



Evaluation of the changes to the initial simulated root canal anatomy when comparing the preparation made by three different rotary systems: ProTaper Universal, ProTaper Next and ProTaper Gold.
MethodsThe quantitative analysis was made by measuring the canal width of 36 S-shaped canals, distributed by three groups of twelve samples each (Group A – ProTaper Universal, Group B – ProTaper Next, Group C – ProTaper Gold). To measure canal width, pre and post instrumentation images were superimposed and studied using Rhinoceros Software. The statistical analysis was obtained using Kolmogorov–Smirnov test, Mann–Whitney post hoc multiple comparisons U test and One-Way ANOVA, with a significance of p<0.05.
ResultsConsidering the inner side of both apical and coronal curvatures, differences between files were statistically significant (p<0.05). ProTaper Universal system was responsible for a bigger widening, while ProTaper Gold presented the smaller mean value.
ConclusionsProTaper Gold was the rotary system that most respected the initial S-shaped canal anatomy. ProTaper Universal was the system that originated the greatest modification of the initial canal, presenting a significant tendency to straighten the apical curvature.
Avaliar as alterações da anatomia inicial do canal radicular simulado, após a preparação com diferentes sistemas rotativos: ProTaper Universal, ProTaper Next e ProTaper Gold.
MétodosA análise quantitativa foi feita através da medição da largura de 36 canais em forma de S, distribuídos em três grupos de doze espécimes (Grupo A - ProTaper Universal, Grupo B - ProTaper Next, Grupo C - ProTaper Gold). Para a realização das medições as imagens pré e pós instrumentação foram sobrepostas e estudadas no software Rhinoceros. A análise estatística foi obtida com o teste Kolmogorov–Smirnov, Mann–Whitney post hoc U test de comparações múltiplas e One-Way ANOVA, considerando os valores estatisticamente significantes com p<0,05.
ResultadosConsiderando a porção interna da curvatura coronal e apical, as diferenças entre as preparações efetuadas foram estatisticamente significantes (p<0,05). O sistema ProTaper Universal foi responsável por um maior alargamento do canal e a ProTaper Gold por apresentar os valores mais baixos.
ConclusõesProTaper Gold foi o sistema rotativo que melhor respeitou a anatomia inicial dos canais simulados. Por sua vez, o sistema ProTaper Universal originou a maior modificação do canal inicial, apresentando uma tendência significativa para a retificação da curvatura apical.
When performing an endodontic treatment, it is crucial that the final root canal preparation presents a shape and direction similar to the initial canal anatomy. This is important in order to accomplish a correct irrigation, removing all debris and microorganisms. At the same time, it is also important to avoid excessive dentinal removal, which can compromise the success of the treatment.1–4 However, it is known that the maintenance of the initial canal shape and direction becomes a challenge as root canal curvature increases, especially in the apical regions.1,2,5
To overcome the difficulties in root canal preparation, simplify the procedures and reduce its preparation time, several rotary systems have been developed and improved in the last few years, with the development of new rotary file designs, techniques and manufacturing methods.4,6–8
Nickel–titanium (NiTi) instruments, characterized by their super-elastic behavior, shape-memory property and lower modulus of elasticity compared to stainless steel files, prove to be more efficient and conservative in shaping narrow and curved root canals than stainless steel instruments.7,9–13 Many studies have been made to evaluate this shaping ability, confirming its efficacy.13,14 However, the type of alloy was not the only responsible for better instruments that improved canal preparation. Many factors independently and in combination, influence instrument properties and their shaping ability. Different thermomechanical processing and file designs have been applied to optimize the microstructure and transformation behavior of NiTi alloys, improving their flexibility and fracture resistance.8,15,16
ProTaper Universal (PTU), made of conventional NiTi wire, has been widely used and studied. This system is characterized by a variable taper through the file's length, passive tips and a convex triangular cross-section.10,15,16 Recently, a new NiTi wire was developed through a patented thermomechanical process, called M-Wire. ProTaper Next (PTN) files, made out of this M-Wire alloy, have also a variable taper design and an off-centered axis with a rectangular cross-section, presenting improved cyclic fatigue resistance in comparison with those made of conventional super elastic NiTi alloys.3,8,15 A more recent and advanced metallurgy process allowed the manufacturer to introduce ProTaper Gold (PTG) rotary files. This system features identical geometric characteristics as PTU but presents more flexibility and more fatigue resistance, as it is claimed by the manufacturer.15,16 However, PTG properties have not been widely studied, as this system was introduced in the market in the end of 2014.16
To compare each system shaping ability it is important to evaluate their capacity to avoid central axis transportation and curvature straightening of curved root canals.10 According to the scientific evidence, highly flexible files originate more centered preparations, reducing iatrogenic errors resulting from canal transportation, such as zippings, ledgings or perforations and reducing the tendency to straightening, resulting in an increased efficiency and safety of root canal treatment.2,11,15
Therefore, the aim of this study was to compare the three rotary systems ability to maintain a shape similar to the initial simulated S-shaped canals anatomy, regarding the straightening and canal transportation.
