






The objective of this work is to compare the cases of transsexuality studied in the Forensic Medical Clinic of Madrid with those published in other series.
Material and methodsA retrospective, descriptive, cross-sectional, and observational study was carried out by collecting a series of data from the reports issued by forensic doctors attached to the Forensic Medical Clinic of Madrid, from 11 January 1995 to 4 May 2007.
ResultsA total of 52 reports were obtained in relation to transsexuality, of which 29 were from male to female (55.76%), and 23 from female to male (44.23%). It was noted that the majority lacked psycho-pathological disorders (72.4/65.2% male/female, respectively), the early onset of transsexual sentiment (86.2/100%), the age of re-assignment surgery (male between 18 and 41 years of age; female, between 22 and 43 years old), and its proximity to the application for change of registration.
ConclusionsThe study emphasises the high incidence of absence of psycho-pathological problems (observed in approximately one-third of the cases), the precociousness in the appearance of the transsexual feeling and the proximity between the surgery and the application for registration, conditioned by the current legal requirements. The results obtained in the present study are compared with other series, taking into account the difference in the procedures used.
El objetivo de este trabajo es el de comparar los casos de transexualidad peritados en la Clínica Médico Forense de Madrid con los publicados en otras series.
Material y métodosSe trata de un estudio retrospectivo sobre los informes emitidos por médicos forenses adscritos a la Clínica Médico Forense de Madrid, desde el once de enero de 1995 hasta el cuatro de mayo de 2007, recogiendo una serie de datos y realizando un estudio observacional descriptivo y transversal.
ResultadosSe han obtenido 52 informes en relación con transexualidad, de los que 29 eran de hombre a mujer (55,76%) y 23 de mujer a hombre (44,23%). Se recoge que la mayoría carecían de alteraciones psicopatológicas (72,4/65,2% hombre/mujer respectivamente), la aparición precoz del sentimiento transexual (86,2/100%), la edad de la cirugía de reasignación (hombres entre 18 y los 41 años de edad; mujeres, entre los 22 y los 43 años de edad), y su proximidad a la solicitud de cambio de inscripción registral.
ConclusionesDestaca la alta incidencia de ausencia de alteraciones psicopatológicas (hemos objetivado estas alteraciones aproximadamente en un tercio de los casos), la precocidad en la aparición del sentimiento transexual y la proximidad entre la cirugía transexual y la solicitud de inscripción registral, condicionado por los requisitos legales del momento. Los resultados obtenidos en nuestro estudio son comparables con otras series, teniendo en cuenta la diferencia de procedimientos empleados.
When there is a noticeable mismatch between the gender experienced or expressed and the gender assigned, with an intense desire to belong to the gender experienced, a situation that causes anguish or clinically significant impairment, we find ourselves before what the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)1 considers and defines as gender dysphoria (F64), a situation comparable to that which the Diccionario de la Lengua Española [Dictionary of the Spanish Language] (tercentenary edition, 2017 update) lists as transsexual, with definitions of: belonging or relating to gender reassignment; person who feels as though they are of the opposite sex and adopts their dress and behaviour; that which by hormone treatment and surgical procedure acquires the sexual characteristics of the opposite sex.
The International Classification of Diseases, 10th Revision (ICD-10)2 defines three different gender identity disorders: gender identity disorder of childhood, dual-role transvestism and transsexualism, which the DSM-IV-TR3 lists within the same category, called gender identity disorder.
The expert committee of the World Health Organisation (WHO) in charge of reviewing mental disorders (Chapter F), and in particular F64.0, is evaluating the creation of a chapter in which the names proposed are gender dysphoria, gender-body mismatch, gender mismatch and other similar terms.4
There is no specific diagnostic test for gender identity disorder. In the presence of a normal physical examination, performing a karyotype of the sex chromosomes or determinations of the corresponding hormones is not indicated. Psychological tests may reveal an identification or behaviour patterns of the other sex.
