



The loss of chance is a legal concept that has gained ground in recent years as a decisive criterion for the assessment of healthcare-related bodily harm. In this paper, we analyse the convictions issued by the contentious-administrative jurisdiction (public medicine), in cases in which, due to a lack of diligence by the professional, the patient lost the possibility of a diagnosis or adequate treatment.
Material and methodsWe selected the sentences related to Spanish public medicine, which referred to the concept of loss of chance that were issued until May 2014.
ResultsOf the 519 analysed sentences, 340 (66.5%) were due to misdiagnosis and 138 (26.6%) due to inadequate treatment. Since 2010, 351 (67.6%) sentences were passed, representing more than a 100% increase compared to 168 (32.4%) in the first 8 years of the study (2002–2009). Most patients were male (56.1%) who died (57.4%), and the conditions that most frequently led to the conviction were malignant cancer (26.4%) and neurological disorders (17.3%).
ConclusionsThe litigation due to loss of chance in Spanish public health has significantly increased over the last few years. The convictions were mainly issued because of diagnostic error or inadequate treatment.
La pérdida de oportunidad asistencial es un concepto jurídico que se ha abierto paso en los últimos años como un criterio determinante para la valoración del daño corporal derivado de la asistencia sanitaria. En este trabajo analizamos las sentencias condenatorias dictadas por la Jurisdicción Contencioso Administrativa, en el ámbito de la medicina pública española, en los supuestos en los que, por falta de diligencia del profesional, el paciente ha perdido la posibilidad de un diagnóstico o un tratamiento adecuado.
Material y métodosSe han seleccionado las sentencias judiciales, relacionadas con la medicina pública española, que hacían referencia al concepto de pérdida de oportunidad asistencial y que fueron dictadas hasta mayo del 2014.
ResultadosDe las 519 sentencias analizadas, 340 (66,5%) fueron dictadas por error diagnóstico y 138 (26,6%) por tratamiento inadecuado. Desde el año 2010 se produjeron 351 (67,6%) sentencias, lo que supuso más del 100% de aumento con respecto a las 168 (32,4%) ocurridas en los primeros 8 años del estudio (2002 a 2009). La mayoría de los pacientes fueron varones (56,1%), que fallecieron (57,4%), siendo las patologías que más frecuentemente originaron la condena, la oncológica maligna (26,4%) y la neurológica (17,3%).
ConclusionesLa actividad litigante por pérdida de oportunidad asistencial en la medicina pública española ha aumentado significativamente estos últimos años. Las condenas fueron dictadas fundamentalmente por error diagnóstico y tratamiento inadecuado.
In healthcare, the loss of chance concept emerged with a view to offer a legal solution to cases in which, through the omission of due diligence, the patient was denied the possibility of being cured.1–3 Saigí Ullastre et al.4 define the loss of chance concept as cases which present, as a common characteristic, an error or delay in the diagnosis of a medical process that ends in the injury or death of the patient. From the standpoint of medical responsibility, an omission refers to a specific action; the action that could be expected of the physician who had the obligation to act, or rather, to act in a given way, i.e. pursuant to lex artis.3 In these cases, the omission generates uncertainty as to what would have happened had the behaviour in question been replaced by the appropriate action, which is why it is unknown if the end result occurred in all certainty due to the medical professional's omission.1–3 We do not know if the injury to the patient would have occurred in the same way if the appropriate action had been taken.1–3
In effect, we are dealing with complex cases regarding proof of the causal relationship, in which we cannot know or substantiate what might have happened had the perpetrator of such behaviour acted appropriately.1–3 To that end, we need to know whether, on mentally adding the omitted behaviour, the damage would have occurred in the same way.3
This article seeks to ascertain the characteristics of the rulings issued due to loss of chance in Spanish public health, taking into account all of the variables that may have an influence, both with regard to the way the claim is handled and in the resolution of the legal process. In this sense, the results could facilitate safer medical practice for both the patient and professional, and could help to establish criteria that provide some degree of foreseeability as regards possible judicial claims arising due to loss of chance. Finally, it should be noted that there is no similar study in the medical or legal literature that makes specific reference to the loss of chance in medicine.