Materials and methodsA total of 36 clear resin blocks with an S-shaped curvature canal (ISO 15, Endo-Training-Bloc-S .02 Taper; Dentsply Maillefer, Ballaigues, Switzerland, Lot 3461830) were used. Attending to the manufacturer's recommended technique, each group of twelve resin blocs was prepared by one of the three different rotary files system, using inside each group two sterilized PTU kits Sx-F3, 25mm (Dentsply Maillefer, Ballaigues, Switzerland, Lot 1182375, Val 2019-10), two sterilized PTN kits X1–X3, 25mm (Dentsply Maillefer, Ballaigues, Switzerland, Lot 1211969, Val 2020-02) and two non-sterilized PTG kits Sx-F3, 25mm (Dentsply Tulsa Dental Specialties, Johnson City, TN, Lot 0000069807).
Each simulated canal was prepared to a working length of 16millimeters, at a speed of 300rpm and a torque-control level of 40, 2Ncm, as the suggested settings by the manufacturer, using a 1:16 reduction hand-piece powered by an electric motor (ATR Tecnika, Dentsply Maillefer).
All canals were prepared by the same operator, a final year dental student who had little experience using rotary files. Only 6 resin blocks were prepared at a time to minimize operator fatigue. The final apical preparation was set in a 0.25mm diameter, corresponding in Group A to a PTU F2, in Group B to a PTN X2 and in Group C to a PTG F2, after all canals were scouted up to the working length with a #10 stainless-steel k-file (Dentsply Maillefer,) and a ProGlider (25mm, Dentsply-Maillefer, Ballaigues, Switzerland, Lot 1167749, Val 2019-09). Irrigation was performed with water after the use of each file.
Pre instrumentation and post instrumentation images were recorded using a DSLR (Digital Single-lens Reflex) camera (Olympus Digital Camera E500) with a 35 macro lens, using a shutter speed of 1.6s and a 22 F-stop.