There are various theories with regard to transsexuality (psychoanalytical, social learning, development and role),5 to which we can add biological theories.6
Until the legal amendments, it was practically impossible to declare a change of sex in the national identity document, Registry Office, etc., if gender reassignment surgery had not taken place beforehand, with the forensic medical report and court decision being required. The decriminalisation in 1983 of certain lesions (organ transplant, sterilisations and transsexual surgery) upon consent7 allowed specific surgical techniques, performed legally and by physicians, to be undertaken. Spanish Law 3/2007, of 15 March, Regulator of the Amendment of the Registry of the reference relating to the sex of individuals,8 means that it is not necessary for surgery prior to the request to change the registered sex, and essentially sets out that the applicant, of legal age and Spanish, should prove:
- a)
Existence of gender dysphoria, by means of a report from a doctor or clinical psychologist, which should refer to:
- 1.
Existence of discordance between the morphological sex or physiological gender initially registered and the gender identity felt by the applicant or psychosocial gender, as well as the stability or persistence of this discordance.
- 2.
Absence of personality disorders that could influence the existence of this discordance.
- b)
That they have been treated medically for at least two years to adapt their physical characteristics to those of the claimed gender, by means of a report from the doctor under whose direction the treatment has been performed or, failing this, from a specialist forensic doctor.
This Law8 establishes that gender reassignment surgery is not necessary, and that the treatments mentioned in the previous section will not be essential on grounds of age or health, providing medical certification of these aspects. We can therefore see that, with the legislative change, the role of the forensic doctor will be merely occasional, surgery unnecessary, and the possibility of increasing the clinic's file unlikely.
ObjectivesThe objectives proposed in this study are for both male and female transsexuality:
- 1.
To determine the number of transsexuals in both directions studied at the Forensic Medical Clinic of Madrid, the relationship of transsexuality by gender and the incidence in the population.
- 2.
To determine the existence of psychopathological processes and of possible consumption of substances of abuse in these subjects.
- 3.
To determine the time of onset of the transsexual feeling.
- 4.
To assess the type of sexual relationships maintained.
- 5.
To determine the age of initiation of legal proceedings, of the performance of gender reassignment surgery and the type of procedure.
- 6.
To compare these results with other studies and publications carried out on the same topic.
The field in which the study was conducted is made up of reports issued by forensic doctors affiliated to the Forensic Medical Clinic of Madrid, from 11 January 1995 to 4 May 2007, having selected all the reports issued on transsexuality, after obtaining authorisation from His Lordship, Magistrate-Senior Judge of the Courts of Madrid, with the study proposal and the commitment to secrecy appearing in the application.
MethodsThe sheet to fill in for the study lists: name, age, date of application, profession, age of onset of the feeling, psychopathological study, drug use, relationships, hormone treatment and surgical treatment. Based on the data collected in the sheets obtained from the reports included in the study, a descriptive, observational and cross-sectional study was conducted, both for males and females, and percentages were determined. The Clinic's results are compared with the main authors and publications on the subject: DSM-IV-TR,3 Benjamin,9 Pauly,10,11 Edgerton,12 Lothstein,13 Wälinder,14 Mercader,15 Szazs16 and Hoenig.17
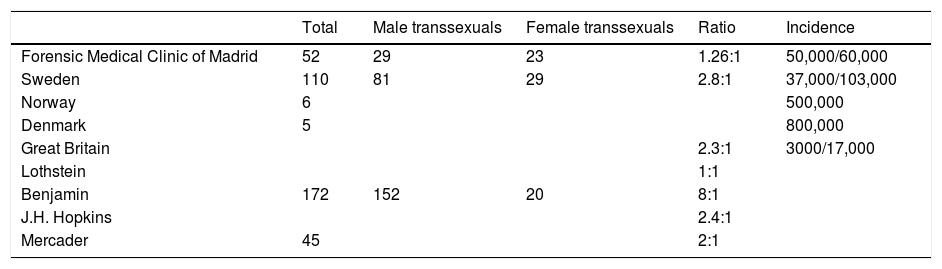
ResultsFifty-two expert reports regarding transsexuality were obtained, 29 of which were male to female (55.76%) and 23 female to male (44.23%) (Table 1).