MethodsOrigin of the material and inclusion criteriaFirst of all, it should be clarified that the Spanish jurisdictional hierarchy is established by its procedural function.1 Thus, we can distinguish, on the one hand, between bodies of first instance, which resolve matters initially, and, on the other, bodies of second instance, which are used to review the former; in other words, an new and full indictment before a superior body that is stratified in the following way in the contentious-administrative channel: High Court of Law (superior body in the autonomous community with powers to judge pecuniary liability following the transfer of competences from the State to the autonomous communities), the National Audience (which still has powers as regards matters of pecuniary liability derived from healthcare in competences that have not been transferred to the autonomous communities, such as those exercised by the Ministry of Health, Social Services and Equality, or in exclusive State competences, such as those held by the Ministry of Defence) and finally, the Supreme Court (the highest jurisdictional body). The contentious-administrative complaint channel is a complex system of competences provided for by Law 29/1998, of 13 July, regulating Contentious-Administrative Jurisdiction, in which, depending on the territorial scope, in the first instance the procedure is executed by the Contentious-Administrative courts or directly by the High Court of the autonomous community, with no need to go to the Contentious-Administrative courts first.
We have analysed all judicial sentences issued in Spain related to medical, surgical and obstetric conditions, in the sphere of the Contentious-Administrative Jurisdiction, which make reference to the loss of chance concept, up until May 2014. The search was performed in May, 2014, using the legal database of the El Derecho publishing house (http://www.elderecho.com/), due to currently being considered one of the most powerful and most used databases in the academic and professional sphere by lawyers, judges and magistrates.
Said database included the administrative, judicial and clinical variables of each sentence. However, the “type of professional involved” variable could not be gathered since most of the sentences, which were issued in the contentious-administrative sphere, did not specify which doctor (specialist or not) had been involved. The route of access (search engine) was as follows: pecuniary liability/healthcare/loss of chance/conviction.
Statistical analysisA simple descriptive study was performed on the variables gathered by means of percentages. As regards the autonomous communities, and with a view to correct the number of sentences related to the medical activity performed, the number of public hospital beds is presented according to data from the Ministry of Health, Social Services and Equality, as on 31 December 2014 (http://www.msssi.gob.es/ciudadanos/prestaciones/centrosServiciosSNS/hospitales/docs/CNH2015.pdf). This yielded the index of sentences for every 100,000 hospital beds. In the sets of two variables whose distribution could be related and where this relationship could be of interest, a comparison of variables was performed by means of contingency tables using the Chi-square test or Fisher's exact test. The Wilcoxon signed-rank test was used to compare the amount of compensation awarded to the amount claimed. Statistical significance was established for a p value of <0.05 and the data were analysed by means of the SPSS, v. 21.0 statistics program.
ResultsOf the 10,001 sentences obtained, 1249 alluded to the loss of chance concept. Of these, 522 were convictions in the sphere of public medicine. However, we decided to exclude three of them because the condition or sequelae that prompted the claim were not specified. These convictions were issued between 16 October 2002 and 14 May 2014.
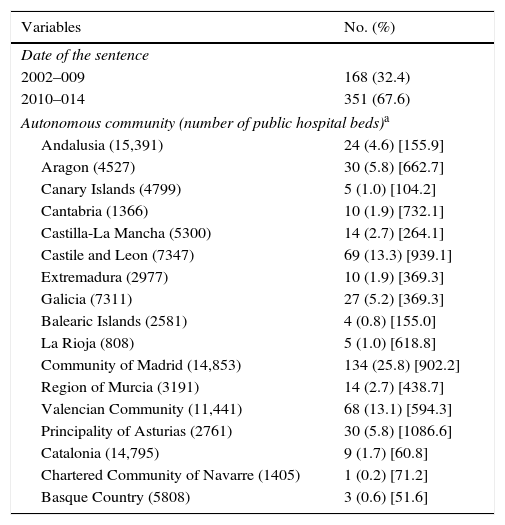
In our sample, the first sentence due to loss of chance in Spain, within the sphere of public medicine (failure to detect a phocomelia during a prenatal ultrasound), was issued on 16 October 2002 by the National Audience. Since then, there has been exponential growth in this type of sentence (Table 1). Thus, since 2010 there have been 351 (67.6%) sentences. This amounts to an increase of more than 100% with respect to the 168 (32.4%) sentences issued in the first 8 years of the study (2002–2009). Of the 17 autonomous communities, Castile and Leon and Valencia were, in absolute terms, the ones with the most convictions for loss of chance; however, following the “correction” concerning the number of beds, the index of sentences per 100,000 hospital beds was highest in the Principality of Asturias and in Castile and Leon (Table 1).
