of rights, and especially guarantee of quality of life and comprehensive health care for this elderly population.5
In an elderly patient, comprehensive health is mainly defined in terms of preservation of functionality, independence and autonomy; its main components are suitable mobility and neuro-cognitive function.2 Oral health, as part of general health has been defined as «physical, psychological and social well being with respect to dental circumstances as well as its linking with soft and hard tissues of the mouth». Health of the oral cavity is essential for vital functions such as feeding, communication, affection and sexuality, in addition to its relationship with physiological and psychological aspects as well as social relationships.6
In elderly patients, oral morbidity profile is generally deficient, with loss of teeth, presence of dental caries, high prevalence of periodontal disease, xerostomy, lesions of the oral mucosa (pre-malignant and malignant) as well as temporomandibular joint disorders. The latter have been identified as a series of alterations with clinical signs and symptoms related to temporomandibular articulations and the muscles surrounding them. Frequently TMJ disorders are a combination of muscle tension, anatomical problems within the articulation, psychosocial alterations, parafunctional habits, trauma and alterations in tooth occlusion.7,8
The Third National Study of Oral Health (Estudio Nacional de Salud Bucal III ENSAB) showed that subjects over 55 years of age exhibited high prevalence of severe symptoms related to temporomandibular disorders.9 Nevertheless, results of national and international studies show extremely variable prevalence rates, which in turn indicate that symptoms related to temporomandibular disorders tend to decrease in elderly subjects, whereas clinical signs increase with age.8,10,11 In Colombia there are few specific studies on this subject.
Relevance of providing clarification of real circumstances of temporomandibular disorders found in elderly patients lies in the fact that early detection and proper handling of these disorders contribute to avoid a progression to masticatory function deterioration, as well as nutritional circumstances, speech, presence of myofascial pain, perception of health and, in general terms, quality of life of elderly population. Thus, the objective proposed for the present study was determination of temporomandibular disorders’ signs and symptoms prevalence in elderly patients treated within the hospital public network in Medellin as well as related factors.
MATERIAL AND METHODSDesign and information sourceThe present was a cross-sectional study. Studied population was composed of elderly patients attending the outpatient services of the Metrosalud Health Service in Medellin. Subjects of the study were males and females aged 65 years or over, selected from first time visit recordings, gathered by the statistics unit of the institution for the year 2011. The following patients were excluded: subjects with hearing or visual disability, subjects systemically compromised unable to attend the institution (since no home care was contemplated) as well as subjects refusing to participate in the study.
Initially, a total sample of 354 elderly subjects was selected by means of a two stage design: At a first stage, the facilities and health centers to take part in the sample were selected, after this, the sample was proportionally allotted to each of these facilities and centers. For the present analysis, information on 342 elderly subjects was used (58.2% females), which, after data depuration, constituted 97% of the total sample.
In summary, the wider scope project contemplated use of structured survey and full dental examination including information of socio-demographic data, self-perceived health variables (mental, general and oral), use of oral health services, quality of life related to oral health, temporomandibular articulation examination, oral mucosa, soft tissue evaluation, as well as prosthetic, dental and periodontal examination. Field work was conducted between the months of March-December 2013, and was performed by a team which was standardized for survey and clinical examination performance. In clinical examinations a concordance level of over 80% was guaranteed (intra and inter observer) which was deemed acceptable for the objective of the study.
VariablesThe following socio-demographical variables were considered: age, education level (no education, primary school, secondary school-university) socioeconomic level (low, middle) occupation (obtained from the occupations international classification accepted in Colombia);12 occupation was classified into non manual (directorships, university professionals, scientists and intellectuals, technicians, non university secondary teachers and assistants, office workers, service workers and salespeople (merchants), manual workers (agriculture, industry construction and non-qualified workers), housework and others (retired and students); residence area: (rural, urban); social support: Duke-11 profile was used, which is a questionnaire or survey composed of eight sentences which are graded according to five categories of Likert scale, ranging from «much less than I desire» (which rates 1 point) to «as much as I desire» (which rates 5 points). In order to obtain scale punctuations, obtained values were added to the sentences, punctuation range varied from 11 to 55 points, the greater the number of points, greater will be the perceived support. To consider perceived social support as low, a punctuation cutting point of < 32 was established.13
The following health related variables were studied: Self perceived stress (yes/no), mental health was measured with a 12 question General Health Questionnaire (GHQ-12); this questionnaire purports the aim of conducting a screening of present mental disorders.14 Following category 4 in the Likert scale, the subject is requested to report whether he has recently experienced a given symptom. In the four response categories, 0 was allotted to answers 1 and 2, and 1 was allotted to answers 3 and 4. Poor mental health was allotted to a cutting point of punctuation ≥ 3, according to other studies in populations of similar context,15 self-perceived general health (good/poor) satisfaction with respect to state of teeth and mouth (satisfied, dissatisfied); self perceived oral health (good/poor), oral problems in the last 30 days (yes/no), number of teeth present (20 and more ≤ 19) presence of oral and dental prostheses (yes/no).