Case study, ratio and incidence of transsexuality in both directions.
| Total | Male transsexuals | Female transsexuals | Ratio | Incidence | |
|---|---|---|---|---|---|
| Forensic Medical Clinic of Madrid | 52 | 29 | 23 | 1.26:1 | 50,000/60,000 |
| Sweden | 110 | 81 | 29 | 2.8:1 | 37,000/103,000 |
| Norway | 6 | 500,000 | |||
| Denmark | 5 | 800,000 | |||
| Great Britain | 2.3:1 | 3000/17,000 | |||
| Lothstein | 1:1 | ||||
| Benjamin | 172 | 152 | 20 | 8:1 | |
| J.H. Hopkins | 2.4:1 | ||||
| Mercader | 45 | 2:1 |
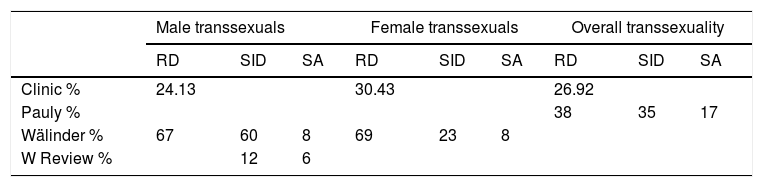
Psychopathologies were not observed in 21 cases (72.4%), three had mild reactive depression (10.3%), and another four (13.8%) had more severe reactive depression which required treatment. One case, who had taken recreational drugs temporarily in his youth, had anxiety attacks that required treatment (3.4%) (Table 2).
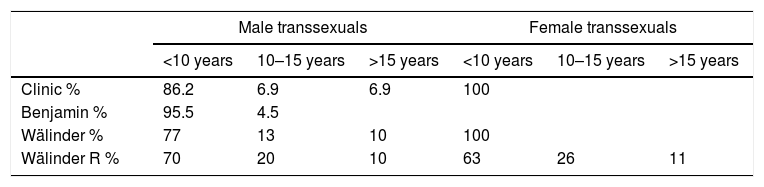
In 25 cases (86.2%), the transsexual feeling developed in childhood, in two (6.9%) it started in adolescence as a homosexual tendency and in another two (6.9%) there were clear transsexual tendencies in adolescence (Table 3).
The majority of cases which involved sexual relationships (19, 65.5%) were heterosexual (15 cases, 51.7%). On one occasion (3.4%) and despite having feelings of belonging to the other sex, the individual got married and, while sporadically maintaining sexual relations with his partner, did not reach climax on any occasion. In another case (3.4%), there was only one attempt to maintain a relationship with a woman, which failed. Two cases (6.8%) initially maintained relationships from a homosexual point of view, until the transsexual feeling became more established and they then went on to have relationships with men from a heterosexual point of view. Five cases (17.2%) reported never having had a sexual relationship. One case (3.4%) expressed bisexuality and in six (20.7%), this information was not recorded. The remaining cases (13, 44.8%) had relationships exclusively from the heterosexual point of view with men.
The greatest incidence in terms of age at the beginning of legal proceedings was recorded between the ages of 25 and 35 (21 cases, 72.4%), with the earliest initiation of proceedings at 21 and the latest at 42. Surgical treatments ranged between the ages of 18 and 41. The age of gender reassignment surgery was very close to the legal application (Table 4).
Range and ages of initiation of legal proceedings, first consultation and surgical reassignment.
They had been treated with hormones in all cases, and in 27 (93.1%), genital surgery had been performed (bilateral orchiectomy, removal of the corpora cavernosa, vaginoplasty using penile skin between the bladder and rectum, reconstruction of the labia majora with scrotum) and 23 (79.3%) had mammoplasty surgery. Eight cases (27.6%) underwent plastic surgery (Table 5).
Female transsexualityPsychopathologies were not observed in 15 cases (65.2%), seven presented episodes of reactive depression (30.4%) and one case (4.3%) presented low tolerance to frustration and drug use (cannabis between the ages of 16 and 18) (Table 2).