Administrative variables.
| Variables | No. (%) |
|---|---|
| Date of the sentence | |
| 2002–009 | 168 (32.4) |
| 2010–014 | 351 (67.6) |
| Autonomous community (number of public hospital beds)a | |
| Andalusia (15,391) | 24 (4.6) [155.9] |
| Aragon (4527) | 30 (5.8) [662.7] |
| Canary Islands (4799) | 5 (1.0) [104.2] |
| Cantabria (1366) | 10 (1.9) [732.1] |
| Castilla-La Mancha (5300) | 14 (2.7) [264.1] |
| Castile and Leon (7347) | 69 (13.3) [939.1] |
| Extremadura (2977) | 10 (1.9) [369.3] |
| Galicia (7311) | 27 (5.2) [369.3] |
| Balearic Islands (2581) | 4 (0.8) [155.0] |
| La Rioja (808) | 5 (1.0) [618.8] |
| Community of Madrid (14,853) | 134 (25.8) [902.2] |
| Region of Murcia (3191) | 14 (2.7) [438.7] |
| Valencian Community (11,441) | 68 (13.1) [594.3] |
| Principality of Asturias (2761) | 30 (5.8) [1086.6] |
| Catalonia (14,795) | 9 (1.7) [60.8] |
| Chartered Community of Navarre (1405) | 1 (0.2) [71.2] |
| Basque Country (5808) | 3 (0.6) [51.6] |
Data submitted as No. (%) [index of sentences/100,000 hospital beds].
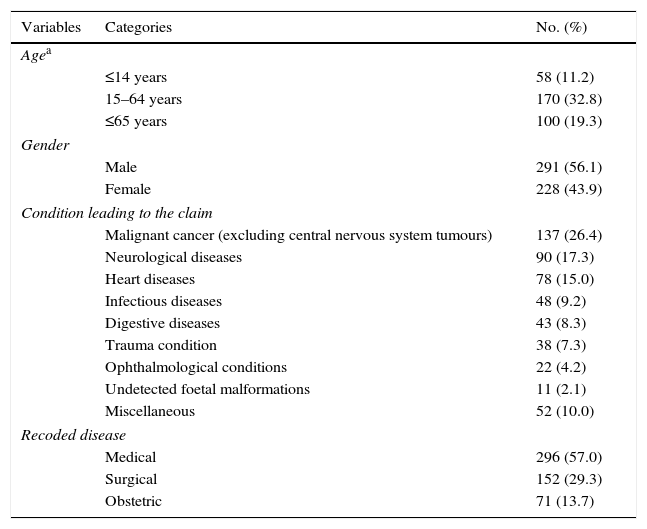
Table 2 presents the clinical variables. Most of the patients were male (56.1%), and the conditions that most frequently led to a conviction were malignant cancer (26.4%) and neurological disease (17.3%).
Clinical variables.
