



The statistical forms corresponding to deaths that require judicial and forensic interventions contain a very high number of ill-defined causes of death. The objective is to show the results of data recovery from the forensic autopsies and to analyse the impact of this information on the cause-of-death statistics for the year 2013 in Catalonia (Spain).
Material and methodsDeaths with judicial intervention with an ill-defined cause of death according to the WHO coding standards were selected from the Catalan Mortality Registry. Information was recovered from the autopsy registers of the Forensic Pathology centres of the Institute of Legal Medicine and Forensic Science of Catalonia (IMLCFC).
ResultsDeaths with judicial intervention represent 6% of total mortality in Catalonia, 42.9% due to external causes and 77% pertaining to ill-defined causes-of-death. There were 3,639 cases of death with judicial intervention, of which 43.4% (n=1,578) were reviewed, resulting in information that improved the cause of death in 78.4% of cases. The information retrieved increased accidental poisoning by 61.3%, suicides by 32.6%, homicides by 28.9%, falls by 27.4%, traffic accidents by 22.7% and ischaemic heart disease by 5.2%, with the equivalent increase in the mortality rates from these causes.
ConclusionsThe forensic autopsy information has a significant impact on cause-of-death statistics, especially external causes and ischaemic heart disease. A forensic report concerning the cause and circumstances of death, structured to facilitate further coding and the direct transmission of data to the statistical office, would be the best solution to prevent the loss of information currently experienced.
Los boletines estadísticos correspondientes a las defunciones que requieren intervención judicial (DIJ) y actuación forense contienen un número elevado de causas de muerte mal definidas. El objetivo es presentar los resultados de la recuperación de datos a partir de las autopsias judiciales del año 2013 en Cataluña y analizar el impacto de esta información sobre la estadística de causas de muerte.
Material y métodosSe seleccionaron del Registro de Mortalidad de Cataluña las defunciones con intervención judicial que tenían como causa de muerte unas determinadas afecciones mal definidas, según criterios de codificación de la OMS. Se recuperó la información de los registros de autopsia de los centros de Patología Forense del Instituto de Medicina Legal y Ciencias Forenses de Cataluña (IMLCFC).
ResultadosLas DIJ representan el 6% de la mortalidad total de Cataluña, el 42,9% de las causas externas y el 77% de las mal definidas. De los 3.639 casos de DIJ del año 2013 se revisó un 43,4% (n=1.578) y se obtuvo información que mejoró la causa de muerte del 78,4% de los revisados. La información recuperada aumentó un 61,3% las intoxicaciones accidentales, un 32,6% los suicidios, un 28,9% los homicidios, un 27,4% las caídas, un 22,7% los accidentes de tráfico y un 5,2% la cardiopatía isquémica, con el equivalente aumento de las tasas de mortalidad por estas causas.
ConclusionesLa información de las autopsias judiciales tiene un gran impacto en las estadísticas de causa de muerte, especialmente en las causas externas y la cardiopatía isquémica. Un informe forense sobre la causa y las circunstancias de la muerte, de manera que permita fácilmente su codificación posterior, así como la transmisión directa de estos datos a la oficina estadística serían la mejor solución para evitar la pérdida de información que se produce actualmente.
Mortality statistics play a major role in demographics, social studies and the healthcare administration. Basic indicators such as the gross or age-adjusted mortality rate and life expectancy allow us to determine the level of a population's health, and to situate it in time and compare it between territories.1 Studying the cause-of-death is fundamental in public health, as it furnishes knowledge about disease among the population and permits the re-allocation of healthcare resources within the context of service planning.2
Most causes of death are related to the diseases suffered by the population, barring a small percentage encompassed within so-called external or violent causes, which nevertheless enjoy major social relevance.