In all cases, the onset of transsexual feeling occurred in childhood (Table 3).
Eighteen cases (78.2%) had sexual relationships, 17 (73.9%) of which were from the heterosexual point of view. Fifteen cases (65.2%) had sexual relationships exclusively with women from the heterosexual point of view. In two cases (8.7%), there was an attempt to have a relationship with a male, which failed, and they then went on to have a relationship with a heterosexual female. Three cases (13.0%) had never had a relationship. One case (4.3%) had a relationship with a homosexual male, taking the male role, and in two (8.7%) it is not recorded.
The age of onset of legal proceedings ranged from 23 to 47, with the greatest incidence of cases at the age of 32. The age at which gender reassignment surgery was performed ranged from 22 to 43. The age of gender reassignment surgery was very close to the legal application (Table 4).
All cases (100%) had been treated with hormones and undergone a mastectomy, and 21 (91.3%) underwent a hysterectomy; in nine cases (39.1%), reassignment surgery had been performed (phallus-urethroplasty), in five cases (21.7%), testicular prostheses had also been fitted, and in two (8.6%), penile prostheses were implanted (Table 6).
DiscussionIn terms of the number of transsexuals in both directions, ratio of transsexuality by gender and incidence in the population during the period that the study covers, our study found a male/female ratio of 1.26:1 (Table 1). The data from some European countries suggest that one in every 30,000 males and one in every 100,000 females desire surgical treatment.3 In Sweden,14 it has been determined that there is one case of transsexuality for every 54,000 inhabitants; among the 110 cases that Wälinder lists, 81 are males and 29 females, a ratio of 2.8:1. This would result in one case among males in every 37,000 inhabitants and one in every 103,000 among females. The same author has collected figures from the literature of six cases from 3 million inhabitants in Norway, five from 4 million inhabitants in Denmark, and one in every 3000 males to one in every 17,000 females in Great Britain, with a male/female ratio of 2.3:1. The Clinic's study found a legal application for gender reassignment in one in every 50,000 males and one in every 65,000 females. For Lothstein, who published a long discourse on female transsexuality,13 the figures appear to be close to a ratio of 1:1. For other authors, the ratio between males and females who wished to have a gender transformation operation has been established at a ratio of 8:1 (Benjamin9 and Pauly11). The Clinic's results regarding the proportion between sexes are quite similar to those of Lothstein13 and those provided by Sweden, in which the same number of males and females have requested legal gender reassignment. At the John Hopkins University Hospital, the average male to female ratio for requests for a gender reassignment operation is 2.4:1, while Benjamin,9 as we have already mentioned, found the number of males to be eight times higher than females. It seems that there is a certain prevalence in the number of males who wish to undergo gender reassignment compared to females, in line with the results from the Clinic. Patricia Mercader15 collected 70 judgements from French courts issued between 1965 and 1992; from this date, the applications per year in Paris were 25; two thirds were male and one third female (2:1); half of the decisions were negative, and the requests from women were accepted with slightly greater frequency. Mercader studied 45 judgements in detail, 15 of which were females and 30 males; the ages of the applicants ranged between 21 and 66; the mean age for females was less than 35 (time at which they requested the authorisation to undergo an operation), and the mean age for males was over 38. In general, before 1975, only errors in gender registration were admitted; from this date transsexualism was then considered; and after the judgements of the Court of Human Rights in 1992, the jurisprudence was amended radically.15 This study also found a greater prevalence of males, in line with the Clinic's results (Table 1).