| Variables | Categories | No. (%) |
|---|---|---|
| Agea | ||
| ≤14 years | 58 (11.2) | |
| 15–64 years | 170 (32.8) | |
| ≤65 years | 100 (19.3) | |
| Gender | ||
| Male | 291 (56.1) | |
| Female | 228 (43.9) | |
| Condition leading to the claim | ||
| Malignant cancer (excluding central nervous system tumours) | 137 (26.4) | |
| Neurological diseases | 90 (17.3) | |
| Heart diseases | 78 (15.0) | |
| Infectious diseases | 48 (9.2) | |
| Digestive diseases | 43 (8.3) | |
| Trauma condition | 38 (7.3) | |
| Ophthalmological conditions | 22 (4.2) | |
| Undetected foetal malformations | 11 (2.1) | |
| Miscellaneous | 52 (10.0) | |
| Recoded disease | ||
| Medical | 296 (57.0) | |
| Surgical | 152 (29.3) | |
| Obstetric | 71 (13.7) | |
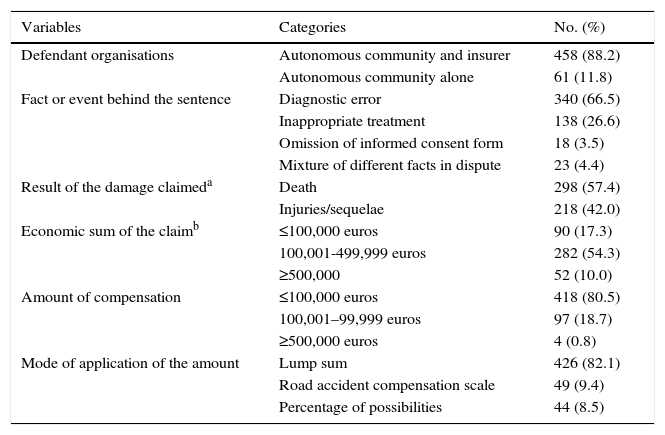
Table 3 presents the judicial variables. Most of the convictions were imposed upon the autonomous community and their insurer (insurance company) (88.2%). Of the 519 sentences, 340 (66.5%) were issued on account of a diagnostic error (either through failure to request a specific test or a deficient examination), 138 (26.6%) for the omission of a suitable treatment and just 18 (3.5%) for the omission of information. 57.4% of the patients died. It should be noted that the distribution of the amount initially claimed is lower than that of the compensation that was eventually awarded. While most of the claims are for amounts between 100,000 and 499,999 euros (54.3%), the results show that, for the most part (80.5%), the compensation awarded was ≤100,000 euros. Generally speaking, the amount awarded (median=50,000 euros) was less than the sum claimed (median=180,301.50 euros) (Wilcoxon signed rank test, p<0.001). Moreover, we found no statistically significant differences (Mann–Whitney U, p=0.09) between the compensation awarded in the first period of the study (2004–2009) (median=60,000 euros) and that of the second period (2010–2014) (median=40,000 euros). The largest amount (almost one million euros) was issued in the case of a male patient of unspecified age who had suffered