The following factors were considered in order to assess presence of signs and symptoms of temporomandibular joint disorders: 1) Helkimo (HI) anamnesic index. This index is conducted through posing the patients 7 questions which assess presence of noises, pain or muscle fatigue. According to this, classification was: no symptoms, mild symptoms and severe symptoms; 2) clinical examination in which the following was considered: clinical assessment of presence of noise, pain upon lateral and posterior palpation, pain in masseter, pterygoid and temporal muscles. At a later point this was re-classified into noise, functional pain and muscle pain (Yes/No). The aforementioned were adapted from instruments used in the III National Study of Oral Health9 (Estudio Nacional de Salud Bucal). Although there were other indicators for the diagnosis of temporomandibular disorders16–18 it was decided to use HI as comparability and as screening test, taking into account scarcity of studies on the subject.
AnalysesAnalyses were separately conducted for males (M) and females (F). First of all evaluation was conducted of relative frequencies (prevalence) of signs and symptom’ presence through HI according to socio-demographic characteristics as well as health indicators under consideration. At a later point clinical symptoms prevalence according to gender was determined, calculating square Chi for the difference of proportions. In a third place, association between presence of subjective signs and symptoms (HI) with health indicators was estimated; this was achieved through non conditional logistic regression, calculating Odds Ration (OR) with confidence intervals to 95% (CI 95%) in raw form, to later adjust it according to sociodemographic variables. Finally, association between gender and presence of subjective (HI) signs and symptoms as well as through clinical examination was established by means of the aforementioned logistic regression procedures.
EthicsThe present study was approved by the Comité de Ética de Investigación (CEI) (Research Ethics Committee) of the METROSALUD institution, according to notary certificate 09-2011. In order to participate in the study, elderly subjects had to grant written and verbal consent; informed consent was requested from the elderly subjects, confidentially and respect for acquired information were guaranteed. The present study complied with national and international norms for research in human beings, and was classified as entailing minimum risk.
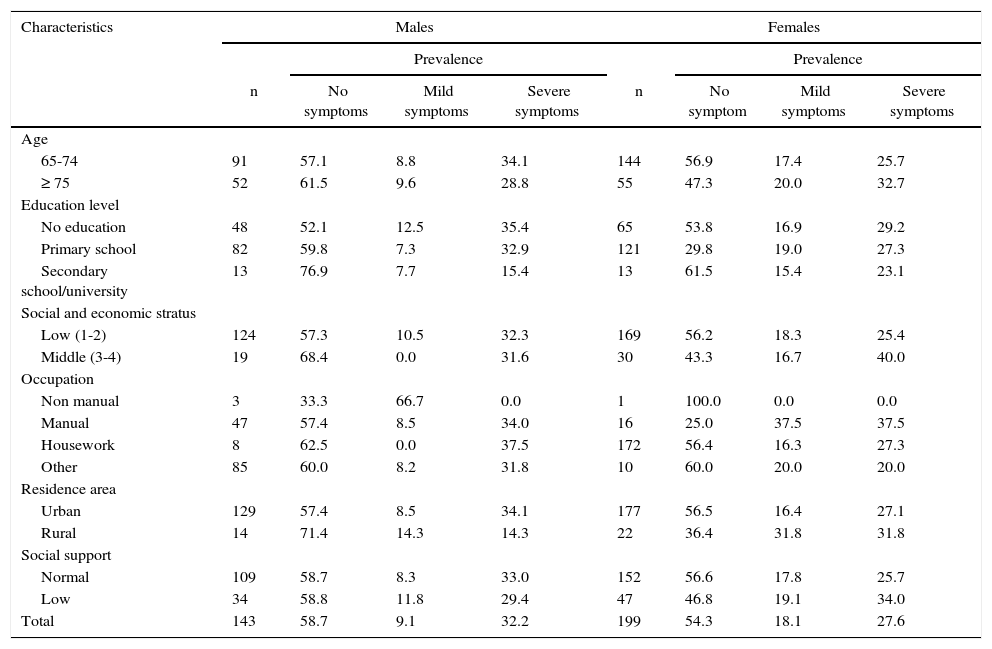
RESULTSTable I shows prevalence of subjective signs and symptoms according to socio-demographic characteristics. In general terms, prevalence of severe symptoms was higher in males (32%) whereas females exhibited higher prevalence of mild symptoms. Higher prevalence of severe symptoms was found in females aged 75 years and over (33%), in males and females lacking academic background (M: 35%, F: 29%), in males of low social background (32%) and females of middle economic stratus (40%). With respect to life occupation, higher prevalence of mild symptoms was found in males engaged in nonmanual labor, (67%), severe symptoms were reported by subjects devoted to housework (38%), whereas in females, prevalence was higher for those engaged in manual labor (38% for mild and severe cases). With respect to area of residence, prevalence of mild and severe symptoms was higher in females residing in rural areas, (32% in both cases). Males with scarce social support exhibited higher prevalence of mild symptoms (12%), females with scarce social support exhibited higher prevalence of mild (19%) and severe (34%) symptoms.