The study on the presence of psychopathological processes is listed in Table 2. Stoller's definitions, published in 1968 in “Sex and Gender”,18 established the criteria for being operated on, referring essentially to transsexual males: feminine character, not having gone through stages of masculinity nor having considered oneself to be a man, having expressed femininity from a young age, not giving value to the penis, not having been married, no children nor being delusional. The fundamental criterion for inclusion in the framework of transsexuality is the exclusion of a major psychiatric disorder. This was confirmed in all the cases that we considered, although some strictly reactive symptoms to the situation in which they found themselves were identified. For some authors,9 the reactive symptoms are a consequence of the individual not only wishing to pretend that he/she is of the other sex, but having the desire to be so, with suffering due to these ego-dystonic symptoms. Consumption of alcohol or recreational drugs is occasionally reported, to obtain false relief, and individuals may even become candidates for self-mutilation (four cases listed among 152 male transsexuals, who reported doing so to force surgical reconstruction after the mutilation. Some suicides were also recorded, listed as of “unknown” cause, but which were related to the impossibility of gender reassignment and the subsequent frustration). In studies performed in a series of 43 cases,14 68% of cases of reactive depression (67% in males and 69% in females), with suicidal ideations in 49% (60% in males and 23% in females) and suicide attempts in 16% (20% and 8%, respectively) were compiled. In other series,10 depressive reactions were found to be 38%, suicidal ideations 35% and attempts 17%. In a review of 207 cases from the literature,14 12% presented suicidal ideations and 6% suicide attempts; it is considered that the higher suicide percentages among males is due to the fact that they suffer greater observation and rejection by society (which would also partly explain the greater incidence of transsexuality among males) (Table 1). As Hoenig and Torr state, it is not hermaphroditism, and genetically they do not present abnormalities, with normal chromatin patterns.17 The Clinic's results show lower rates of reactive symptoms than in the other series. This is very probably due to the fact that when the legal application for gender reassignment was submitted, the individual could already see the light at the end of the tunnel. Regarding the few cases in which substances of abuse were consumed, this was on a temporary basis and possibly as an escape route given their frustrating situation.
The time of onset of the transsexual feeling is recorded in Table 3. Money19 considered that the gender was so well “established” after two and a half years that it was difficult to perform a gender reassignment, and he compared it to the imprinting of some animal species, which starts in the first year of life, even at the time of birth. In “The Transsexual Phenomenon”,9 it is stated that among the 51 cases of males who had been operated on, the feeling had developed in 43 cases in early childhood, in two during puberty and in six cases it was not recorded. In total, Wälinder14 lists an age of onset of the feeling of belonging to another gender in 43 cases: in 36 cases before the age of 10 (84%), in four between the ages of 10 and 15 (9%) and in three between the ages of 15 and 25 (7%). For males, onset occurred in childhood in 23 (77%), in adolescence in four (13%) and in the rest between the ages of 15 and 25 (10%). For females, the figures are 100% (13 cases) in early childhood. The author reviews a total of 156 published cases (137 males and 19 females) and, for males, finds an age of onset of the feeling in 96 cases (70%) before the age of 10, 28 cases (20%) between the ages of 10 and 15 and 13 cases (10%) after the age of 15, with the equivalent figures for females being 12 (63%) 5 (26%) and 2 (11%), respectively. The Clinic's results, in particular regarding the age of onset of the transsexual feeling, are identical to those of Wälinder in transsexual females: in all cases the age of onset was in early childhood. With regard to transsexual males, the results of the Clinic's series are halfway between those of Benjamin9 and those of Wälinder14; it must be taken into account that the series of these authors are not cases that submit legal applications, but instead they are care cases, meaning that the sample is not completely comparable.