a stroke and in whom there had been a diagnostic error. Finally, it is highly relevant that the road accident compensation scale is only applied by analogy or similar reasoning in 9.4% of cases, that in 8.5% compensation is provided according to the hypothetical percentage of being cured (percentage applied to the aforementioned scale) and that in most cases (82.1%) a lump sum is awarded, i.e. without considering the scale or defined criteria (Table 3).
Judicial variables.
| Variables | Categories | No. (%) |
|---|---|---|
| Defendant organisations | Autonomous community and insurer | 458 (88.2) |
| Autonomous community alone | 61 (11.8) | |
| Fact or event behind the sentence | Diagnostic error | 340 (66.5) |
| Inappropriate treatment | 138 (26.6) | |
| Omission of informed consent form | 18 (3.5) | |
| Mixture of different facts in dispute | 23 (4.4) | |
| Result of the damage claimeda | Death | 298 (57.4) |
| Injuries/sequelae | 218 (42.0) | |
| Economic sum of the claimb | ≤100,000 euros | 90 (17.3) |
| 100,001-499,999 euros | 282 (54.3) | |
| ≥500,000 | 52 (10.0) | |
| Amount of compensation | ≤100,000 euros | 418 (80.5) |
| 100,001–99,999 euros | 97 (18.7) | |
| ≥500,000 euros | 4 (0.8) | |
| Mode of application of the amount | Lump sum | 426 (82.1) |
| Road accident compensation scale | 49 (9.4) | |
| Percentage of possibilities | 44 (8.5) |
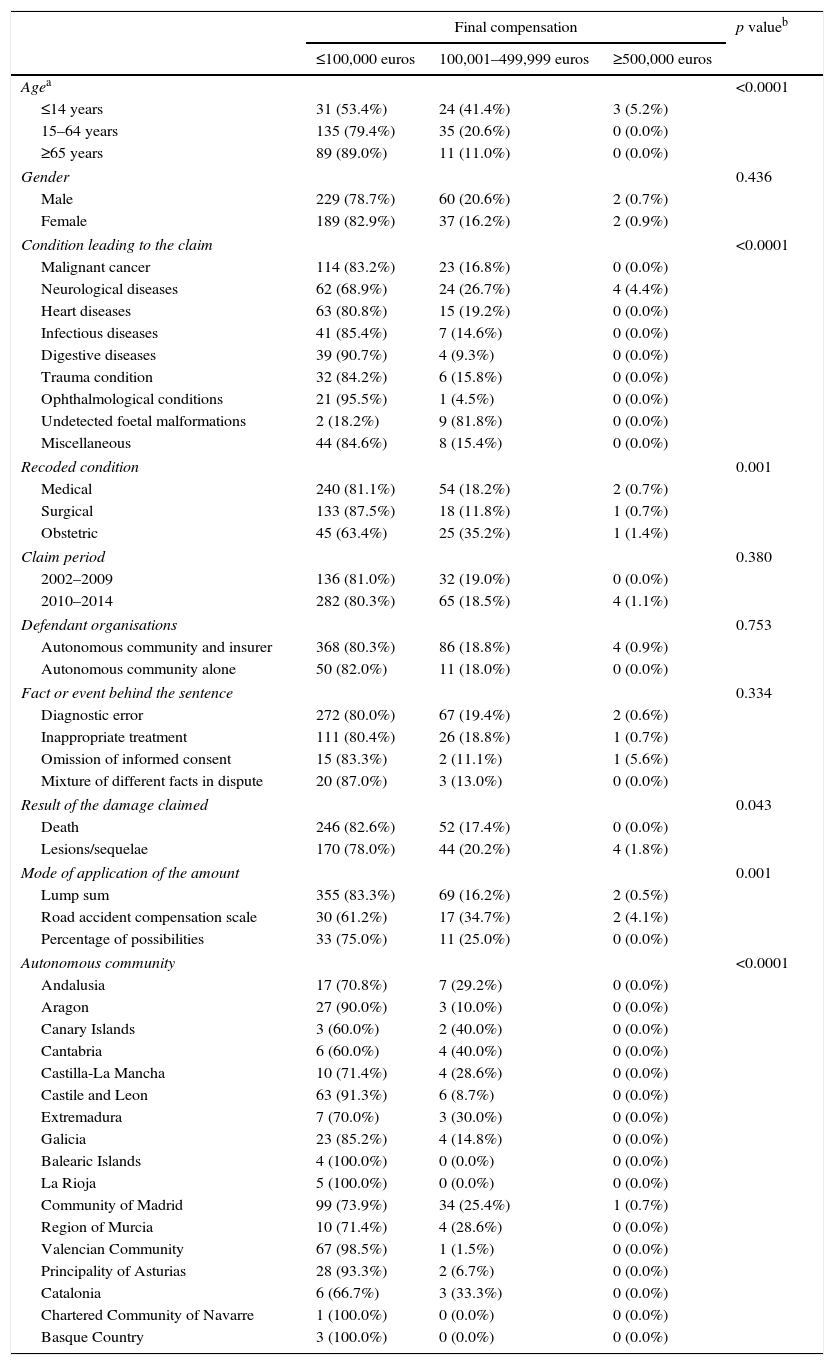
Table 4 shows that the higher compensation amounts (≥500,000 euros) were awarded to paediatric patients and in cases of undetected foetal malformations. With regard to the importance of obstetric conditions, some work has already been done in Spain with regard to the loss of chance.5 Similarly, when the conditions were recoded as medical, surgical and obstetric, the latter received the greatest compensation in proportional terms (Table 4). Sequelae or oral lesions received proportionally more compensation than deaths (Table 4). Finally, the highest compensation amounts were awarded in the autonomous communities of the Canary Islands and Cantabria (Table 4).