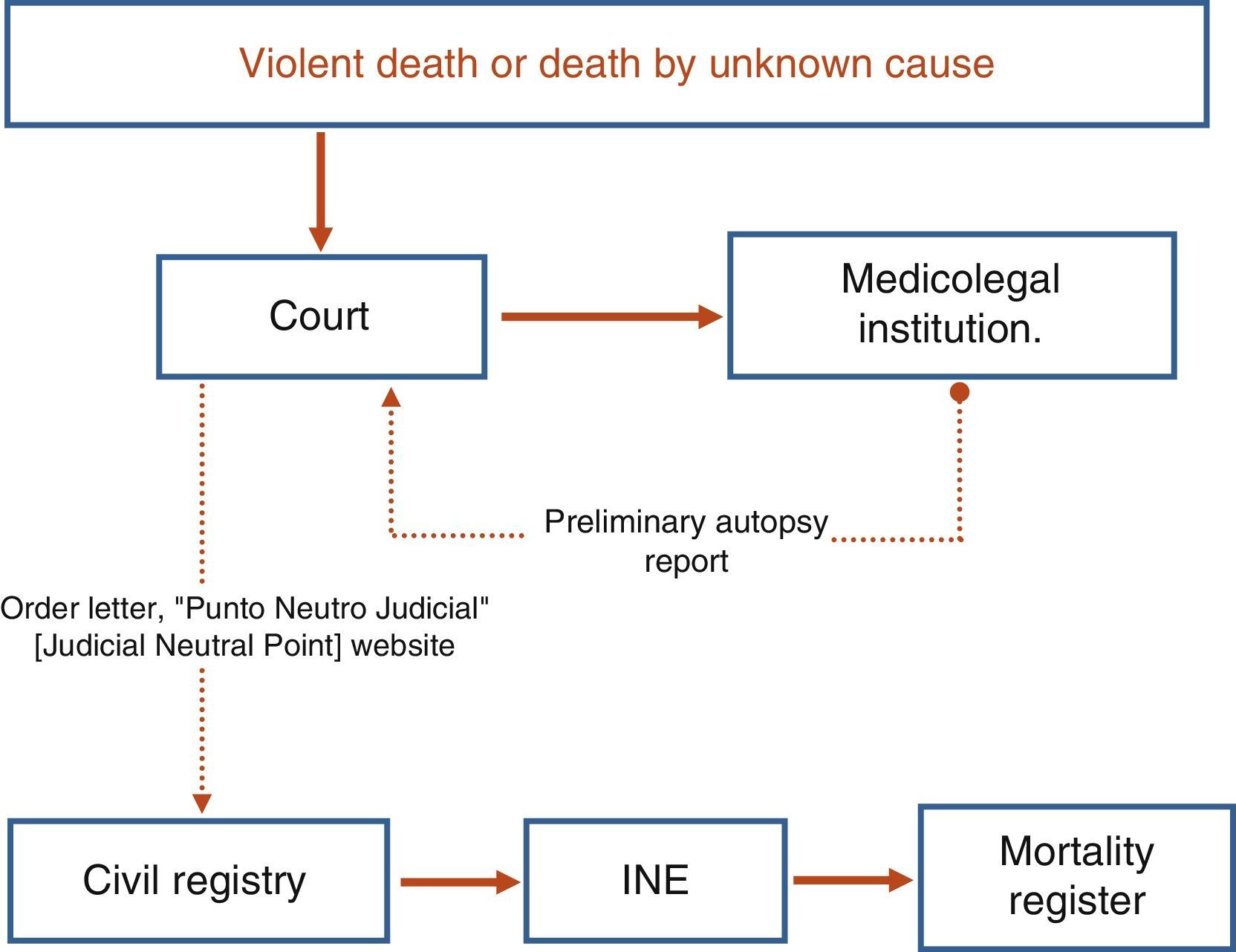
According to the Spanish legislation, when a death is suspected to be due to an external, violent or unknown cause, a forensic autopsy must be performed in order to determine the cause and circumstances of death. Based on the data from the preliminary forensic report, the lawyer from the justice administration is responsible for transcribing the causes of death onto the order letter that is sent to the Civil Registry to register the death. This is where the Judicial Statistical Death Register is completed (BEDJ).3 This Register, which is different to the one used for deaths that do not involve an inquest, contains the demographic data, cause and circumstances pertaining to the death and is sent to the Spanish National Statistics Institute (INE).4 The forensic autopsy is often accompanied by complementary tests (toxicology, histology, etc.), the results of which may take a few months and could potentially modify the causes of death issued on the preliminary report. As such, these results would not be reflected in the BEDJ.