Regarding the type of sexual relationships maintained, in those cases in which there could have been a homosexual beginning, this failed, and when there were relationships, they were always from the heterosexual point of view, with the exception of one case of male transsexuality, with bisexual behaviour, and one case of female transsexuality in which, although male behaviour was adopted, there was a relationship with a homosexual male. Transsexuality should not be confused with homosexuality. Sexual orientation refers to both the sexual and romantic and emotional attraction towards other people. In the case of homosexuals, their gender identity remains consistent with their sexual anatomy,9 a situation which is clearly different from transsexuals. Transsexuals who try to resolve their gender dysphoria by trying to adopt a homosexual identity eventually fail, and they resolve the conflict only through gender reassignment. In a large number of transsexuals, sexuality is, in itself, something secondary, which barely concerns them or which remains suppressed, in relation to gender identity. Of the 51 males listed by Benjamin,9 12 had been married beforehand as males before the surgery; following surgery, 12 got married as females; in five cases both experiences coincided (they failed as males, and some did not even consummate the marriage); five got divorced as females and three got married again one or more times; among the 39 who did not get married, 23 had had sexual relationships, and, of them, nine practised prostitution part or full time. Of the 20 females, five had been married as females (with the desire of reversing the tendency, or under pressure from their family or to escape family control); all cases ended in annulment or divorce, and in one case there was a reversal of roles; some marriages were never consummated; in three cases there were four pregnancies, with one abortion, one death at birth and two normal births. Among the nine females who underwent surgery, six got married as males with females; two had been married before and four after the surgery; there were no cases of divorce; in two cases the patients experienced marriage as both female and male. One of the nine cases, who had previously been married and divorced, tried to live as a male after the surgery but returned to the female role and restored the appearance of her breasts by plastic surgery. In one study of 43 cases,13 93% of the males were mentally aroused by people of the same sex from birth, and 100% of the females. Fifty-three per cent (53%) of males and 61% of females had maintained fundamentally or exclusively homosexual experiences, 20% of males and 8% of females had maintained heterosexual experiences and 27% of males and 31% of females had not had any type of relationship (expressing a lack of desire or preferring to wait until the sex change). In all cases, they denied having relationships from the homosexual point of view, and denied that their partner was homosexual.
The mean age at which legal proceedings for gender reassignment were started is shown in Table 4 and the treatments in Tables 5 and 6. Pauly10 lists 100 cases of male transsexuality from the literature; of the first 28 published, 16 had undergone some type of procedure; all had been castrated, seven had undergone penectomy and artificial vaginas had been created in six. This author found that in some cases, there was what he called a polysurgical attitude, requiring successive plastic surgery procedures, with an average of 3.5 procedures in cases of female to male gender reassignment. A total of 30% of Edgerton's patients12 wished to undergo rhinoplasty, vocal cord alteration and use of silicone to alter the contours of the face, lips and hips. This was a similar percentage to that of our series. Up to 1964, Benjamin9 had studied 152 males who fulfilled the transsexuality criteria. Of them, 51 underwent surgery. Of those who underwent surgery in the United States, the majority involved creating the vaginal canal with skin from the thigh, but for those who had been surgically treated in Casablanca, inverted skin from the penis had been used; in two cases an intestinal loop was used. The ages at the time of the surgery were: 23 cases were in their twenties, 14 in their thirties, 11 in their forties and three in their fifties. The oldest was 58 and the youngest 20, with a mean age of 33.2. Of the 20 women included in the same study, most were in their twenties, one was aged between 10 and 20, four in their thirties and three in their forties. The mean age was 30.3. Sixteen cases received androgen therapy. Nine underwent a hysterectomy, accompanied by an oophorectomy, except in one case. The mean age at the time of the operation was 35.5. Four patients were in their twenties, two in their thirties, two in their forties and one in her fifties. In five cases only mastectomy was performed. Mastectomy and hysterectomy were performed in five cases. In another four cases, hysterectomy without mastectomy was performed. Mercader15 found that the ages of the applicants for a legal procedure in France ranged between 21 and 66; the mean age for women was less than 35 (the time at which they requested the authorisation to have surgery), and the mean age for males was over 38 (Table 4). Other authors16 found that the age of the first medical consultation was 24.5 in males and 22.5 in females (these figures represent initial medical consultations, not surgical consultations or the legal application for gender reassignment).