Prevalence of subjective symptoms of Temporomandibular Articulation problems according to sial and demographic characteristics in the studied population. Medellin 2013 (n = 342).
| Characteristics | Males | Females | ||||||
|---|---|---|---|---|---|---|---|---|
| Prevalence | Prevalence | |||||||
| n | No symptoms | Mild symptoms | Severe symptoms | n | No symptom | Mild symptoms | Severe symptoms | |
| Age | ||||||||
| 65-74 | 91 | 57.1 | 8.8 | 34.1 | 144 | 56.9 | 17.4 | 25.7 |
| ≥ 75 | 52 | 61.5 | 9.6 | 28.8 | 55 | 47.3 | 20.0 | 32.7 |
| Education level | ||||||||
| No education | 48 | 52.1 | 12.5 | 35.4 | 65 | 53.8 | 16.9 | 29.2 |
| Primary school | 82 | 59.8 | 7.3 | 32.9 | 121 | 29.8 | 19.0 | 27.3 |
| Secondary school/university | 13 | 76.9 | 7.7 | 15.4 | 13 | 61.5 | 15.4 | 23.1 |
| Social and economic stratus | ||||||||
| Low (1-2) | 124 | 57.3 | 10.5 | 32.3 | 169 | 56.2 | 18.3 | 25.4 |
| Middle (3-4) | 19 | 68.4 | 0.0 | 31.6 | 30 | 43.3 | 16.7 | 40.0 |
| Occupation | ||||||||
| Non manual | 3 | 33.3 | 66.7 | 0.0 | 1 | 100.0 | 0.0 | 0.0 |
| Manual | 47 | 57.4 | 8.5 | 34.0 | 16 | 25.0 | 37.5 | 37.5 |
| Housework | 8 | 62.5 | 0.0 | 37.5 | 172 | 56.4 | 16.3 | 27.3 |
| Other | 85 | 60.0 | 8.2 | 31.8 | 10 | 60.0 | 20.0 | 20.0 |
| Residence area | ||||||||
| Urban | 129 | 57.4 | 8.5 | 34.1 | 177 | 56.5 | 16.4 | 27.1 |
| Rural | 14 | 71.4 | 14.3 | 14.3 | 22 | 36.4 | 31.8 | 31.8 |
| Social support | ||||||||
| Normal | 109 | 58.7 | 8.3 | 33.0 | 152 | 56.6 | 17.8 | 25.7 |
| Low | 34 | 58.8 | 11.8 | 29.4 | 47 | 46.8 | 19.1 | 34.0 |
| Total | 143 | 58.7 | 9.1 | 32.2 | 199 | 54.3 | 18.1 | 27.6 |
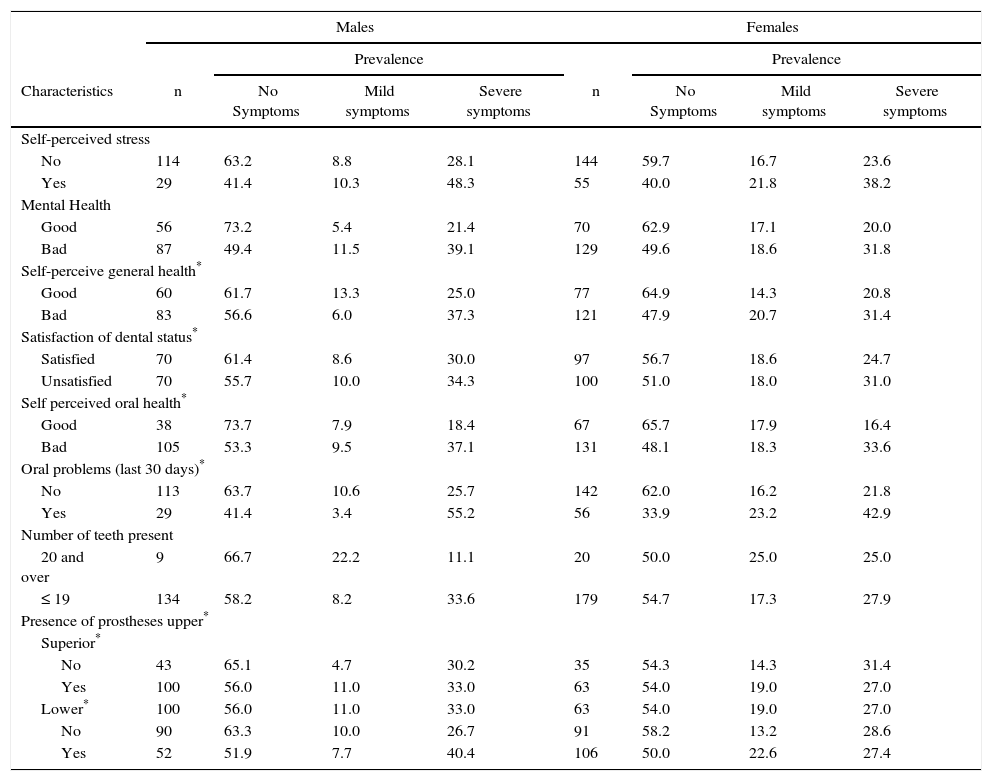
With respect to signs and symptoms prevalence according to health indicators (Table II) subjects with poorest indicators of general and oral health showed a tendency to exhibit greater prevalence of severe signs and symptoms. In this last case, greater prevalence (above 40%) was found in males who reported stress (48%), those with oral problems in the last 30 days (55%) and those wearing a lower denture (40%). With respect to females, higher prevalence was found in those reporting oral problems in the last 30 days (43%). In any case, prevalence of severe signs and symptoms were over 25% in males and females; mild signs and symptoms varied from 9.5% to 25%.
