




Monitoring and preventing suicidal behaviour requires, among other data, knowing suicide deaths precisely. They often appear under-reported or misclassified in the official mortality statistics. The aim of this study is to analyse the under-reporting found in the suicide mortality statistics of Tarragona (a province of Catalonia, Spain).
Method and materialsThe analysis takes into account all suicide deaths that occurred in the Tarragona Area of the Catalan Institute of Legal Medicine and Forensic Sciences (TA-CILMFS) between 2004 and 2012. The sources of information were the death data files of the Catalan Mortality Register, as well as the Autopsies Files of the TA-CILMFS. Suicide rates and socio-demographic profiles were statistically compared between the suicide initially reported and the final one.
ResultsThe mean percentage of non-reported cases in the period was 16.2%, with a minimum percentage of 2.2% in 2005 and a maximum of 26.8% in 2009. The crude mortality rate by suicide rose from 6.6 to 7.9 per 100,000 inhabitants once forensic data were incorporated. Small differences were detected between the socio-demographic profile of the suicide initially reported and the final one. Supplementary information was obtained on the suicide method, which revealed a significant increase in poisoning and suicides involving trains.
ConclusionsAn exhaustive review of suicide deaths data from forensic sources has led to an improvement in the under-reported statistical information. It also improves the knowledge of the method of suicide and personal characteristics.
La vigilancia y prevención de la conducta suicida requiere, entre otros datos, conocer con precisión las muertes por suicidio (MPS). Frecuentemente existe una infradeclaración o mala clasificación de las MPS en las estadísticas oficiales de mortalidad. El objetivo del estudio es analizar la infradeclaración de la estadística de mortalidad por suicidio en Tarragona (Cataluña, España).
Material y métodosAnálisis de las MPS ocurridas en la División de Tarragona del Institut de Medicina Legal i Ciències Forenses de Catalunya (DT-IMLCFC) entre los años 2004 y 2012. Las fuentes de información fueron el fichero de defunciones del Registre de Mortalitat de Catalunya (RMC) y el archivo de autopsias del DT-IMLCFC. Se compararon estadísticamente las tasas y las características demográficas de las MPS declaradas en el RMC y las recuperadas.
ResultadosLa media de casos no declarados en el período fue del 16,2%, con el mínimo en el año 2005 (2,2%) y el máximo en el año 2009 (26,8%). La tasa bruta de mortalidad por suicidio pasó de 6,6 por 100.000 habitantes a 7,9 por 100.000 habitantes tras la incorporación de los datos forenses. Se detectaron diferencias poco importantes en el perfil sociodemográfico de los suicidios declarados inicialmente y los definitivos, excepto en el método de suicidio, con un aumento significativo de los envenenamientos y los arrollamientos en vía férrea.
ConclusionesLa recuperación de datos en las MPS a partir de las fuentes forenses mejora la información estadística, corrigiendo su infradeclaración y ampliando el conocimiento sobre el método de suicidio y las características personales.
Suicide is one of the main public health problems at a worldwide level. According to the World Health Organisation, it causes approximately 800,000 deaths per year (11.4 cases per 100,000 individuals in the year 2012), and rates vary greatly geographically and over time, even in a single country.1 Although the pattern of mortality due to suicide varies according to age, sex and temporal and geographical distribution,2 Spain has one of the lowest rates in the European Union.3 In the five years from 2007 to 2011 the annual average stood at 3265 deaths due to suicide (DDS), while since 2008 DDS have surpassed deaths due to traffic accidents, with age-adjusted rates of 9.6 per 100,000 men and 2.7 per 100,000 women.4 Additionally, in this period suicide was the first cause of mortality in men aged from 35 to 44 years old and in women aged from 25 to 44 years old.
Several studies indicate that DDS are underreported or poorly classified.1,5 This affects mortality statistics due to this cause and may have repercussions on the development of preventive policies, research financing and the evaluation of prevention programmes.6 In Spain, as is the case with other deaths due to external causes, several studies have shown that suicide mortality statistics are not very reliable,7–9 and it is said that forensic data should be used to improve them. Forensic information is used as a source of data to complement statistical data due to the fact that it supplies basic data on the cause and circumstances of death. This data is from the legal autopsies performed by forensic doctors in Legal Medicine Institutions.10 These autopsies are obligatory in Spain in all cases of death due to violent or unknown causes. They discover the mechanism that causes death and its intentionality, which is fundamental to detect suicide. Autopsy is only not performed in a very small percentage of cases of death when legal intervention takes place, in cases when death is well-documented as natural.