Breakdown of the final compensation in accordance with the clinical, administrative and judicial variables.
| Final compensation | p valueb | |||
|---|---|---|---|---|
| ≤100,000 euros | 100,001–499,999 euros | ≥500,000 euros | ||
| Agea | <0.0001 | |||
| ≤14 years | 31 (53.4%) | 24 (41.4%) | 3 (5.2%) | |
| 15–64 years | 135 (79.4%) | 35 (20.6%) | 0 (0.0%) | |
| ≥65 years | 89 (89.0%) | 11 (11.0%) | 0 (0.0%) | |
| Gender | 0.436 | |||
| Male | 229 (78.7%) | 60 (20.6%) | 2 (0.7%) | |
| Female | 189 (82.9%) | 37 (16.2%) | 2 (0.9%) | |
| Condition leading to the claim | <0.0001 | |||
| Malignant cancer | 114 (83.2%) | 23 (16.8%) | 0 (0.0%) | |
| Neurological diseases | 62 (68.9%) | 24 (26.7%) | 4 (4.4%) | |
| Heart diseases | 63 (80.8%) | 15 (19.2%) | 0 (0.0%) | |
| Infectious diseases | 41 (85.4%) | 7 (14.6%) | 0 (0.0%) | |
| Digestive diseases | 39 (90.7%) | 4 (9.3%) | 0 (0.0%) | |
| Trauma condition | 32 (84.2%) | 6 (15.8%) | 0 (0.0%) | |
| Ophthalmological conditions | 21 (95.5%) | 1 (4.5%) | 0 (0.0%) | |
| Undetected foetal malformations | 2 (18.2%) | 9 (81.8%) | 0 (0.0%) | |
| Miscellaneous | 44 (84.6%) | 8 (15.4%) | 0 (0.0%) | |
| Recoded condition | 0.001 | |||
| Medical | 240 (81.1%) | 54 (18.2%) | 2 (0.7%) | |
| Surgical | 133 (87.5%) | 18 (11.8%) | 1 (0.7%) | |
| Obstetric | 45 (63.4%) | 25 (35.2%) | 1 (1.4%) | |
| Claim period | 0.380 | |||
| 2002–2009 | 136 (81.0%) | 32 (19.0%) | 0 (0.0%) | |
| 2010–2014 | 282 (80.3%) | 65 (18.5%) | 4 (1.1%) | |
| Defendant organisations | 0.753 | |||
| Autonomous community and insurer | 368 (80.3%) | 86 (18.8%) | 4 (0.9%) | |
| Autonomous community alone | 50 (82.0%) | 11 (18.0%) | 0 (0.0%) | |
| Fact or event behind the sentence | 0.334 | |||
| Diagnostic error | 272 (80.0%) | 67 (19.4%) | 2 (0.6%) | |
| Inappropriate treatment | 111 (80.4%) | 26 (18.8%) | 1 (0.7%) | |
| Omission of informed consent | 15 (83.3%) | 2 (11.1%) | 1 (5.6%) | |
| Mixture of different facts in dispute | 20 (87.0%) | 3 (13.0%) | 0 (0.0%) | |
| Result of the damage claimed | 0.043 | |||
| Death | 246 (82.6%) | 52 (17.4%) | 0 (0.0%) | |
| Lesions/sequelae | 170 (78.0%) | 44 (20.2%) | 4 (1.8%) | |
| Mode of application of the amount | 0.001 | |||
| Lump sum | 355 (83.3%) | 69 (16.2%) | 2 (0.5%) | |
| Road accident compensation scale | 30 (61.2%) | 17 (34.7%) | 2 (4.1%) | |
| Percentage of possibilities | 33 (75.0%) | 11 (25.0%) | 0 (0.0%) | |
| Autonomous community | <0.0001 | |||
| Andalusia | 17 (70.8%) | 7 (29.2%) | 0 (0.0%) | |
| Aragon | 27 (90.0%) | 3 (10.0%) | 0 (0.0%) | |
| Canary Islands | 3 (60.0%) | 2 (40.0%) | 0 (0.0%) | |
| Cantabria | 6 (60.0%) | 4 (40.0%) | 0 (0.0%) | |
| Castilla-La Mancha | 10 (71.4%) | 4 (28.6%) | 0 (0.0%) | |
| Castile and Leon | 63 (91.3%) | 6 (8.7%) | 0 (0.0%) | |
| Extremadura | 7 (70.0%) | 3 (30.0%) | 0 (0.0%) | |
| Galicia | 23 (85.2%) | 4 (14.8%) | 0 (0.0%) | |
| Balearic Islands | 4 (100.0%) | 0 (0.0%) | 0 (0.0%) | |
| La Rioja | 5 (100.0%) | 0 (0.0%) | 0 (0.0%) | |
| Community of Madrid | 99 (73.9%) | 34 (25.4%) | 1 (0.7%) | |
| Region of Murcia | 10 (71.4%) | 4 (28.6%) | 0 (0.0%) | |
| Valencian Community | 67 (98.5%) | 1 (1.5%) | 0 (0.0%) | |
| Principality of Asturias | 28 (93.3%) | 2 (6.7%) | 0 (0.0%) | |
| Catalonia | 6 (66.7%) | 3 (33.3%) | 0 (0.0%) | |
| Chartered Community of Navarre | 1 (100.0%) | 0 (0.0%) | 0 (0.0%) | |
| Basque Country | 3 (100.0%) | 0 (0.0%) | 0 (0.0%) | |
Our research was based on examining sentences issued in cases of the pecuniary liability of the public administration. In this way, we ruled out all the resolutions from the civil and penal jurisdictions in order to prevent our results from becoming “contaminated”, given that the indictment criteria are different depending on the jurisdiction judging the medical acts. Most of the Spanish work conducted does not distinguish between the three types of jurisdictions (civil, penal and administrative), thus making it difficult to compare the results thereof to this study.6–11