Prevalence of temporomandibular articulation problems’ subjective symptoms according to general, mental and oral health indicators in the studied population. Medellin 2013 (n = 342).
| Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|
| Prevalence | Prevalence | |||||||
| Characteristics | n | No Symptoms | Mild symptoms | Severe symptoms | n | No Symptoms | Mild symptoms | Severe symptoms |
| Self-perceived stress | ||||||||
| No | 114 | 63.2 | 8.8 | 28.1 | 144 | 59.7 | 16.7 | 23.6 |
| Yes | 29 | 41.4 | 10.3 | 48.3 | 55 | 40.0 | 21.8 | 38.2 |
| Mental Health | ||||||||
| Good | 56 | 73.2 | 5.4 | 21.4 | 70 | 62.9 | 17.1 | 20.0 |
| Bad | 87 | 49.4 | 11.5 | 39.1 | 129 | 49.6 | 18.6 | 31.8 |
| Self-perceive general health* | ||||||||
| Good | 60 | 61.7 | 13.3 | 25.0 | 77 | 64.9 | 14.3 | 20.8 |
| Bad | 83 | 56.6 | 6.0 | 37.3 | 121 | 47.9 | 20.7 | 31.4 |
| Satisfaction of dental status* | ||||||||
| Satisfied | 70 | 61.4 | 8.6 | 30.0 | 97 | 56.7 | 18.6 | 24.7 |
| Unsatisfied | 70 | 55.7 | 10.0 | 34.3 | 100 | 51.0 | 18.0 | 31.0 |
| Self perceived oral health* | ||||||||
| Good | 38 | 73.7 | 7.9 | 18.4 | 67 | 65.7 | 17.9 | 16.4 |
| Bad | 105 | 53.3 | 9.5 | 37.1 | 131 | 48.1 | 18.3 | 33.6 |
| Oral problems (last 30 days)* | ||||||||
| No | 113 | 63.7 | 10.6 | 25.7 | 142 | 62.0 | 16.2 | 21.8 |
| Yes | 29 | 41.4 | 3.4 | 55.2 | 56 | 33.9 | 23.2 | 42.9 |
| Number of teeth present | ||||||||
| 20 and over | 9 | 66.7 | 22.2 | 11.1 | 20 | 50.0 | 25.0 | 25.0 |
| ≤ 19 | 134 | 58.2 | 8.2 | 33.6 | 179 | 54.7 | 17.3 | 27.9 |
| Presence of prostheses upper* | ||||||||
| Superior* | ||||||||
| No | 43 | 65.1 | 4.7 | 30.2 | 35 | 54.3 | 14.3 | 31.4 |
| Yes | 100 | 56.0 | 11.0 | 33.0 | 63 | 54.0 | 19.0 | 27.0 |
| Lower* | 100 | 56.0 | 11.0 | 33.0 | 63 | 54.0 | 19.0 | 27.0 |
| No | 90 | 63.3 | 10.0 | 26.7 | 91 | 58.2 | 13.2 | 28.6 |
| Yes | 52 | 51.9 | 7.7 | 40.4 | 106 | 50.0 | 22.6 | 27.4 |
Lost values for the following variables: Self perceived general health n = 1 (0.3%), satisfaction of dental status: n = 5, (1.5%), self perceived oral health n = 1 (0.29%), oral problems (last 30 days): n = 4 (1.2%), presence of upper denture: n = 1 (0.29%), presence of lower denture: n = 3 (0.9%).