The statistical information follows a parallel route to the judicial data,5 albeit with different times and the involvement of other institutions in the context of the territorial organisation of the statistics and health administrations. In the statistical circuit, the data from the BEDJ5 are processed without any subsequent updates following the final autopsy results. The deceased's demographic details are validated and the cause of death is coded in accordance with the standards established in the International Classification of Diseases (ICD-10)6 used in Spain since 1999.
Fig. 1 describes the process that these registers have followed since 2009, until they are converted into statistical data.

Numerous studies point to the complexity of the procedure and the flow of information as the cause behind the loss of quality and exhaustiveness of the data, in view of the time elapsed and the different agents involved,7,8 and confirm the scant validity of the data in some causes of death such as suicide and road accidents.9–11
In Catalonia, an increase in unreported causes of death was detected (cause left blank) in deaths with an inquest (DWI) from 2009, the year in which the new BEDJ was implemented and the information circuit changed, thus leading different measures to be taken. Since 2010, data from forensic autopsies regarding deaths in the city of Barcelona, which the Public Health Agency of Barcelona have been compiling since 1985,8 have been included in the Catalan Mortality Registry of the Department of Health. Moreover, this activity extended progressively to all DWIs in Catalonia as of 2011.12 This process has been made possible thanks to collaboration agreements between the Public Health Agency of Barcelona and the Department of Health, on the one hand, and between the administrations of Justice and Health of the Government of Catalonia, on the other.
This study presents the results retrieved from autopsy information corresponding to DWIs, whose causes of death reported in the BEDJ were ill-defined (see “Material and methods”), and analyses the impact of improving the basic cause of death on cause-of-death statistics. The purpose of this work is to illustrate the importance, for mortality statistics, of improving the DWI information circuits and forensic procedures.
Material and methodsThe data referred to herein have been taken from the BEDJ provided by the INE to the Department of Health for DWIs occurring in Catalonia in 2013. The deaths of residents of Catalonia that took place in other territories are not included.
DWIs from the Catalan Mortality Registry were identified using the registration number assigned by the INE and from the type of register variable, both of which allow for a distinction between registrations of these deaths and other deaths. Of this group, those in which the cause of death was included in Chapter xviii, on ill-defined diseases, according to the ICD-10 (revised codes: R00 to R99, except R95) were selected, with unspecific external causes (category X59), pulmonary oedema and cerebral oedema (categories J81 and G93) often used in the preliminary reports. For each of these deaths, information about cause of death was obtained from the autopsy register of all the divisions of the Institute of Legal Medicine and Forensic Sciences of Catalonia (IMLCFC). The autopsy register contains the identification variables and the cause of the preliminary autopsy report.
In order to evaluate the effect of this intervention on general mortality, the percentage change between the number of final causes and the number of initial causes was calculated, as was the proportion of retrieved causes regarding the total per final cause of death group. Both indicators are defined as follows:
Final cause: cause assigned to each DWI after the autopsy data have been included.
Initial cause: course assigned to each DWI in the BEDJ from the INE.
Retrieved cause: cause in which information from the autopsy has modified the initial cause.
ResultsIn 2013, 61,026 people died in Catalonia. Of these deaths, around 6% required an inquest. 3531 autopsies were performed at the IMLCFC, and there were 3639 registers with an inquest identifier (DWI).