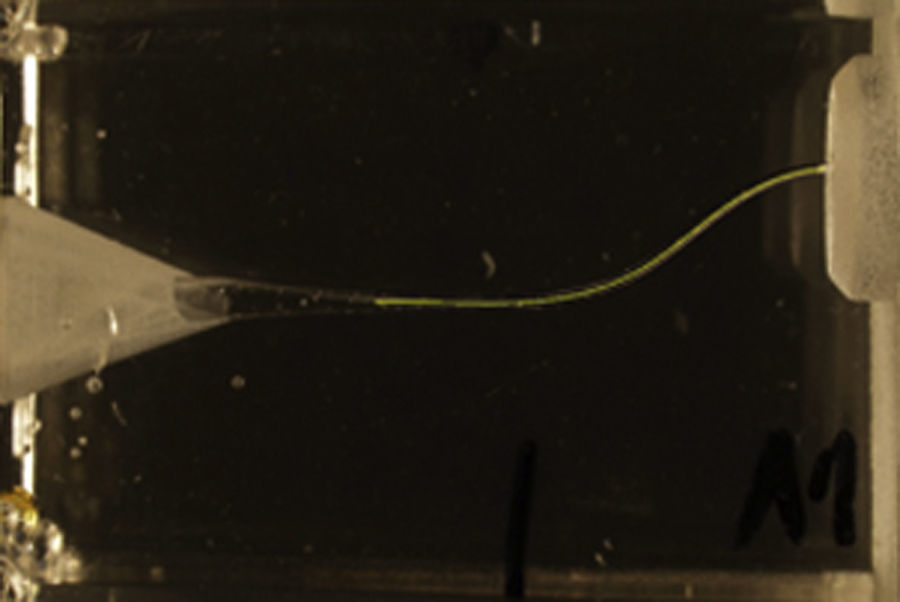
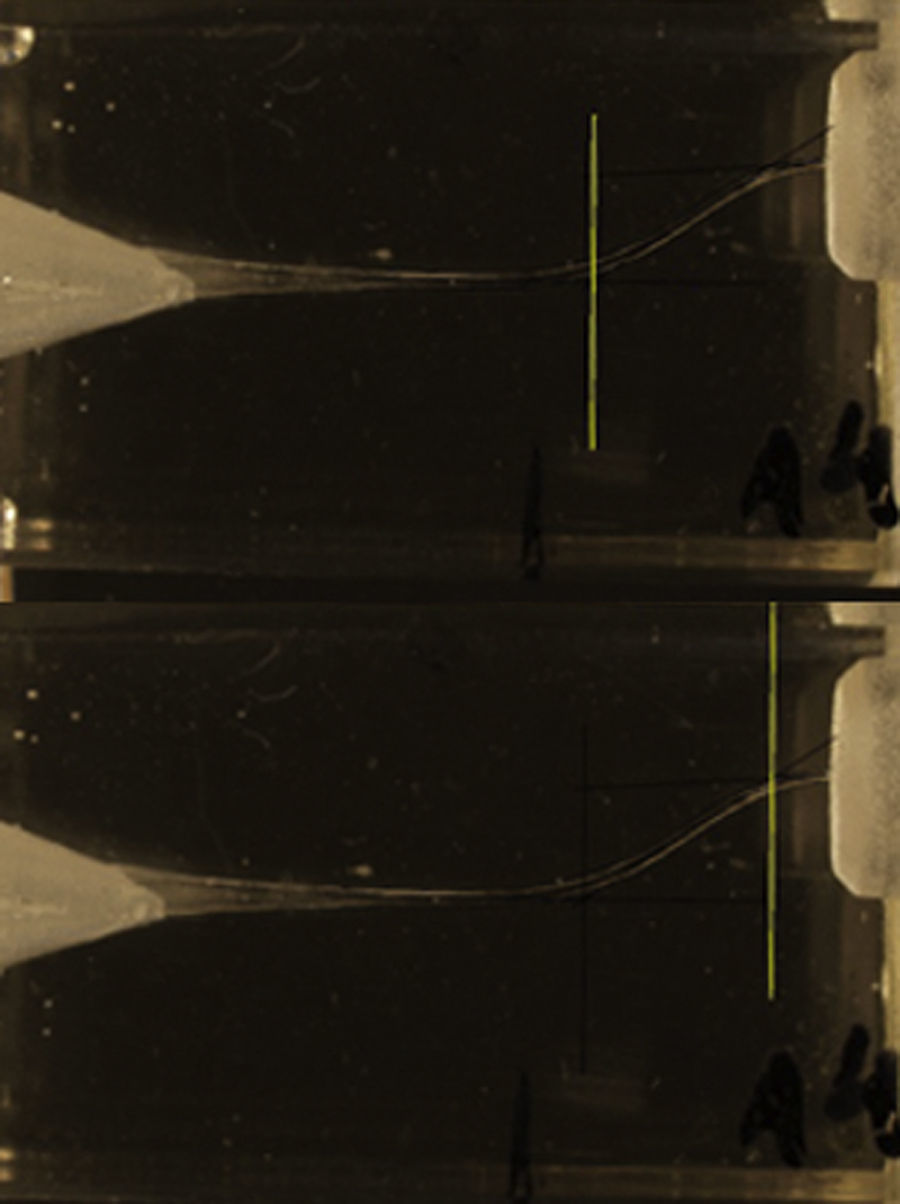
Rhinoceros Software (version 5.0; Robert McNell & Associates, Seattle, WA) was used to identify the mean axis of the canal from the pre instrumentation images and to identify the two margins of the prepared canal, in the post instrumentation images. It was also used to identify the two measure points in the coronal and apical curvatures, as defined in Figs. 1 and 2, respectively. These measure points resulted from the interception of two tangent lines of each curve.