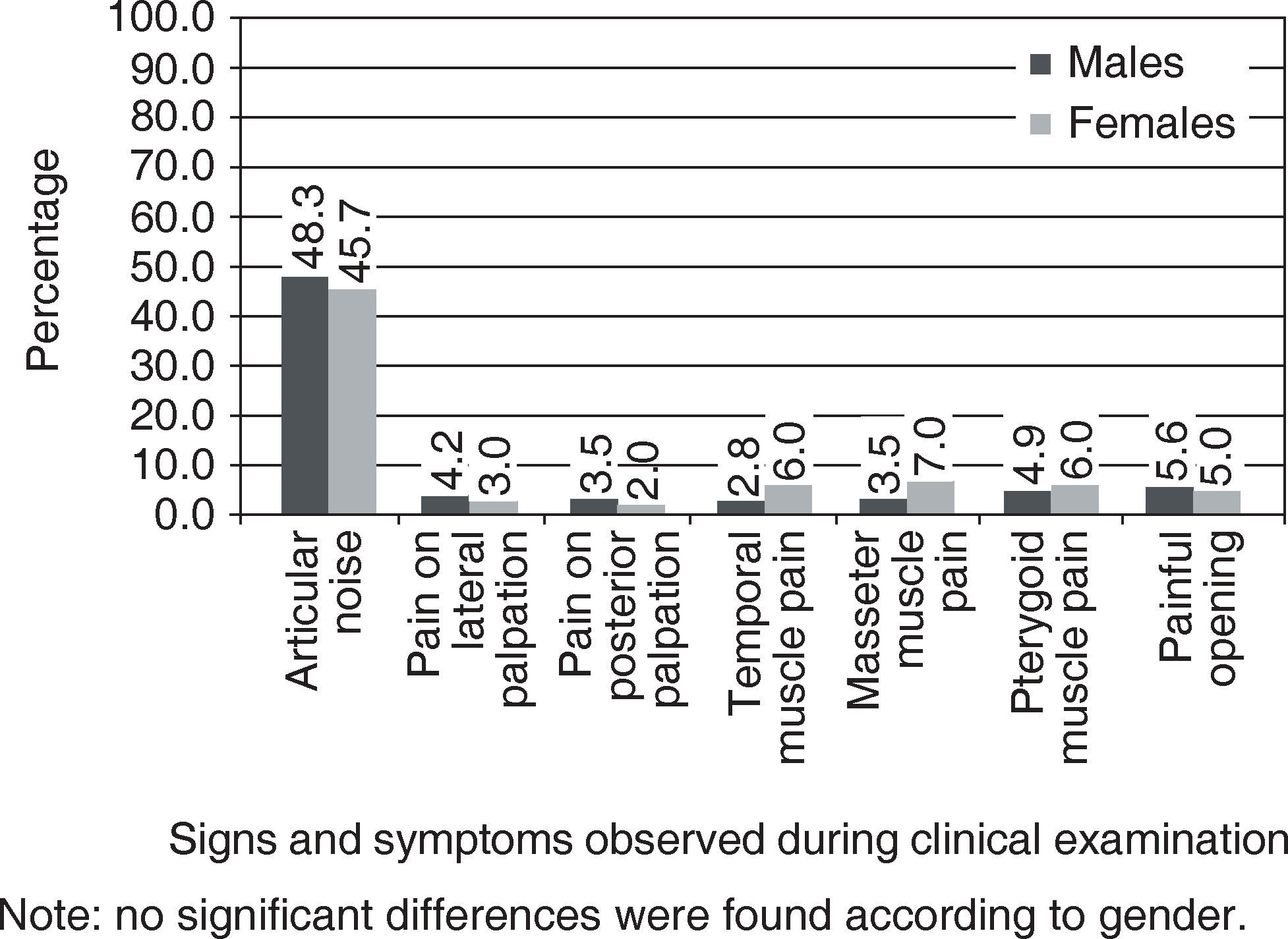
Clinical examination of signs and symptoms of ATM disorders (Figure 1) revealed that over 48% of males and 46% of females exhibited articular noises. In the rest of cases, prevalence of symptoms was under 10%. With respect to muscle pain, highest prevalence was found in the masseter muscle (7%), and in females in the pterygoid muscle (6%). No statistically significant differences were found when comparing males and females.
.")