The aim of this study was to analyse the underreporting of mortality statistics due to suicide in the geographical area of the Tarragona Division of the Institut de Medicina Legal i Ciències Forenses de Catalunya (DT-IMLCFC). This covers an area with more than half a million inhabitants, and forensic sources of information were compared with the Registre de Mortalitat de Catalunya (RMC). It is possible to compare both sources thanks to an agreement 2012 between the departments of Salut and Justícia of the Generalitat de Catalunya. This allows the RMC to access data on deaths subjected to a legal autopsy in the IMLCFC to improve statistical quality.
MaterialAll of the cases of DDS which occurred from 2004 to 2012 in the DT-IMLCFC were analysed. This institution covers 5 judicial areas (El Vendrell, Falset, Reus, Tarragona and Valls) corresponding to the comarcas of Alt Camp, Baix Camp, Baix Penedès, Conca de Barberà, Priorat and Tarragonès, as well as 8 municipalities in the Ribera d’Ebre comarca. This territory as a whole covers a large part of Tarragona province.
Data are from the autopsy archive files of the DT-IMLCFC and the deaths file of mortality statistics. The autopsy file includes general information (age, sex and date of death as well as data corresponding to identification and legal proceedings), the cause of death and the medical-legal cause of the same established by the forensic doctor after combining information on the circumstances of the case and the autopsy result.
The deaths file of the mortality statistics lists all of the deaths in Catalonia of residents and non-residents. Those involving a judicial intervention include a specific document consisting of the statistical bulletin of death with judicial intervention. This is completed in the court or registry office based on the data of the forensic report, and it is sent to the statistical administration.
All of the DDS identified in both sources were included, verifying sociodemographic data as well as the cause of death. Cause of death was coded according to the tenth revision of the International Classification of Diseases (ICD-10). The standard cause of death was the one shown in the autopsy file of the DT-IMLCFC, while for demographic data the causes shown in the RMC were used. The cases which initially only appeared in one of the 2 sources were mainly deaths shown with another cause in their respective files.
The population for calculation of the rates was obtained from the Statistics Institute of Catalonia (IDESCAT), the post-census estimation at 1 July for the populations of the comarcas and the municipal registry of inhabitants for the populations of the 8 municipalities analysed.
MethodsFor each year calculation of the percentage of underreporting used the total number of DDS declared to the RMC over the total number of deaths due to suicide detected after recovering the forensic information. To estimate the impact of underreporting on suicide mortality statistics, the rates of mortality were calculated for the different years before and after the recovery of autopsy data. For “beforehand”, the numerator contained the DDS declared in the RMC, while to calculate “afterwards”, the total number of identified suicides was included. Both cases refer to individuals resident in the area.
Both rates were compared by using the following formula:
where:
tRMC=mortality rate due to suicide “beforehand” (RMC).
tRMC+DT= mortality rate due to suicide “afterwards” (RMC).
P=population of residents in the area.
If the value of μ is greater than ±1.96, both rates are statistically different with a confidence level of 95%.
The demographic characteristics of the DDS shown in the RMC were compared with those that were recovered (the DDS not detected in one of the 2 sources) using the chi-squared test (χ2).
Results483 DDS were identified in the forensic autopsies of the DT-IMLCFC, one of which was not shown in the RMC. In 394 cases both sources agreed that suicide was the cause of death, while 88 suicides confirmed by autopsy figured in the RMC with other causes of death. Moreover, in 14 other cases shown as suicides in the RMC, 10 had a different cause of death in the autopsy file and 4 did not figure in the said registry. To summarise, before data recovery the RMC contained 408 cases of suicide that, after different checks using the forensic source, amounted to 487 (with 4 cases of suicide shown in the RMC that were not located in the forensic source).