Of the 3639 DWIs, 1578 cases (43.4%) were reviewed according to the defined criteria, from which information was obtained. 78.4% of the registers (n=1237) improved the coding of the initial cause, obtaining a cause that does not feature in Chapter xviii of ICD-10. Nevertheless, some of the cases reviewed did not involve an improvement, as in 341 cases (21.6% of those reviewed) the final code remained in the chapter of ill-defined diseases.
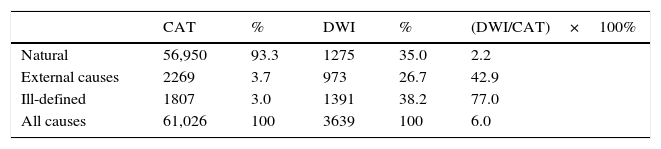
The weight these DWIs have on mortality in Catalonia in some causes of death prior to the retrieval of forensic information is included in Table 1. While DWIs only account for 6% of the total deaths occurring in Catalonia in 2013, they represent 43% of the external causes and more than three quarters of the ill-defined causes in the overall statistics.
Total deaths and deaths that require an inquest, by cause group, before the retrieval of forensic information, 2013.
| CAT | % | DWI | % | (DWI/CAT)×100% | |
|---|---|---|---|---|---|
| Natural | 56,950 | 93.3 | 1275 | 35.0 | 2.2 |
| External causes | 2269 | 3.7 | 973 | 26.7 | 42.9 |
| Ill-defined | 1807 | 3.0 | 1391 | 38.2 | 77.0 |
| All causes | 61,026 | 100 | 3639 | 100 | 6.0 |
CAT, Catalonia; DWI, deaths that require an inquest.
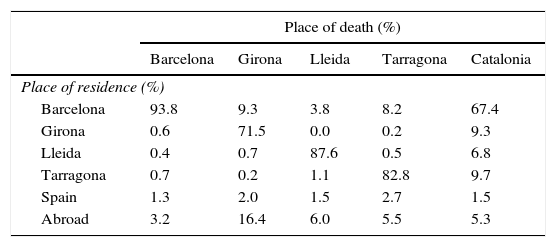
The distribution of the DWIs is presented in Table 2, according to the deceased's province of residence and the place where the death occurred. First of all, it should be noted that the proportion of deaths of people who are non-residents of Catalonia (foreigners and residents of other parts of Spain) is just over 6%, with the highest percentages in provinces with a significant influx of tourists, mainly Girona. The autopsies performed in the province of Barcelona correspond mainly to residents (93.8%). Residents of the province of Barcelona also account for a by no means negligible proportion of the cases occurring in the other provinces (7.6%).
Initial distribution of the 3639 deaths requiring an inquest, according to the place of death and residence, 2013.
| Place of death (%) | |||||
|---|---|---|---|---|---|
| Barcelona | Girona | Lleida | Tarragona | Catalonia | |
| Place of residence (%) | |||||
| Barcelona | 93.8 | 9.3 | 3.8 | 8.2 | 67.4 |
| Girona | 0.6 | 71.5 | 0.0 | 0.2 | 9.3 |
| Lleida | 0.4 | 0.7 | 87.6 | 0.5 | 6.8 |
| Tarragona | 0.7 | 0.2 | 1.1 | 82.8 | 9.7 |
| Spain | 1.3 | 2.0 | 1.5 | 2.7 | 1.5 |
| Abroad | 3.2 | 16.4 | 6.0 | 5.5 | 5.3 |
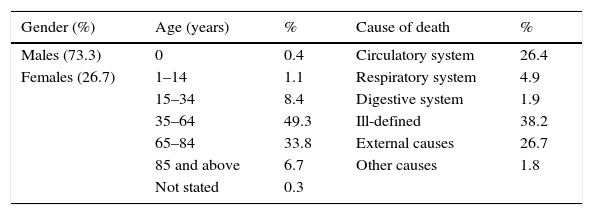
Table 3 presents the characteristics of the DWIs prior to the retrieval of information. Two thirds of the cases correspond to male deaths, and almost half are aged between 35 and 64 years, although there is a small proportion of unknown ages. According to the chapters of the ICD-10, the most frequent causes of death are those in the group of ill-defined diseases, followed by external causes and circulatory system diseases.