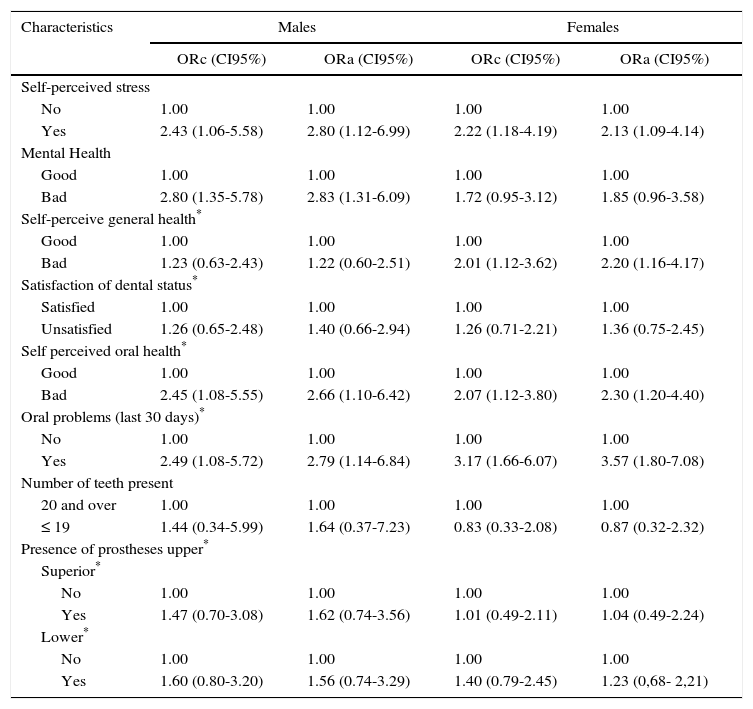
Findings with respect to associations between subjective signs and symptoms (HI) with health indicators by means of logistic regression (Table III) indicate that in both raw and adjusted models, subjects reporting general and oral health problems exhibited higher probability to report signs and symptoms of TMJ disorders. Nevertheless, no statistically significant associations were found for the case of subjects of both genders, dissatisfied with their oral health status and wearing upper or lower dentures. It is worth mentioning that females with 19 teeth or less exhibited lesser risk of reporting these signs and symptoms, even though associations were not significant. The greatest association was found in the indicator of dental problems in the prior 30 days (aOR 3.57) CI 95%, 1.80-7.08) and self-perceived poor oral health (aOR 2.30; CI 95%) 1.20-4.40) in the case of females, and for males it was found within the poor mental health indicator (H: aOR 283; CI 95% 1.31- 6.09) as well as self-perceived stress (H: aOR 2.80; CI 95% 1.12-6.99).
Association between presence of subjective signs and symptoms and through clinical examination and gender in the studied population. Medellin 2013 (n = 342).*
| Characteristics | Males | Females | ||
|---|---|---|---|---|
| ORc (CI95%) | ORa (CI95%) | ORc (CI95%) | ORa (CI95%) | |
| Self-perceived stress | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 2.43 (1.06-5.58) | 2.80 (1.12-6.99) | 2.22 (1.18-4.19) | 2.13 (1.09-4.14) |
| Mental Health | ||||
| Good | 1.00 | 1.00 | 1.00 | 1.00 |
| Bad | 2.80 (1.35-5.78) | 2.83 (1.31-6.09) | 1.72 (0.95-3.12) | 1.85 (0.96-3.58) |
| Self-perceive general health* | ||||
| Good | 1.00 | 1.00 | 1.00 | 1.00 |
| Bad | 1.23 (0.63-2.43) | 1.22 (0.60-2.51) | 2.01 (1.12-3.62) | 2.20 (1.16-4.17) |
| Satisfaction of dental status* | ||||
| Satisfied | 1.00 | 1.00 | 1.00 | 1.00 |
| Unsatisfied | 1.26 (0.65-2.48) | 1.40 (0.66-2.94) | 1.26 (0.71-2.21) | 1.36 (0.75-2.45) |
| Self perceived oral health* | ||||
| Good | 1.00 | 1.00 | 1.00 | 1.00 |
| Bad | 2.45 (1.08-5.55) | 2.66 (1.10-6.42) | 2.07 (1.12-3.80) | 2.30 (1.20-4.40) |
| Oral problems (last 30 days)* | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 2.49 (1.08-5.72) | 2.79 (1.14-6.84) | 3.17 (1.66-6.07) | 3.57 (1.80-7.08) |
| Number of teeth present | ||||
| 20 and over | 1.00 | 1.00 | 1.00 | 1.00 |
| ≤ 19 | 1.44 (0.34-5.99) | 1.64 (0.37-7.23) | 0.83 (0.33-2.08) | 0.87 (0.32-2.32) |
| Presence of prostheses upper* | ||||
| Superior* | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.47 (0.70-3.08) | 1.62 (0.74-3.56) | 1.01 (0.49-2.11) | 1.04 (0.49-2.24) |
| Lower* | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.60 (0.80-3.20) | 1.56 (0.74-3.29) | 1.40 (0.79-2.45) | 1.23 (0,68- 2,21) |