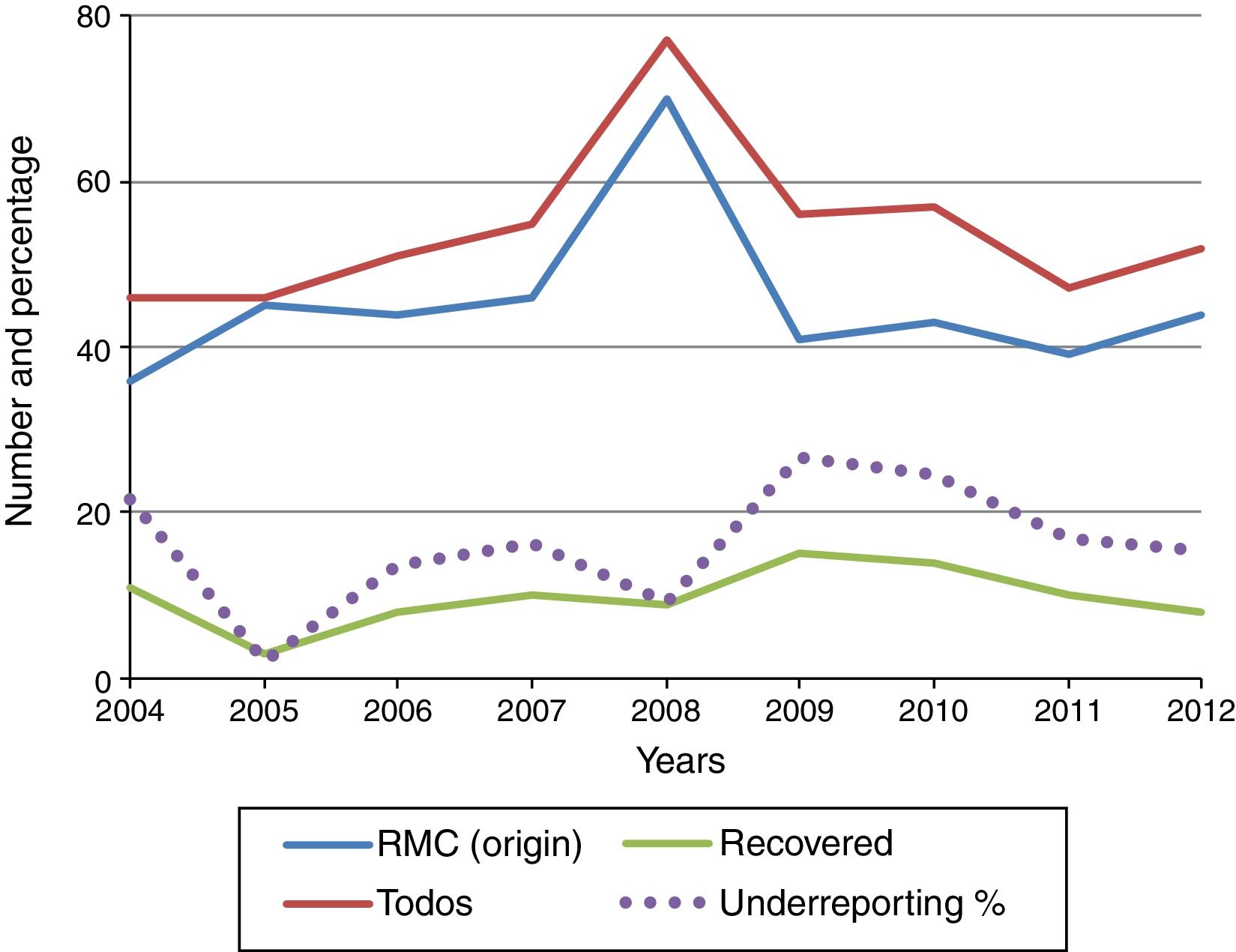
Fig. 1 shows the evolution of recovered and total declared cases of suicide, as well as the percentage of underreporting per year. The average proportion of unreported cases in this period stands at 16.2%, while the smallest number occurred in the year 2005 (2.2%) and the largest in 2009 (26.8%).

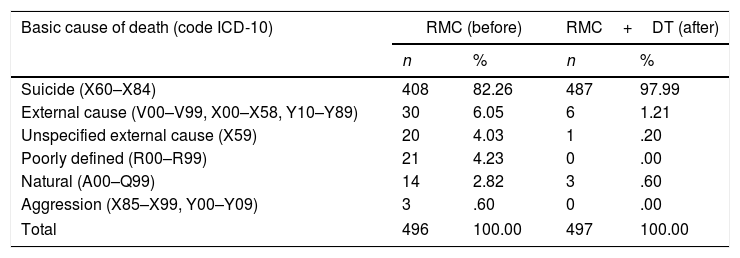
Table 1 shows the detected causes and the causes of death before and after information recovery and verification. More than half of the 88 cases of suicide unreported to the RMC as such were included in the group of external causes. On the other hand, of the 10 cases initially reported as suicides, 7 were classified as due to other external causes after the inclusion of forensic information and 3 were classified as natural.
Suicide cases according to cause of death coding, before and after the recovery of forensic data. Tarragona, 2004–2012.
| Basic cause of death (code ICD-10) | RMC (before) | RMC+DT (after) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Suicide (X60–X84) | 408 | 82.26 | 487 | 97.99 |
| External cause (V00–V99, X00–X58, Y10–Y89) | 30 | 6.05 | 6 | 1.21 |
| Unspecified external cause (X59) | 20 | 4.03 | 1 | .20 |
| Poorly defined (R00–R99) | 21 | 4.23 | 0 | .00 |
| Natural (A00–Q99) | 14 | 2.82 | 3 | .60 |
| Aggression (X85–X99, Y00–Y09) | 3 | .60 | 0 | .00 |
| Total | 496 | 100.00 | 497 | 100.00 |
DT: Tarragona Division of the Institut de Medicina Legal i Ciències Forenses de Catalunya (IMLCFC); RMC: Registre de Mortalitat de Catalunya.
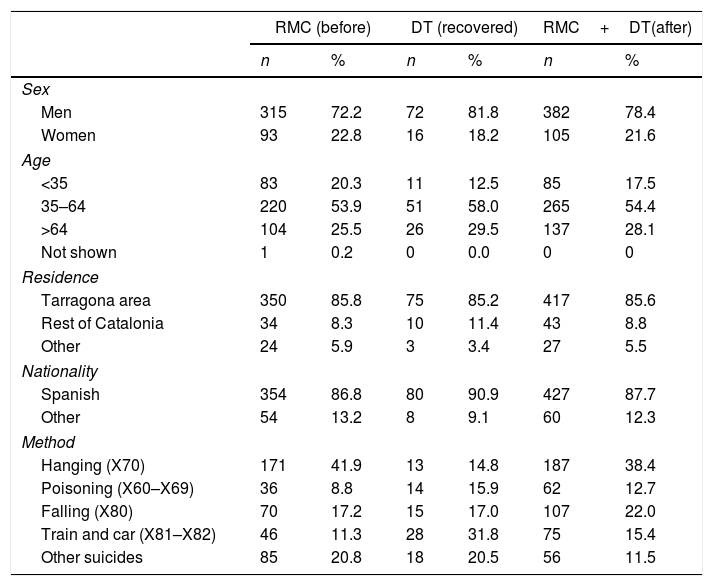
Table 2 shows the demographic characteristics of the DDS cases. In the comparison between the reported and unreported cases, in recent years the higher proportion of men stands out, as do older age groups and more residents in the rest of Catalonia, while there are fewer foreign nationals. Regarding the mechanisms that caused death in the cases reported from the first as suicides, hanging appears more often, to the detriment of poisoning or falls. When the demographic profile of the suicides immediately reported as such are compared with those which were not, no statistically significant different are detected except for the method of suicide, which show a higher proportion of poisonings and being run over by motor vehicles (trains and others) in the recovered information.
Demographic characteristics of suicide cases. Tarragona, 2004–2012.
| RMC (before) | DT (recovered) | RMC+DT(after) | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Sex | ||||||
| Men | 315 | 72.2 | 72 | 81.8 | 382 | 78.4 |
| Women | 93 | 22.8 | 16 | 18.2 | 105 | 21.6 |
| Age | ||||||
| <35 | 83 | 20.3 | 11 | 12.5 | 85 | 17.5 |
| 35–64 | 220 | 53.9 | 51 | 58.0 | 265 | 54.4 |
| >64 | 104 | 25.5 | 26 | 29.5 | 137 | 28.1 |
| Not shown | 1 | 0.2 | 0 | 0.0 | 0 | 0 |
| Residence | ||||||
| Tarragona area | 350 | 85.8 | 75 | 85.2 | 417 | 85.6 |
| Rest of Catalonia | 34 | 8.3 | 10 | 11.4 | 43 | 8.8 |
| Other | 24 | 5.9 | 3 | 3.4 | 27 | 5.5 |
| Nationality | ||||||
| Spanish | 354 | 86.8 | 80 | 90.9 | 427 | 87.7 |
| Other | 54 | 13.2 | 8 | 9.1 | 60 | 12.3 |
| Method | ||||||
| Hanging (X70) | 171 | 41.9 | 13 | 14.8 | 187 | 38.4 |
| Poisoning (X60–X69) | 36 | 8.8 | 14 | 15.9 | 62 | 12.7 |
| Falling (X80) | 70 | 17.2 | 15 | 17.0 | 107 | 22.0 |
| Train and car (X81–X82) | 46 | 11.3 | 28 | 31.8 | 75 | 15.4 |
| Other suicides | 85 | 20.8 | 18 | 20.5 | 56 | 11.5 |
DT: Tarragona Division of the Institut de Medicina Legal i Ciències Forenses de Catalunya (IMLCFC); RMC: Registre de Mortalitat de Catalunya.
The rates show a certain stability over the period studied, for the immediately reported cases as well as for the definitive ones. The exception to this is the year 2008, when mortality was unusually high. The impact of underestimation on the rate as a whole during the period amount to somewhat more than 1 case per 100,000 inhabitants, and this underestimation is not statistically significant.
DiscussionThis paper basically analyses the poor classification of statistical data on mortality due to suicide, comparing the data reported to the RMC with the results of DT-IMLCFC forensic autopsies. The main aim is not so much to validate the cause of death (as this is not a validity study), but rather to evaluate the impact of loss of information on official statistics, underlining the importance of forensically-sourced information.
This study supplies new evidence that statistics in Spain may be underestimated, and that directly including forensically-sourced data in mortality statistics has a beneficial impact. The underreporting of DDS in the area of Tarragona amounted to 16.2% in the period studied as a whole, which is far below the corresponding figures of 104% in the Canary Islands from 1977 to 198311 and 53.1% in the City of Barcelona from 2004 to 2006,8 although it is similar to the 16.1% found by De Aran et al. for a series of deaths examined judicially in Catalonia in 1996.7 The study by Giner and Guija9 also shows that the Legal Medicine Institutions (LMI) reported from 9.3% to 18.7% more DDS than the National Institute of Statistics for the 34 Spanish provinces in which it was possible to obtain numerically complete data.12 The results in Tarragona therefore show that the problem remains, even though it is at a lower level than is the case in the Canary Islands and Barcelona.
The results show that the lack of data and erroneous classification of cases of suicide occur in both directions, while in some cases it is not shown in either of both sources. Many cases were found of suicide reported as due to other causes in the statistics (which was the most common occurrence). However, 10 cases were also found which had been reported as suicide before this autopsy, which then disproved this.
The cases of suicide erroneously reported to the statistical source as due to other causes of death have few differentiating sociodemographic characteristics. This means that they may easily go unnoticed, although fortunately they do not modify the final demographic profile of death by suicide statistics too much. Nevertheless, there are differences respecting the method of suicide. This is because the majority of initial cases are suicides with no information as to the method used, and this data is then supplied in the forensic diagnosis. This aspect may be connected with the number of steps or intermediaries involved in reporting these deaths.13
The significant differences respecting cases of poisoning and being hit by a train may be specifically related to the initial problem of diagnosing the intention of suicide when certain methods are used. This would also explain in part why the DDS with the lowest rate of underreporting are hangings, as here the suicidal intention is more evident and gives rise to fewer doubts. As Giner and Guija point out, DDS are not always easy to identify,9 and in some cases of death it may be necessary to know the results of complementary tests before concluding that a death had a suicidal intention. In the case of toxicological studies, the presence of lethal or toxic concentrations is a very important datum in concluding that deaths by poisoning had a suicidal intention. On the other hand, the detection of psychoactive drugs in therapeutic concentrations is understood in other methods to be a sign of a psychiatric history, and this may support the conclusion that a death had a suicidal intention. Lack of information about a pathological record, which is not always available at first, and cases involving greater bodily destruction (being hit by a train) when there is a lack of information to identify the victim, may partially explain underreporting in such cases.
DDS due to being hit by a train are particularly striking, given that once underreporting has been corrected, they appear as the third most common means of suicide in a proportion of more than 15%, which is the highest percentage described internationally to date.14 This aspect would deserve specific study due to its implications for prevention at a local level, while also monitoring tendencies and railway suicide reduction programmes such as those undertaken in some European countries.15–17
The specific underreporting of suicides by train has been studied by other authors. They compared the official mortality data with the number of suicides reported by railway agencies. For England and Wales Taylor et al. found 5.4% more cases in the railway source.15 Reynders et al. compared the data from 15 European countries and found that as a whole the European Railway Agency reported 34.3% more suicides.18 One of the reasons for this cited by the authors is that a high proportion of these deaths are recorded as indeterminate, as occurs in our case, where a high percentage of deaths are initially classified as due to unspecified and poorly defined external causes. The number of cases is probably lower in mortality statistics due to the difficulty of knowing the intentions underlying the event with any certainty at the moment when information is sent to the statistical document.
In the light of the above considerations, and as Xifró et al.19 point out, the criteria for considering a death to be suicide are relevant, given that there are problems with verifying intentions as well as with cultural attitudes to suicide. They therefore recommend adapting operational criteria such as those used by the United States’ Centers for Disease Control and Prevention20 to our environment or developing similar ones. In this respect the creation and implementation in 2014 of the Forensic Medical Board21 may be a major opportunity for the development of common operational criteria for the definition of a DDS.
There are 2 factors in Spain that make forensic sources the gold standard: a judicial autopsy is obligatory in the case of violent deaths (including DDS) and they are performed in a homogeneous manner (throughout the State by forensic doctors who belong to the LMI).22 This is relevant, as the rate of autopsies and the rate of suicides have a positive correlation. This may affect the validity of suicide mortality statistics, and it should be taken into account when comparing figures with those in other countries.23 The National Institute of Statistics itself, in its results of deaths according to cause for the year 2013, warns that this year data from the Instituto Anatómico-Forense de Madrid are included. These are considered to be a methodological improvement, as they make it possible to assign a more precise cause of death in cases where there was judicial intervention.24
There is a certain degree of agreement that one of the causes of this underreporting of DDS in Spain, as is the case for other causes of death when there was judicial intervention, is the complexity of the process for reporting them statistically. This complexity means that statistical documents reporting deaths in cases with judicial intervention have deficits in how they are filled in, their coverage and their accuracy. The result of all of this is that the circumstances of such deaths are not always properly described in official documents. Thus recovery of the data from forensic sources, as in our case with cases of DDS, makes it possible to improve the quality of statistics. This recovery of the data about cases of deaths with judicial intervention could be undertaken at regular intervals by regional mortality registers in collaboration with the LMI. Other authors support a more active role for forensic doctors or the LMI in the process of statistically reporting these deaths.10 This could take the form of directly and regularly sending information from the LMI themselves to mortality registers, which would require the development of information systems within the IML12 or, as Giner and Guija suggest, that forensic doctors describe the causes of death in the statistical bulletin of death followed by judicial intervention.9,25
In Tarragona, the higher percentages of underreporting (25%) occurred in the years 2009 and 2010. This coincided with the change in the process and documents used to report deaths that were followed by judicial intervention implemented in 2009.26 When the impact of this change was analysed for the municipality of Barcelona in 2010 it showed a loss of 75 DDS,27 which may influence calculation of the rate for this city. As was the case in our study, after completing data using the forensic source the overall rate for the period in this region of Catalonia increased by 1.3 points per 100,000 inhabitants (from 6.6 to 7.9). Although there are variations in underreporting from year to year, as a whole the final rates evolved quite stably up to the year 2012. Nevertheless, it should be pointed out that there is a major increase in the number (and rate) of suicides in 2008 in the original and final data.
The approach selected for this study may limit it in comparison with other similar studies which centre more on validating the cause of death. As we pointed out above, this is not a study of validity, and its aim is to emphasise the effects of a lack of information on suicide statistics and the importance of forensic data as a necessary and complementary source. This is why 4 cases of suicide lacking autopsy data were accepted as such, even though they may have been natural deaths. However, given the small number of these cases they do not give rise to relevant distortion.
ConclusionsThe lack of reliable information about the cause of death leads to underestimation of mortality due to suicide in official mortality statistics. The demographic characteristics of suicides reported as having other causes of death are hardly differentiated, and this hinders their identification in statistics. The exhaustive recovery of DDS data using forensic sources makes it possible to correct this underreporting. It also adds to knowledge regarding the method of suicide and personal characteristics, so that it may be of interest when designing preventive programmes.
Ethical disclosuresProtection of people and animalsThe authors declare that no experiments took place in human beings or animals for this research.
Data confidentialityThe authors declare that no patient data appear in this paper.
Right to privacy and informed consentThe authors declare that no patient data appear in this paper.
Conflict of interestsThe authors have no conflict of interests to declare.
We would like to thank the professionals in the Tarragona Division of the IMLCFC and the coders in the Registre de Mortalitat de Catalunya for their data elaboration work, as well as the IMLCFC for their involvement in the project to improve mortality statistics.
Please cite this article as: Barbería E, Gispert R, Gallo B, Ribas G, Puigdefàbregas A, Freitas A, et al. Mejora de la estadística de mortalidad por suicidio en Tarragona (Cataluña, España) entre 2004 y 2012. Rev Psiquiatr Salud Ment (Barc.). 2018;11:227–233.