Initial distribution of the 3639 deaths requiring an inquest, according to gender, age and main causes of death, 2013.
| Gender (%) | Age (years) | % | Cause of death | % |
|---|---|---|---|---|
| Males (73.3) | 0 | 0.4 | Circulatory system | 26.4 |
| Females (26.7) | 1–14 | 1.1 | Respiratory system | 4.9 |
| 15–34 | 8.4 | Digestive system | 1.9 | |
| 35–64 | 49.3 | Ill-defined | 38.2 | |
| 65–84 | 33.8 | External causes | 26.7 | |
| 85 and above | 6.7 | Other causes | 1.8 | |
| Not stated | 0.3 |
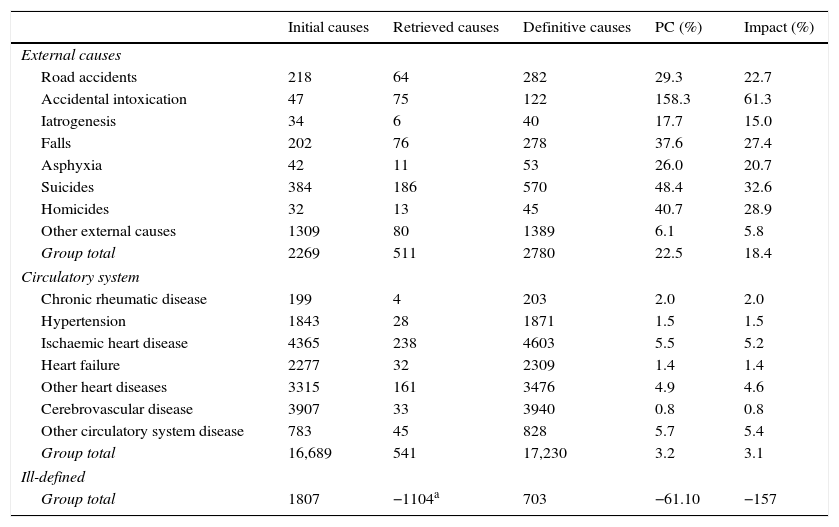
Table 4 shows the impact of retrieving forensic data on the causes of death with the greatest changes. The categories with a substantial percentage change (PC) following the retrieval of information are the ill-defined causes (PC: −61.1%), which diminish, whereas the number of cases in other groups increases, such as external causes (PC: 22.5%) and, to a lesser extent, circulatory system diseases (PC: 3.2%) and ischaemic heart disease (PC: 5.5%). The final impact on statistics is significant, mainly in the group of ill-defined causes (−157%), and other groups increase as a result, such as the external causes, in which 18.4% of the final cases are so thanks to the information retrieved. The most specific causes in the external causes group are those that present a greater percentage change and impact on the overall statistics, such as accidental intoxications, suicides, accidental falls and road accidents.
Result of the retrieval of causes and impact on mortality statistics by group of causes of death selected, 2013.