Descriptions of the sentences issued due to loss of chance in Spanish public medicine over 12 years mainly show that these have increased by more than 100% in the last few years. The loss of chance theory was vigorously introduced into the jurisprudential doctrine for judging the conduct of medical professionals in 2002. As such, we may conclude that, while the theory has only been in use for a few years, it has become more widespread over time.
Our data reveal several different issues that must be highlighted: The communities do not apply the loss of chance theory with the same frequency; compensation amounts also vary depending on the geographical area; malignant cancer and neurological disease led to the highest number of convictions, and finally, diagnostic error was the most common cause of conviction.
The results show that, while they did not issued the most sentences, proportionally the Principality of Asturias and Castile and Leon are the autonomous communities that have applied loss of chance on the most occasions, although in reality the effect thereof is spreading vigorously across Spain, with Madrid and Valencia also taking on greater prominence.
With regard to the amount of compensation, in most cases (80.5%) this was equal to or below 100,000 euros, despite the fact that the most common reason behind the claims was death derived from a diagnostic error or inadequate treatment. This points to a discrepancy with the amount claimed, which was only equal to or below 100,000 euros in 17.3% of the cases. There is an explanation for these results. When a doctor fails to apply a treatment–for example, in the case of a properly diagnosed acute myocardial infection with ST-segment elevation, where the physician fails to indicate rapid mechanical restoration of blood flow by means of a stent–and the patient dies or suffers crippling sequelae, we will never know if the same outcome would have occurred had the appropriate treatment been applied in time. In such an eventuality, nobody could say whether or not the patient would have survived without sequelae. For this reason, the jurisprudential doctrine faces enormous difficulties when assessing liability and, where applicable, in determining the amount of compensation warranted by the resulting damage. Logically, since we can only talk at most about a hypothetical causality, we can see that the convictions significantly reduce the amount claimed because the judges do not seem to want to hold the physician liable for all of the damages. There is no consensus in the jurisprudence that solves this debate, although it must be highlighted that in 426 cases (82.1%), the compensation awarded was a lump sum to cover moral damages, and the specific criterion applied was not known, which also gave rise to a reduction in the compensation versus the amount claimed, as is established in the accident scale. In 49 cases (9.4%), the damages were compensated in full through the application of the scale established to assess personal injuries in road accidents, due to the lack of a scale for healthcare injuries, and in 44 cases (8.5%) the compensation was reduced taking into account the percentage of possibilities that the damage would not have occurred had due diligence been applied.
The first criterion is precisely the one followed by Section 10 of the High Court of Madrid, which has regularly issued the amount of 12,000–18,000 euros by way of compensation in cases where the patient died. See, among the many other sentences issued under this Section and Chamber, the one dated 13/09/2012, no. 605/2012, which awarded the sum of 18,000 euros as compensation following the death of a cancer patient; the sentence dated 07/02/2013, no. 119/2013, which paid out 12,000 as compensation for death; and the one from 03/10/2012, no. 647/2012, granting 8000 euros for the death of a patient with oesophageal cancer.