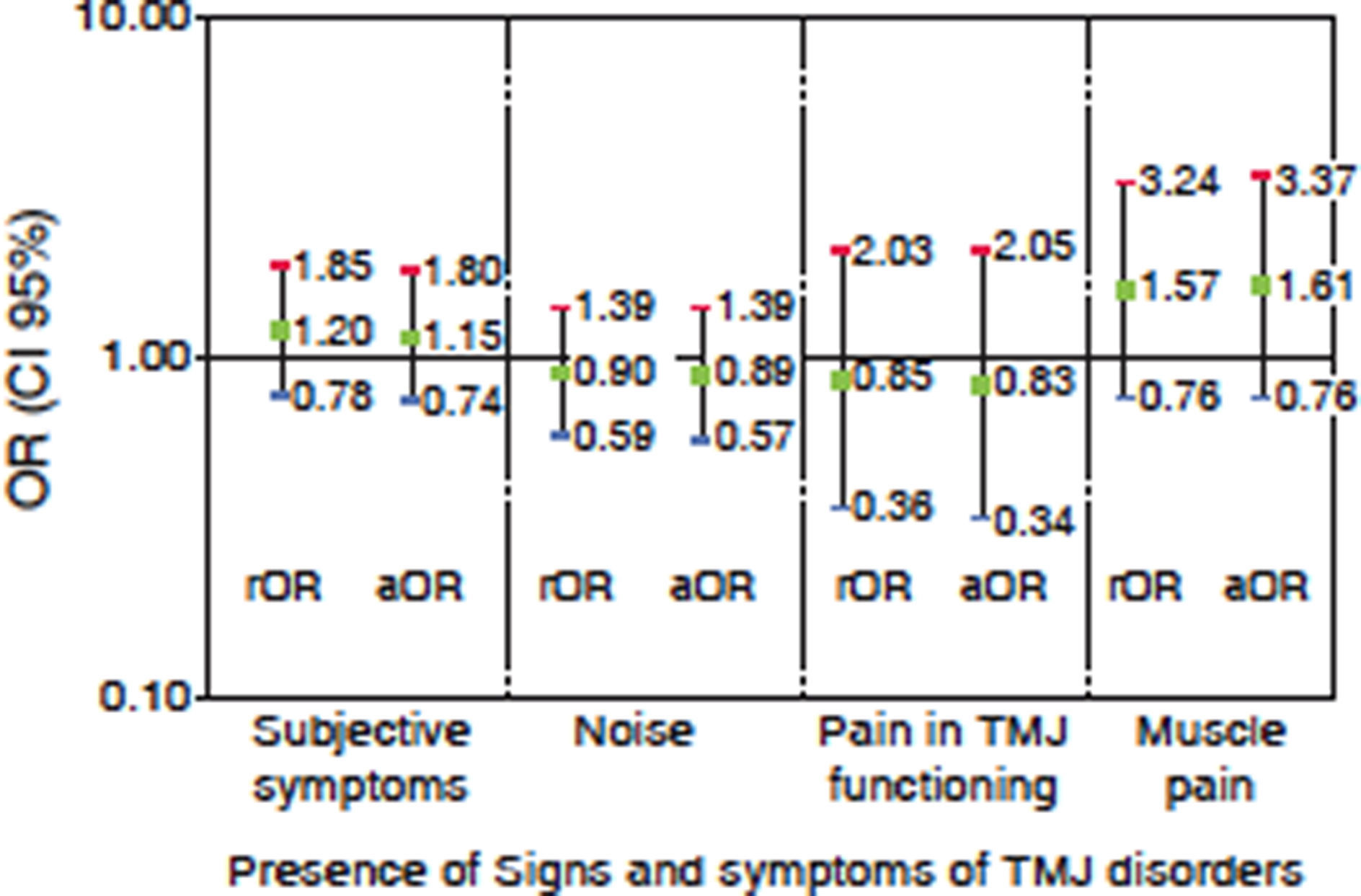
Finally, bearing in mind association between gender and presence of subjective signs and symptoms (HI) as well as clinical examination (figure 2) it was observed that although females exhibited greater risks of reporting TMJ related problems (except articular noises which were higher in males) no statistically significant associations were found. It is worth mentioning that the higher association was found in the case of presence of muscle pain (aOR 1.61 CI 95% 076-3.37).
DISCUSSION.")
Main findings of the present study provide an account of social and demographic factors related to prevalence of signs and symptoms of TMJ disorders. Age, educational level, occupation, social and economic status or residence area are all factor taking part in the process; important differences have been found according to age. Subjects with low social support reported higher presence of severe symptoms. An association was found between presence of subjective signs and symptoms with health indicators, even with very few exceptions after adjusting for confusion variables. Females exhibited a tendency of reporting more severe TMJ problems, although no statistically significant association was found in raw and adjusted models.
High prevalence of TMJ disorders in elderly patients assessed in the present study concurs with findings of other studies which have used similar methodologies and comparable indicators. With respect to those reported by means of anamnesic index, literature reports that their prevalence decreases with age. In the present study this premise was confirmed; it was additionally found that in elderly subjects there was greater frequency of severe symptoms involving self-perceived functional limitations. This concurs with results of the last Estudio Nacional de Salud Bucal ENSAB III (National Study of Oral Health ENSAB III) as well as other international studies.8–10,19 This phenomenon can be explained based on the adaptive ability of biological systems; moreover, elderly subjects tend to only report health conditions considered more severe by psychosocial factors involved with pain perception and modulation.
Many local and worldwide studies show similar results with respect to gender-related severity of signs and symptoms of temporomandibular disorders, these studies have revealed no significant differences according to gender, showing higher prevalence and severity values in females.2,3,9 Nevertheless, other studies have reported differences which are not significant according to gender.24 These differences can be explained in relation with pain mechanisms and the stomatognatic system as well as factors related to the support and social role of women, among other factors, psycho-social circumstances and hormonal fluctuations.