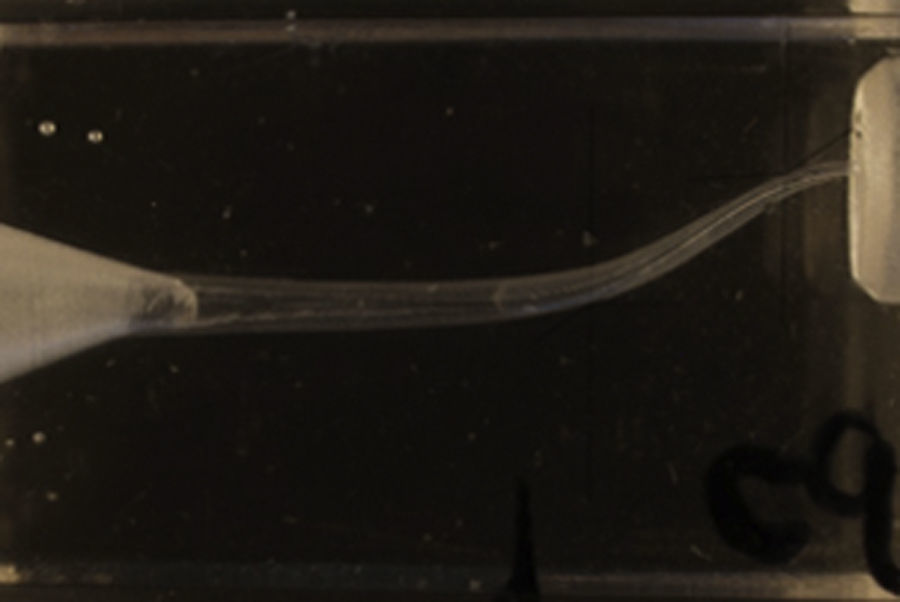
The post instrumentation digital images were finally superimposed over the pre instrumentation images using a digital imaging software (Adobe Photoshop, version CS6; Adobe Systems Inc., San Jose, CA), as presented in Fig. 3.
.")
Before superimposed images return to the Rhinoceros Software, four variables were established: the distance, in a real scale, from the center of the canal to the inner and outer margins of the prepared curve canal, in both apical and coronal curvatures. These paired images and the canal width measures obtained, gave us a quantitative evaluation of the incidence of canal transportation after mechanical preparation.
The statistical analysis was obtained using the IBM ® SPSS ® Statistics version 22.0.0 software. Descriptive statistical analysis was performed in each group (A, B and C). The Kolmogorov–Smirnov test was used to evaluate the data normality, followed by One-Way ANOVA, a parametric test, for data with a normal distribution and the Mann–Whitney post hoc multiple comparisons U test, a non-parametrical test for data with no normal distribution. Differences were considered statistically significant when p<0.05.
ResultsDescriptive statistics of the four variables was done. The mean width and standard deviation for each experimental group are displayed in Table 1.