In the second criterion, the resolutions provide full compensation for the damages, with no percentage reduction, either because the Court deems that it is not appropriate to appraise conjectures or because it considers that the liability should fall upon the person who failed to fulfil their objective duty of care and gave rise to the risk.
In the third criterion, a rule of proportional liability was applied which nevertheless is still somewhat hypothetical and full of causal uncertainty. In fact, while the statistics augur a survival percentage of 80%, the patient might still have enjoyed all of the possibilities since this is no more than a statistic. Moreover, awarding this same percentage of compensation could be unfair, as there is a greater likelihood of the person falling within the 80% of patients who overcome the disease and, in such an eventuality, of recovering their health if they had received proper treatment with 100% possibilities (all those within the 80% bracket would overcome the disease).
The Third Chamber of the Supreme Court, without mentioning the criterion of loss of chance, and through the application of another doctrine, namely the ease of proof principle referred to in Article 217 of the Rules of Civil Procedure, resolves this conflict in a totally different and highly logical way by noting that, once malpractice has been demonstrated, and provided that there is a treatment for the condition, the burden of proof must be transferred to the Public Administration so that it may substantiate which damages and what percentage thereof might have been avoided or caused, as applicable, since the burden of proof of a fact or an event that cannot be proven may not be transferred to the victim. This was the ruling reached by Chamber 3, Sect. 4 of the Supreme Court, in the sentence dated 26/03/2012, and Sect. 6, in the sentences issued on 07/07/2008, 20/03/2007 and 17/07/2007.
We might even add that, in some cancer cases, for example, where the only option is to institute palliative care, if such treatment is applied late, it is logical to conclude that the patient would die anyway, although compensation might still be considered given that the patient would have died later had the treatment been initiated earlier. We will all die, that much is certain. The question, however, is when, and if that time arises before it is expected to, death will constitute a breach of the duty of care.
Moreover, the descriptions of the sentences issued in relation to malignant neoplasms and neurological conditions over the 12-year period mainly show that these processes constitute a “high” judicial risk with regard to loss of chance (more than 4 in every 10 loss of chance sentences issued in Spain in the contentious-administrative setting are related to cancer or neurological disease). This indicates that it is in the context of these matters that the loss of chance theory is most frequently applied, precisely because in this area it is extremely difficult to establish a causal relationship with any degree of certainty.
Diagnostic error was the most frequently reported event that gave rise to the sentence (66.5% of the cases analysed). This error is also included in other series as the most frequent grounds for complaint. For example, a recent Swedish study included the judicial claims of 134 women (between 1995 and 2006) who presented the adverse effects caused by a late diagnosis of breast cancer.12 Their misdiagnoses were caused by an incomplete clinical or radiological examination and/or a deficient interpretation of these examinations.12 It was considered that, in at least 1 in 4 cases, the diagnostic delay had a negative impact on the patient's evolution.12 In another review of 559 cases of neurological negligence claims occurring in the UK National Health Service between 1995 and 2005, diagnostic error was cited in 44% of cases, with degenerative disc disease (27%), central nervous system tumours (21%), central nervous system infections (11%) and subarachnoid haemorrhages (9%) being the conditions that generated most claims.13 Finally, in a more recent study of the UK National Health Service, this time lasting up until 2012,14 diagnostic error continued to be the most frequent cause of litigation. However, unlike the previous study, the conditions were different, with spinal pathology, cerebrovascular disease, intracranial tumours, hydrocephalus and neuromuscular disease being the most frequent.14
In conclusion, sentences issued on account of loss of chance in Spanish public medicine have increased considerably over the last few years, mainly due to diagnostic errors and inadequate treatment. Generally speaking, the majority of the patients were males, who died, with malignant cancer and neurological disease being the conditions that generated the highest number of convictions. In most cases, the amount of compensation was established as a lump sum, without taking specific criteria into account.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Sardinero-García C, Santiago-Sáez A, Perea-Pérez B, Albarrán-Juan ME, Labajo-González E, Benito-León J. Responsabilidad por pérdida de oportunidad asistencial en la medicina pública española. Rev Esp Med Legal. 2017;43:5–12.