| Initial causes | Retrieved causes | Definitive causes | PC (%) | Impact (%) | |
|---|---|---|---|---|---|
| External causes | |||||
| Road accidents | 218 | 64 | 282 | 29.3 | 22.7 |
| Accidental intoxication | 47 | 75 | 122 | 158.3 | 61.3 |
| Iatrogenesis | 34 | 6 | 40 | 17.7 | 15.0 |
| Falls | 202 | 76 | 278 | 37.6 | 27.4 |
| Asphyxia | 42 | 11 | 53 | 26.0 | 20.7 |
| Suicides | 384 | 186 | 570 | 48.4 | 32.6 |
| Homicides | 32 | 13 | 45 | 40.7 | 28.9 |
| Other external causes | 1309 | 80 | 1389 | 6.1 | 5.8 |
| Group total | 2269 | 511 | 2780 | 22.5 | 18.4 |
| Circulatory system | |||||
| Chronic rheumatic disease | 199 | 4 | 203 | 2.0 | 2.0 |
| Hypertension | 1843 | 28 | 1871 | 1.5 | 1.5 |
| Ischaemic heart disease | 4365 | 238 | 4603 | 5.5 | 5.2 |
| Heart failure | 2277 | 32 | 2309 | 1.4 | 1.4 |
| Other heart diseases | 3315 | 161 | 3476 | 4.9 | 4.6 |
| Cerebrovascular disease | 3907 | 33 | 3940 | 0.8 | 0.8 |
| Other circulatory system disease | 783 | 45 | 828 | 5.7 | 5.4 |
| Group total | 16,689 | 541 | 17,230 | 3.2 | 3.1 |
| Ill-defined | |||||
| Group total | 1807 | −1104a | 703 | −61.10 | −157 |
Impact: proportion of retrieved causes regarding the total per cause group; PC: percentage change.
This article presents a description of the deaths that undergo an inquest and forensic intervention in Catalonia, as well as their impact on mortality statistics. Of all the deaths occurring annually, only a small number require a forensic intervention. However, an analysis of the specific causes reveals the importance of this information. The discrepancy observed in the number of autopsies performed and the number of DWIs could be the result of cases of natural death in which the coroner issues the death certificate as a doctor from the Civil Registry, without the autopsy being mandatory, since, irrespective of the type of forensic intervention, these deaths are reported in the BEDJ.
Of these results, it should be noted that the number of deaths occurring outside the place of residence is by no means negligible. Since the municipality where the death occurs determines where the autopsy will be performed, this discordance could entail a further loss of information due to the lack of access to related persons, personal circumstances and the data contained in the deceased's medical history, which could prove useful to the work undertaken by the Forensic Pathology Service.
The results obtained through the retrieval of information directly from the medical-forensic source are very satisfactory, since they permit a huge reduction in the number of ill-defined causes in the overall statistics. In turn, they provide information on very sensitive causes that are traditionally regarded as somewhat unreliable in mortality statistics, such as intoxications, suicides, traffic accidents and homicide.7,13,14 They also bring a relatively unknown aspect to light, namely under-reporting, which may affect ischaemic heart disease statistics; receiving this information could prove useful in estimating the incidence thereof.15,16
The impact of forensic information on official mortality statistics has also been a regular international concern.17–21 Thus, in Finnish statistics, the greater impact of retrieving forensic information leads to a reduction in ill-defined causes and an improvement in endocrine system causes, with barely any modification on the unnatural causes.17 There is also a certain degree of improvement in undefined tumours and circulatory system diseases, and more particularly in ischaemic heart disease, albeit to a lesser extent than that observed in this study.18,22,23 Those that analyse external causes detect significant under-reporting of these causes in localised areas19 and a substantial reduction in unspecified accidents to the benefit of road accidents, falls, homicides and suicides, in this order.18
A more recent study analyses the information source and procedure used in England and Wales to report the cause of death to statistics (coroner's short form vs narrative verdicts) and their impact on deaths arising due to accidents and external causes.21 Although it does not find a significant effect on statistics, mainly with regard to suicide, it does note the importance of the coroner producing better-structured information so as to facilitate the coding of the cause of death by the statistics offices and thus improve quality standards.