There is scarce literature dealing with clinical signs, since studies conducted in elderly population are normally restricted to the anamnesic component of subjective evaluation.25 Articular noise was the most frequently found clinical sign, this concurs with other studies conducted in population of same age range.25,26 When analyzing articular and muscular pain in the present article, no associations were found among these clinical signs and social and demographical circumstances. This is contrary to reports of other studies, which indicated that oral and facial pain situations were more common in populations of lower socio-economic and educational level. This situation can be explained by the greater level of psychological distress, more unfavorable oral health status and higher probability of maladaptive response to this disease exhibited by this population group.27,28
Stress has been identified as a triggering factor for temporomandibular disorders. Results revealed by the present study show how elderly patients with self-perceived stress exhibited higher prevalence of temporomandibular disorders, this phenomenon was present in both genders. Likewise, results give evidence of stress being a risk factor for TMD development. These results concur with other studies performed in elderly as well as young population; it can be justified when considering stress’ biological responses, which in some cases might represent a problem since they can manifest as physical exhaustion, headaches, circulatory and gastric alterations, psycho-pathological disorders and oral disease.29–31
Social support of subjects is related to state of health, as proposed in the present study where it was found that elderly subjects with scarce social support exhibited higher prevalence of mild and severe symptoms related to tremporomandibular disorders. This phenomenon can be explained by the effect of social relations’ quality and quantity, since they can exert an effect on biological mechanisms of health-disease processes, through mediation of processes such as stimuli for seeking medical attention, exercise, nutrition, discouraging tobacco use and, in general terms, seeking healthy lifestyles.32
With respect of self-perceived general health, and more specifically oral health, results agree with other studies conducted on elderly population indicating that this factor is related to symptoms perceived with TMD, and explained from the point of view of the relationship of physical and mental repercussions represented by temporomandibular disturbances in terms of loss of functional ability, in addition to the impact exerted by pain on the phychosocial level of people's lives.22,33
It is important to point out both the strengths and weaknesses of the present paper. As far as our knowledge goes, in our country, it can be considered one of the first studies dealing with research, since most studies are centered on caries and periodontal disease. An adequately sized sample of elderly subjects was obtained from Hospital Units and Health Centers of the Public Health Network in Medellin. This enabled us to visualize the status of public health in an important, especially vulnerable segment of society. Likewise, use of validated instruments (self-perception-clinical) allowed establishment of international comparisons. Questionnaire quality control was performed, thus favoring their reliability. Finally, incorporation of health variables allows new perspectives for epidemiological analyses.
With respect to limitations in the present study, it is important to clarify that used indicator (Helkimo Index) for TMJ assessment was conducted depending on signs and symptoms as a sieve test, and did not profess to emit diagnoses of specific diseases. This index is founded on a classification of anamnesic circumstances severity degrees, or subjective symptoms, clinical signs of temporomandibular articulation disorders and associated structures.34 In order to conduct this research in Medellin, an index was selected which, in spite of its recognized limitations, would allow comparative analyses with other studies conducted on elderly population, and also in Colombia. This was based on the fact that the Third Study of Oral Health (1998) (Estudio Nacional de Salud Bucal) used this indicator at a population level.
It is important to mention there are several systems and indexes to determine prevalence of temporomandibular disorders in epidemiological research. Among these we mention the Craniomandibular Index proposed by Friction and Schiffman in 1985,16 DC/TMD index introduced by Dworkin and LeResche in 199217 which is internationally accepted, as well as the clinical orientation analysis proposed by Jeffrey Okesson in 1996.18 DC/TMD index is one of the most widely used by researchers. since it is part of an international consortium, and additionally offers methodological tools and includes bio-psycho-social axes to analyze and achieve diagnostic approach of these disorders.35 Future research projects must use more recent epidemiologic criteria achieved by means of theoretical and clinical gauging in order to identify signs and symptoms of temporomandibular disorders in Colombian elderly population
In any case, irrespectively of the index used, it is necessary to supplement information with other clinical examinations and factor assessment; to thus build up gathered information and render it more reliable, by means of controlling variables and establishing associations, risk factors as well as protectors. Use of these longitudinal studies would contribute to identification of causing factors. It would be suitable to further the present study to include other elderly patients which might be institutionalized in the city as well as those linked to other social strata, so as to identify inequality situations and complement with other social and nutritional variables which might influence in the presence of signs and symptoms of temporomandibular disorders. It is important to establish specific treatment and interventions to alleviate disorders and conduct experimental studies in order to assess efficiency and effectiveness of these therapeutic interventions.
To conclude, it can be said that epidemiologic vigilance systems of oral health indicators need to be reinforced including other conditions, incorporating a perspective of the human vital cycle and encompassing variables to trace inequality situations
Accomplishment of strategies based on the realities of different communities seems to be an effective way to allow improvement of oral health situation in especially vulnerable populations.
This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam