




Adult attention deficit hyperactivity disorder (ADHD) has a prevalence between 2.5% and 4% of the general adult population. Over the past few decades, self-report measures have been developed for the current evaluation of adult ADHD. The ADHD-RS is a 18-items scale self-report version for assessing symptoms for ADHD DSM-IV. A validation of Spanish version of the ADHD-RS was performed.
Material and methodThe sample consisted of 304 adult with ADHD and 94 controls. A case–control study was carried out (adult ADHD vs. non-ADHD). The diagnosis of ADHD was evaluated with the Structured Clinical Interview for DSM-IV (SCID-I) and the Conners Adult ADHD Diagnostic Interview for DSM-IV (CAADID-II). To determinate the internal validity of the two dimensions structure of ADHD-RS an exploratory factor analysis was performed. The α-coefficients were taken as a measure of the internal consistency of the dimensions considered. A logistic regression study was carried out to evaluate the model in terms of sensitivity, specificity, positive predictive value (PPV) and negative predictive values (NPV).
ResultsAverage age was 33.29 (SD=10.50) and 66% of subjects were men (there were no significant differences between the two groups). Factor analysis was done with a principal component analysis followed by a normalised varimax rotation. The Kaiser–Meyer–Olkin measure of sampling adequacy tests was .868 (remarkable) and the Bartlett's test of sphericity was 2 (153)=1835.76, P<.0005, indicating the appropriateness of the factor analysis. This two-factor model accounted for 37.81% of the explained variance. The α-coefficient of the two factors was .84 and .82. The original strategy proposed 24 point for cut-off: sensitivity (81.9%), specificity (74.7%), PPV (50.0%), NPV (93.0%), kappa coefficient .78 and area under the curve (AUC) .89. The new score strategy proposed by our group suggests different cut-off for different clinical presentations. The 24 point is the best cut-off for ADHD combined presentation: sensitivity (81.9%), specificity (87.3%), PPV (78.6%), NPV (89.4%), kappa coefficient .88 and AUC .94, and 21 point is the best cut-off for ADHD predominantly inattentive presentation: sensitivity (70.2%), specificity (76.1%), PPV (71.7%), NPV (74.8%), kappa coefficient .88 and AUC .94.
ConclusionsIn this study, the Spanish version of the ADHD-RS is a valid scale to discriminate between ADHD adults and controls. The new proposed score strategy suggests the relevance of clinical presentations in the different cut-offs selected.
El trastorno por déficit de atención e hiperactividad (TDAH) tiene una prevalencia de entre el 2,5 y el 4% de la población general adulta. La Attention Deficit/Hyperactivity Disorder Rating Scale (ADHD-RS) es una escala autoinformada de 18 ítems para la evaluación de los síntomas del TDAH en adultos. El objetivo del presente estudio es realizar la validación de la versión española de la ADHD-RS.
Material y métodoSe incluyó una muestra de 304 adultos con TDAH y 94 controles sanos sin TDAH. El diagnóstico de TDAH se evaluó con la Entrevista Clínica Estructurada para el DSM-IV (SCID-I) y la Entrevista Diagnóstica para TDAH en Adultos de Conners para el DSM-IV (CAADID-II). Para determinar la validez interna de la estructura de 2 dimensiones de la ADHD-RS se realizó un análisis factorial exploratorio. Los coeficientes α se realizaron como medida de la consistencia interna de las dimensiones consideradas. Mediante un estudio de regresión logística se evaluó el modelo en términos de especificidad, sensibilidad, valor predictivo positivo (VPP) y valor predictivo negativo (VPN).
ResultadosLa media de edad de los participantes fue de 33,29 años (DE=10,50), con un 66% de hombres (sin diferencias entre los 2 grupos). El análisis factorial se realizó con un análisis de componentes principales seguido de una normalización por la rotación varimax. La medida de Kaiser-Meyer-Olkin para el test de adecuación de muestras fue de 0,868 (notable) y el test de esfericidad de Bartlett fue 2 (153)=1.835,76, p<0,0005, indicando que el análisis factorial es adecuado. Este modelo de 2 factores explica el 37,8% de la varianza. El coeficiente α de los 2 factores es 0,84 y 0,82. La estrategia original proponía un punto de corte de 24: sensibilidad (81,9%), especificidad (74,7%), VPP (50,0%), VPN (93,0%), coeficiente kappa 0,78 y área bajo la curva (AUC) 0,89. La nueva estrategia de puntuación sugerida por nuestro grupo propone diferentes puntos de corte según las diferentes presentaciones clínicas de TDAH. El punto de corte para la presentación combinada de TDAH es 24: sensibilidad (81,9%), especificidad (87,3%), VPP (78,6%), VPN (89,4%), coeficiente kappa 0,88 y AUC 0,94, mientras que el punto de corte para la presentación predominante con falta de atención sería 21: sensibilidad (70,2%), especificidad (76,1%), VPP (71,7%), VPN (74,8%), coeficiente kappa 0,88 y AUC 0,94.
ConclusionesLa versión española de la ADHD-RS es una escala válida para discriminar correctamente adultos con TDAH de personas sin TDAH. La nueva propuesta de puntuación sugiere la relevancia de las presentaciones clínicas en los diferentes puntos de corte seleccionados.
Attention deficit/hyperactivity disorder (ADHD) is a neural development disorder that is characterised by a persistent pattern of lack of attention and/or hyperactivity and impulsiveness. It is considered to be a chronic disorder that commences in infancy and persists into adult age in more than 50% of cases.1,2 Its prevalence in children is estimated to stand at 5%, while in adults it is about 2.5–4%.1,2
ADHD is associated in adults as well as children with a general pattern of problems in academic performance and social, family and work-related adaptation, giving rise to high economic and healthcare costs.3,4 In spite of its negative repercussions in different areas for adult patients and the fact that effective treatments are available for it,5–7 this disorder is still under-diagnosed and hardly treated, given that only 11% of adults with ADHD receive treatment for it.8 In our area fewer than 0.5% of the general adult population receive psycho-pharmacological treatment for ADHD.9
As is the case for children, the main tool used to diagnose ADHD in adults is their clinical history, so that they have to be questioned on hyperactivity, attention deficit and impulsiveness symptoms throughout their lives. A retrospective diagnosis of symptoms during infancy has to be made, evaluating the continuity of the same in adult age.10–12 There are currently no reliable means of diagnosis, as neither neuroimaging tests nor molecular genetic findings or neuropsychological examinations now have sufficient specificity to form an exact diagnosis.5 Additionally, although the disorder is similar in infancy and adulthood, the fact that its clinical manifestations may change with patient age has to be taken into account. For example, the external hyperactivity of a child with ADHD usually manifests in adults as an internal sensation of psychomotor or motor restlessness.10,11 On the other hand, differential diagnosis is required vs. other pathologies that have similar clinical symptoms. Due to all of the above reasons effective evaluation instruments are necessary for the diagnosis of ADHD in adults.
Different studies have evaluated the psychometric properties of the English versions of the Attention Deficit/Hyperactivity Disorder Rating Scale (ADHD-RS) with good results. The ADHD-RS is a scale that is widely used to evaluate ADHD symptoms in adults.13–18 In spite of this, its validity in the Spanish-speaking population has not yet been evaluated. There are therefore no studies which examine the validity of the criterion of semi-structured interviews in Spanish to diagnose ADHD in adults.
ObjectivesThe aim of this study is to evaluate the validity of the self-informed version of the ADHD-RS in the Spanish population, as well as to evaluate a new proposal for scoring according to the clinical presentation of ADHD.
MethodsTo validate the Spanish version of the ADHD-RS a study of cases and controls was undertaken (adults with ADHD vs. adults without ADHD). This included a sample of 304 adults with ADHD and 94 control individuals selected in the outpatient facilities of the Adult ADHD Program in the Hospital Universitari Vall d’Hebron (HUVH), Barcelona. The subjects were referred to the program from primary care centres, children's neuropsychiatric surgeries o mental health hospitals in Barcelona due to a diagnostic suspicion of ADHD. The study was approved by the Ethics Committee of the HUVH and all of the subjects signed their corresponding informed consent document.
Instruments and procedureThe diagnosis of ADHD was undertaken by experienced psychiatrists and psychologists using the Structured Clinical Interviews I (SCID-I)14 and Conner's Adult ADHD Diagnostic Interview DSM-IV II (CAADID-II).14,15
The SCID-I is a structured interview that offers a systematic method for evaluating the symptoms of the DSM-IV criteria, and it helps to reach exact and standardised diagnoses.14
The CAADID-II14,15 is a structured interview that helps the process of diagnosing adults with ADHD. This evaluation for individuals over the age of 18 years old is divided into 2 parts each of which lasts for approximately 90min. The first part collects information from the clinical history of the patient using a questionnaire that can be self-administered or asked in a clinical interview. This questionnaire contains questions on demographic patient history, the development of attention problems and associated risk factors, as well as comorbidity. The second part takes the form of an interview and it re-evaluates the symptoms of ADHD using DSM-IV criteria. It also gathers data on the age of onset, the severity and dysfunctionality of the said symptoms.
In turn, the evaluation involved the administration of the ADHD-RS to all of the patients included in the study. An exploratory factorial analysis was performed with the sample of adults with ADHD to determine the degree of internal validity of the structure of the ADHD-RS, which obtained 2 factors. The α coefficients were taken to measure internal consistency, and a logistic regression was performed to evaluate the model in terms of its sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV).
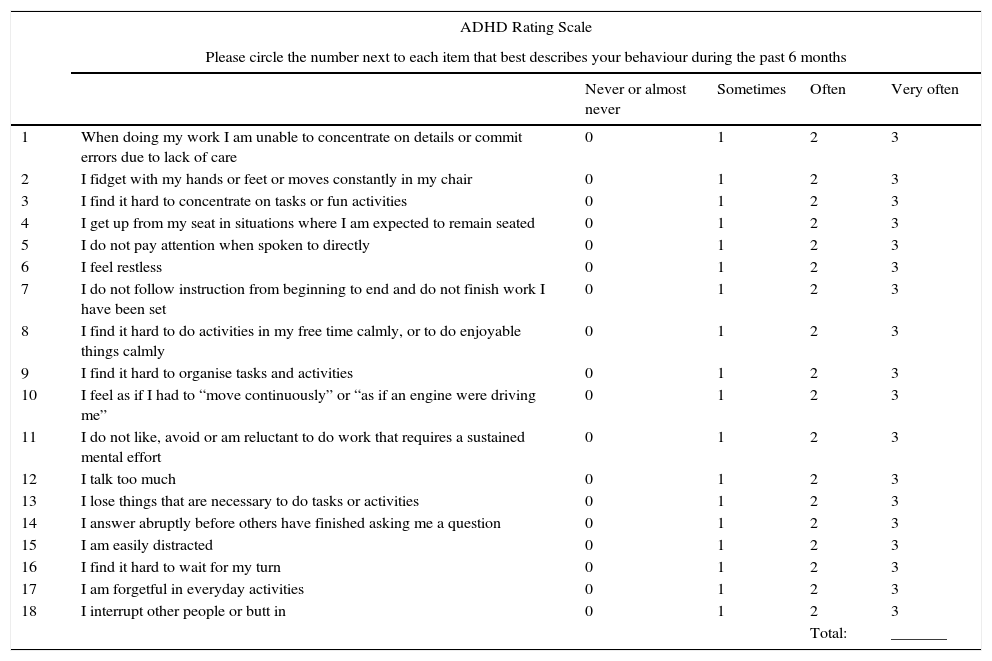
The ADHD-RS is a scale of 18 items which reflects DSM-5 criteria for ADHD. It consists of a lack of attention sub-scale (IN, 9 items), another on hyperactivity/impulsiveness (H/I, 9 items) and the total (TOT, 18 items)17,18 (Appendix A). The sentences do not start with “often”, and interviewees are asked about how often the said symptoms have occurred to them during the past 6 months. Each item is scored from 0 to 3 points, and the highest scores indicate the presence of problematic behaviour. The final score of the ADHD-RS consists of a summary of the direct scores that is independent of the evaluator.19 This questionnaire may be administered by an expert clinician, or it may be self-administered by the patient or a direct family member. Although it was initially designed for administration in infant patients, it has been adapted for adult subjects.
Statistical analysisFor statistical analysis a descriptive study was first carried out of the variables studied, and the χ2 test was used for comparative analysis. Subsequently the same examination strategies were used for each of the 2 decision strategies and for each cut-off point. This is a set of logistic regression analyses that permit evaluation of the fit of each model in terms of sensitivity (the probability that a subject with ADHD will score positively in the test), specificity (the probability that a subject without ADHD will score negatively in the test), PPV (the probability that a subject who scored positively really is a subject with ADHD) and NPV (the probability that a subject who scored negatively really is a subject without ADHD). The respective κ rates were also calculated according to the estimated and actual group subjects belonged to, as well as the area under the curve (where a value of 1 indicates maximum agreement between the foreseen diagnosis and the one observed). Factorial analysis was undertaken using analysis of the main components followed by normalisation with varimax rotation, obtaining 2 factors.
ResultsThe sample consists of 304 adults with ADHD and 94 control subjects, with an average age of 33.29 years old (SD=10.50) of whom 66% are men. No significant differences emerged in data analysis between the 2 groups according to age and sex.
The degree of fit of the Kaiser–Meyer–Olkin test was 0.868 (notable) and Bartlett's sphericity test score was |2 (153)=1835.76, P<.0005, indicating that the factorial analysis is appropriate. The kappa coefficient for agreement between observers was 0.78 and the area under the curve was 0.89, indicating good test reliability.
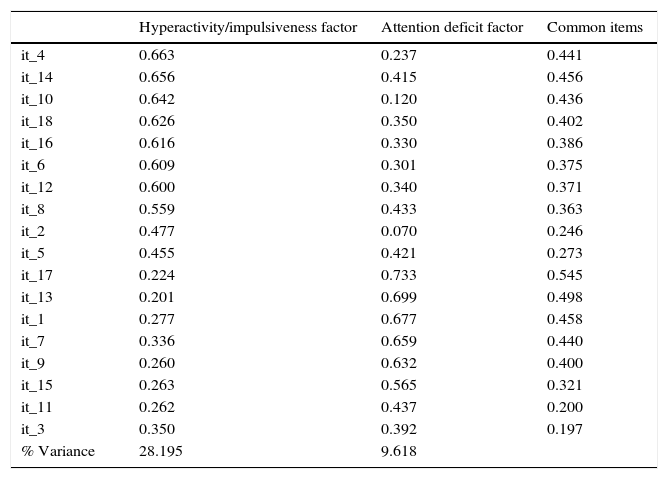
Table 1 shows the factorial weightings of each item of the retained rotated components, as well as the common elements and the percentage of variance explained by each component. This 2 factor model represents 37.81% of the variance. The α coefficients of both factors were 0.84 and 0.82.
Results of analysis of the main components obtained in varimax rotation, an assignation of 2 factors, common items and the percentage of variance explained of the ADHD-RS in the Spanish population.
| Hyperactivity/impulsiveness factor | Attention deficit factor | Common items | |
|---|---|---|---|
| it_4 | 0.663 | 0.237 | 0.441 |
| it_14 | 0.656 | 0.415 | 0.456 |
| it_10 | 0.642 | 0.120 | 0.436 |
| it_18 | 0.626 | 0.350 | 0.402 |
| it_16 | 0.616 | 0.330 | 0.386 |
| it_6 | 0.609 | 0.301 | 0.375 |
| it_12 | 0.600 | 0.340 | 0.371 |
| it_8 | 0.559 | 0.433 | 0.363 |
| it_2 | 0.477 | 0.070 | 0.246 |
| it_5 | 0.455 | 0.421 | 0.273 |
| it_17 | 0.224 | 0.733 | 0.545 |
| it_13 | 0.201 | 0.699 | 0.498 |
| it_1 | 0.277 | 0.677 | 0.458 |
| it_7 | 0.336 | 0.659 | 0.440 |
| it_9 | 0.260 | 0.632 | 0.400 |
| it_15 | 0.263 | 0.565 | 0.321 |
| it_11 | 0.262 | 0.437 | 0.200 |
| it_3 | 0.350 | 0.392 | 0.197 |
| % Variance | 28.195 | 9.618 |
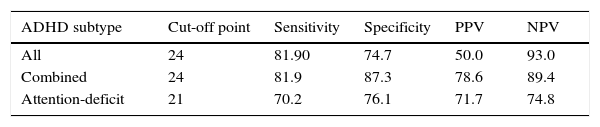
Table 2 shows the psychometric properties of the self-administered ADHD-RS for different score cut-off points. Initially a cut-off point at 24 was proposed, with a sensitivity of 81.9%, a specificity of 74.7%, a PPV of 50.0% and a NPV of 93.0%. The new score proposed by our group suggests different cut-off points depending on the different clinical presentations of ADHD. The best cut-off point for combined ADHD would be 24 points, and 21 points would be the best cut-off point for predominantly attention-deficit ADHD.
DiscussionThe study results show that the adaptation of the ADHD-RS for adults into Spanish has suitable psychometric properties for use as an evaluation scale in the screening and diagnosis of adults with ADHD. It has to be pointed out that after an exhaustive review no validations of this scale in an adult population were found. Nevertheless, validations were found for children and adolescents,20,21 as well as other instruments to aid the diagnosis of ADHD in adult populations in other countries.22–24 An example of these is the semi-structured interview “Assessment System for Individuals with ADHD” (ASIA),which stands out for its validity in adult and Spanish-speaking populations,22 although further research is still required.25
The Spanish version of the ADHD-RS is a valid scale for differentiating adults with ADHD from subjects without the disorder. These results are similar to those obtained in the original studies with samples of children by DuPaul et al. in 1998.26 The attention deficit sub-scales as well as those for hyperactivity/impulsiveness were useful in predicting the clinical and control groups. The new proposed scoring strategy suggests the relevance of the cut-off points selected in the different clinical presentations of ADHD. The use of different cut-off points depending on the clinical presentation of ADHD is important because we have to take into account the fact that patients with ADHD that predominantly consists of attention deficit may sometimes go undetected by current screening tests. This is due to reduced intensity of the symptoms in this group in comparison with patients with combined ADHD, as they do not show as many symptoms expressing hyperactivity-impulsiveness.
The need to make an effort to include all of the available clinical data when evaluating adults with ADHD must also be taken into account, to help with the diagnosis.8 A standardised protocol should include a complete clinical history of the patient, a self-administered questionnaire on symptoms, neuropsychological performance and the evaluation of psychopathological comorbidities. It is therefore important to use self-administered scales such as the ADHD-RS, as this will supply exact and valuable data on the severity and course of the disorder.27 In spite of this, we have to be cautious when interpreting these results, as the study was performed in a clinical sample and not in the general population.
When it is used within a suitable evaluation battery that includes diagnostic interviews, observations of behaviour and related measurements, the ADHD-RS is able to offer valid reliable data on the frequency of ADHD symptoms.27
To conclude, the availability of validated instruments in our field for the diagnosis and evaluation of ADHD in this population is highly important, due to the functional difficulties suffered by adults with ADHD28 as well as the high degree of comorbidity which worsens the course of the disease.8,27,29
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they have adhered to the protocols of their centre of work on patient data publication.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe author J.A.R.Q. has given conferences and/or has acted as a consultant for Eli-Lilly, Janssen-Cilag, Novartis, Shire, Lundbeck, Almirall and Rubió in the past 3 years. He also received travel rewards (air tickets + hotel) for taking part in psychiatric meetings, from Janssen-Cilag, Rubió, Shire and Eli- Lilly. The ADHD program he chairs received unrestricted educational and research support from the following pharmaceutical companies in the last 3 years: Eli-Lilly, Lundbeck, Janssen-Cilag, Actelion, Shire and Rubió.
We would like to thank the patients and control individuals who kindly took part in this study. The European Commission 7th framework program for research, technological development and demonstration (AGGRESSOTYPE_FP7HEALTH2013/602.805). This research was supported by the Instituto de Salud Carlos III (PI14/01700), the Agencia de Gestión de Ayudas Universitarias y de Investigación-AGAUR, Generalitat de Catalunya (2014SGR1357), the European College of Neuropsychopharmacology (ECNP network: “Whole life ADHD”), Departament de Salut, Generalitat de Catalunya, Spain. This project also received financing from the European Union Horizonte 2020 program for research and innovation under grant agreements No. 667302.
| ADHD Rating Scale | |||||
|---|---|---|---|---|---|
| Please circle the number next to each item that best describes your behaviour during the past 6 months | |||||
| Never or almost never | Sometimes | Often | Very often | ||
| 1 | When doing my work I am unable to concentrate on details or commit errors due to lack of care | 0 | 1 | 2 | 3 |
| 2 | I fidget with my hands or feet or moves constantly in my chair | 0 | 1 | 2 | 3 |
| 3 | I find it hard to concentrate on tasks or fun activities | 0 | 1 | 2 | 3 |
| 4 | I get up from my seat in situations where I am expected to remain seated | 0 | 1 | 2 | 3 |
| 5 | I do not pay attention when spoken to directly | 0 | 1 | 2 | 3 |
| 6 | I feel restless | 0 | 1 | 2 | 3 |
| 7 | I do not follow instruction from beginning to end and do not finish work I have been set | 0 | 1 | 2 | 3 |
| 8 | I find it hard to do activities in my free time calmly, or to do enjoyable things calmly | 0 | 1 | 2 | 3 |
| 9 | I find it hard to organise tasks and activities | 0 | 1 | 2 | 3 |
| 10 | I feel as if I had to “move continuously” or “as if an engine were driving me” | 0 | 1 | 2 | 3 |
| 11 | I do not like, avoid or am reluctant to do work that requires a sustained mental effort | 0 | 1 | 2 | 3 |
| 12 | I talk too much | 0 | 1 | 2 | 3 |
| 13 | I lose things that are necessary to do tasks or activities | 0 | 1 | 2 | 3 |
| 14 | I answer abruptly before others have finished asking me a question | 0 | 1 | 2 | 3 |
| 15 | I am easily distracted | 0 | 1 | 2 | 3 |
| 16 | I find it hard to wait for my turn | 0 | 1 | 2 | 3 |
| 17 | I am forgetful in everyday activities | 0 | 1 | 2 | 3 |
| 18 | I interrupt other people or butt in | 0 | 1 | 2 | 3 |
| Total: | _______ | ||||
Please cite this article as: Richarte V, Corrales M, Pozuelo M, Serra-Pla J, Ibáñez P, Calvo E, et al. Validación al español de la ADHD Rating Scale (ADHD-RS) en adultos: relevancia de los subtipos clínicos. Rev Psiquiatr Salud Ment (Barc). 2017;10:185–191.