In Spain, different works have demonstrated the under-reporting and/or lack of validity in the mortality statistics for different causes of death in the DWIs.9,22,23 There may be numerous reasons for this, although one fundamental cause identified is the complexity of the information circuit from the place in which the events occur up to the point where the data are transcribed on the statistical document. It has also been attributed to the time lapse between the performance of the autopsy and the definitive findings, and the lag that this implies on the process of declaring the death to statistics, which is linked to recording the death in the Civil Registry a few hours after death.24
In addition, while the main function of coroners is to report to the administration of justice, like other authors,7 we highlight the importance of autopsy information as a source of information in mortality statistics. The results of this work are a clear example of the impact that their daily work can have on the field of health. Forensic experience suggests the convenience of including the cause derived from the final autopsy finding in the statistical information. This objective is difficult to accomplish, since national and international statistics institutions undertake a commitment to provide mortality data within a very short timeframe after death, but this will have to be repeated at least for the specific studies of concrete causes.
In all the developed countries, cause-of-death statistics are useful for establishing and evaluating healthcare policies,25 which justifies the demand that they be reliable. For example, death by acute myocardial infarction has fallen by a yearly average of 4.4% in Spain,26 with a marked downward trend in Catalonia,26 and has been included as one of the objectives of the Health Plan.2 Important variations, such as the ones observed here, due to the information production process, could distort the evolution of mortality for this cause of death and even the accomplishment of healthcare objectives.
The same thing occurs with other public intervention policies on aspects with a broad social impact, such as accidents or suicides. In Catalonia, the evolution of the suicide rate in the last 20 years was initially stable or downward-tapering, although more recently it has presented a sustained increase.1 This increase partially coincides in time with the forensic information retrieval work undertaken by the Department of Health in order to improve statistics.12 Although we do not have access to validation studies on this cause for the entire region, recent work carried out in the province of Tarragona does not confirm this upward trend, although it does reveal a mean under-reporting of 16%, with a very erratic evolution, with some very poorly-reported years (20% losses) and other less poorly-reported ones (2% losses).26
The study's limitations include the fact that it only describes the results for a single year and that there could be differences in the information retrieved on the one hand due to the improvement intervention and, on the other, to organisational changes in the IMLCFC.
In summary, in view of the relevance of the data provided by forensic procedures to the healthcare sector overall, the information noted on the preliminary autopsy results must be clear and explanatory, underlining the circumstances of death, if external causes are involved, in order to subsequently permit coding by means of the ICD, which includes a large number of codes for reference purposes. It would also be desirable to ensure that coroners relay the information about the cause and circumstances of death directly to the statistics office performing the coding, in order to avoid transcriptions between the different documents by personnel without medical training. In the first instance, the result of the preliminary autopsy, and preferably the final information too, provided that this is feasible and that the delays are acceptable.
ConclusionDeaths that require an inquest or forensic autopsy represent a small proportion of the deaths that occur annually; however, they account for half of the external causes and around three quarters of the ill-defined causes in overall mortality statistics.
The retrieval of forensic information for deaths with an ill-defined cause has a very significant impact on mortality statistics, since other categories, such as external causes (intoxications, suicides, road accidents, homicides) and ischaemic heart disease, increase the mortality rate.
The clear and direct transmission of forensic information to the statistics office about the cause and circumstances of death appears to be the best solution, in order to facilitate coding.
Conflicts of interestWe declare that we have no conflicts of interest.
Thank you to the professionals of the Catalan Mortality Register and the Public Health Agency of Barcelona who helped to gather, code and prepare the data, and to the coroners and members of the Institute of Legal Medicine and Forensic Sciences of Catalonia, who carry out and maintain the information sources regarding autopsies.
Please cite this article as: Puigdefàbregas Serra A, Freitas Ramírez A, Gispert Magarolas R, Castellà Garcia J, Vidal Gutiérrez C, Medallo Muñiz J, et al. Las muertes con intervención judicial y medicolegal y su impacto en la estadística de causas de muerte en Cataluña. Rev Esp Med Legal. 2017;43:13–19.