Descriptive analysis of the canal width in the measure points of the coronal and apical curvatures.
| Coronal curvature | Apical curvature | |||
|---|---|---|---|---|
| Inner (mm) | Outer (mm) | Inner (mm) | Outer (mm) | |
| A – ProTaper Universal | 0.37±0.04 | 0.10±0.04 | 0.31±0.05 | 0.02±0.03 |
| B – ProTaper Next | 0.32±0.02 | 0.09±0.03 | 0.22±0.04 | 0.0 5±0.03 |
| C – ProTaper Gold | 0.29±0.02 | 0.11±0.02 | 0.17±0.02 | 0.05±0.02 |
Differences between the three files systems canal preparations on the outer side of the coronal curvature were not statistically significant, however, in its inner side, these differences were statistically significant (p<0.05), where the PTU system was responsible for a bigger widening, while PTG presented the smaller mean value.
Concerning the inner side of the apical curvature, the differences between the three files systems canal preparations was statistically significant (p<0.05), where PTU was, once more, responsible for a bigger widening, while PTG presented the smaller mean value. In the outer side of the apical curvature, differences in the canal preparation between PTU and the other two files systems were statistically significant (p<0.05), however, differences between PTN and PTG were not statistically significant.
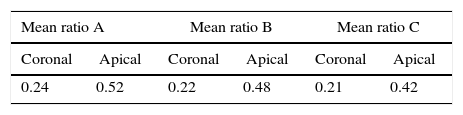
The PTU system caused significantly greater widening than the other two groups, especially at the inner sides of both curved regions, tending toward the straightening of the canal. The PTG showed the lowest widening on both regions. The amount of resin wall removal was always superior in the inner side of both curvatures. Additionally, inside each group, by directly comparing coronal and apical ratio, the apical curvature was the one that lost more material, as it is shown in Table 2.
DiscussionEvaluating modifications in canal initial anatomy after instrumentation has been widely used to understand how the file's mechanical properties or technique used can influence their shaping ability.6 Furthermore, clinicians during clinical practice should be aware of the mechanical properties of the chosen instruments to best adapt a rotary file system to anatomic challenges.
The present study compared the ability of PTU, PTN and PTG to maintain a similar anatomy to the initial one on S-shaped canals. Despite the fact that these resin blocs may not always reflect the file's action in real teeth, they contribute to standardize experimental conditions and have been reported to reliably demonstrate differences in files system performance, probably as a result of their anatomic challenge.1,6,11
The study consisted of a comparison between resin blocks canal shape prior and after mechanical instrumentation.
PTG produced significantly less modification in coronal and apical canal curvature compared to PTU. When comparing PTN and PTU, the results of the first system showed less modification in coronal and apical canal curvature compared to the second one, being these results consistent with Shori et al.3 conclusions, which states that PTN can induce less dentinal defects than PTU. Wu et al.10 concluded that PTN is responsible for a better maintenance of the initial anatomy of coronal curvature compared to PTU, however, when it comes to the apical curvature, both had the tendency to straightening.
It might be assumed that PTG is the rotary system that best respects the initial S-shaped canal anatomy and was responsible for the most centered preparations. Higher flexibility might be the predominant property responsible by the PTG system's ability to maintain a similar S-shaped canal's initial anatomy. Therefore, PTG showed more flexibility than PTN and PTU, coinciding with previous studies.15,16 The identical architecture and operation of PTG and PTU systems, indicates that their different manufacturing process clearly affect their flexibility.16
PTU was responsible for a bigger widening, introducing more modifications on these double curvature canals, presenting less flexibility than PTN and PTG. Using PTU sequentially after other less tapered, more flexible systems can help the clinician to reduce canal transportation.11,17
No macroscopic deformations or fractures of any instrument, mechanical or manual, occurred during the experiment.
Based on the results and regarding the characteristics of each file, the clinician should be able to select the system that best adapt to canal conditions. PTG may be more suited to complicated anatomies with abrupt curvatures.
ConclusionsUnder the limitations of this study, PTG was the rotary system which best respected the initial anatomy of the S-shaped canals, presenting a more centered preparation in both coronal and apical curvatures. PTU was the system that originated the greatest modification of the initial canal, presenting a significant tendency to straighten apical curvature.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.