In the Clinic, markedly higher percentages of male transsexuals who have undergone surgery were collected than in Benjamin's series. However, it must be remembered that this author closed his clinical study in 1964, and that the Clinic's study closed more recently, in an age of more advanced surgical techniques and no secrecy surrounding surgery, performing surgery on cases with legal applications, whose requirements were up to forthcoming dates, to obtain a positive outcome, having previously undergone surgery (Table 5). However, regarding the cases of transsexual females, the case study is similar; this could be interpreted as explained by less social pressure on women who feel that they are of the opposite sex, which has already been mentioned, which is why their surgical percentage is significantly lower than in males (Table 6). Regarding the ages at the time of undergoing surgery, both the Clinic's series and Benjamin's series present a greater number of cases between the ages of 20 and 40, with a sharper decline in the Clinic from the age of 40 to 50. At these ages, the individual may have the financial means to undergo surgery, and their state of health is good enough to tolerate possible repeat operations. The range of ages of the Clinic's series is similar to that of Benjamin's series, and somewhat less broad than Mercader's series. In females, legal proceedings are sought at similar ages in all three series, and at a slightly younger age in France than for males in that study, which is contrary to our findings. The ages of gender reassignment are similar in both males and females, comparing our study with that of Benjamin, with the age being slightly higher in the group of transsexual females. We cannot compare our study with the age at the time of the first medical consultation, which is merely for care or informative purposes. In the transsexual males who underwent surgery, the Clinic's series is comparable to that of Benjamin in terms of percentage and type of reassignment surgery. Regarding transsexual females, in the series which we studied in the Clinic, all cases underwent a procedure, with phalloplasty being particularly predominant; however, in the 1964 series, and perhaps because the techniques with regard to the male organ were not so refined, patients exclusively underwent vaginectomies and mastectomies.
This study has limitations, such as the number of cases, the fact that a retrospective assessment was carried out, and that the series published are not homogeneous.
ConclusionsAt the Forensic Medical Clinic of Madrid and in the period covered by the study, expert reports were issued for 29 male transsexuals and 23 female transsexuals. The ratio of male to female transsexuals is 1.26:1, and the incidence in the population is one case of male transsexuality for every 50,000 males and one case of female transsexuality for every 60,000 females.
In two cases (one per gender, 3.4% and 4.3%, respectively), temporary consumption of substances of abuse was found. No psychotic abnormalities were found. Fourteen cases (24.1% males and 30.4% females) presented reactive depression prior to reassignment, and in four cases (13.8%), involving males, the severity of the symptoms required treatment.
In all cases of female transsexuality (100%), and in the majority of male transsexuals (86.2%), the onset of the feeling was in childhood. In two cases it developed during adolescence (6.9%), and in another two cases (6.9%) homosexual tendencies developed in adolescence and subsequently went on to define the transsexual feeling.
The vast majority of cases who had sexual relationships did so from the heterosexual point of view. In some cases, there was a homosexual relationship at the start.
The age of initiation of legal proceedings was 32.39 years and was slightly higher in females. Gender reassignment surgery was carried out around the time of the legal application for gender reassignment. Classical surgical techniques were used in both directions: vaginoplasty and phalloplasty, although mastectomy and vaginectomy were performed with greater frequency, with many more transsexual males undergoing surgery than females.
Notwithstanding their different characteristics, these results are comparable with previous studies.
In the rare cases in which the forensic doctor may be required to issue a report, the following should be specified:
- a)
Presence of gender dysphoria.
- b)
Absence of lack of conformity with the sexual role, transvestism disorder, body dysmorphic disorder and psychotic disorder.
- c)
Exclusion of a personality disorder.
From a medical perspective, it has gone from a biologistic, deterministic, sexually dichotomous and heterosexist discourse (up to 2011) to another that incorporates the paradigm of sexual diversity,20 with the development of a more inclusive social and legal framework with gender fluidity.21
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Marote González RM, Pera Bajo FJ, Perea Pérez B, Sánchez Sánchez JA. Estudio de la transexualidad desde la Clínica Médico Forense de Madrid. Rev Esp Med Legal. 2018;44:150–157.
The study is based on the evaluation paper that Dr Marote defended when she was a Médico Interno Residente [Resident Medical Intern] (MIR) of Legal and Forensic Medicine at the Institut de Medicina Legal i Ciències Forenses de Catalunya [Institute of Legal Medicine and Forensic Sciences of Catalonia] (IMLCFC) in Barcelona.