




Reduction en masse of an incarcerated inguinal hernia occurs when the hernia sac is reduced in the preperitoneal space after a taxis manoeuvre or during hernia repair surgery. The intestinal loops remain incarcerated in the sac, so the intestinal obstruction continues despite the apparently successful hernia reduction.1,2 Reported for the first time by Luke3 in 1843, reduction en masse is an extremely rare complication. In 1908, its frequency was estimated by Corner and Howitt4 at approximately 0.3% of incarcerated hernias, although the current incidence is probably lower due to the increase in early-stage hernia repairs.
We report the case of a 40-year-old intellectually disabled man. He came to the Emergency Department due to abdominal pain associated with a painful left inguinal mass, but he was not able to specify when the symptoms had appeared. Upon examination, the abdomen was soft with no signs of peritoneal irritation; peristalsis was audible. In the left inguinal area, there was a painful mass, compatible with incarcerated inguinal hernia. The mass was spontaneously and completely reduced during a slight exploratory manoeuvre in the Emergency Room. Blood workup and simple abdominal radiograph showed no pathologic findings, so the need for urgent surgical treatment was ruled out; management was planned with hernioplasty scheduled for a later date. Notwithstanding, we decided to keep the patient overnight for observation. Twelve hours later, the patient's condition clearly worsened and he presented symptoms of occlusion and distended small bowel loops on simple abdominal radiograph. However, there was no palpable hernia in the inguinal canal upon examination.
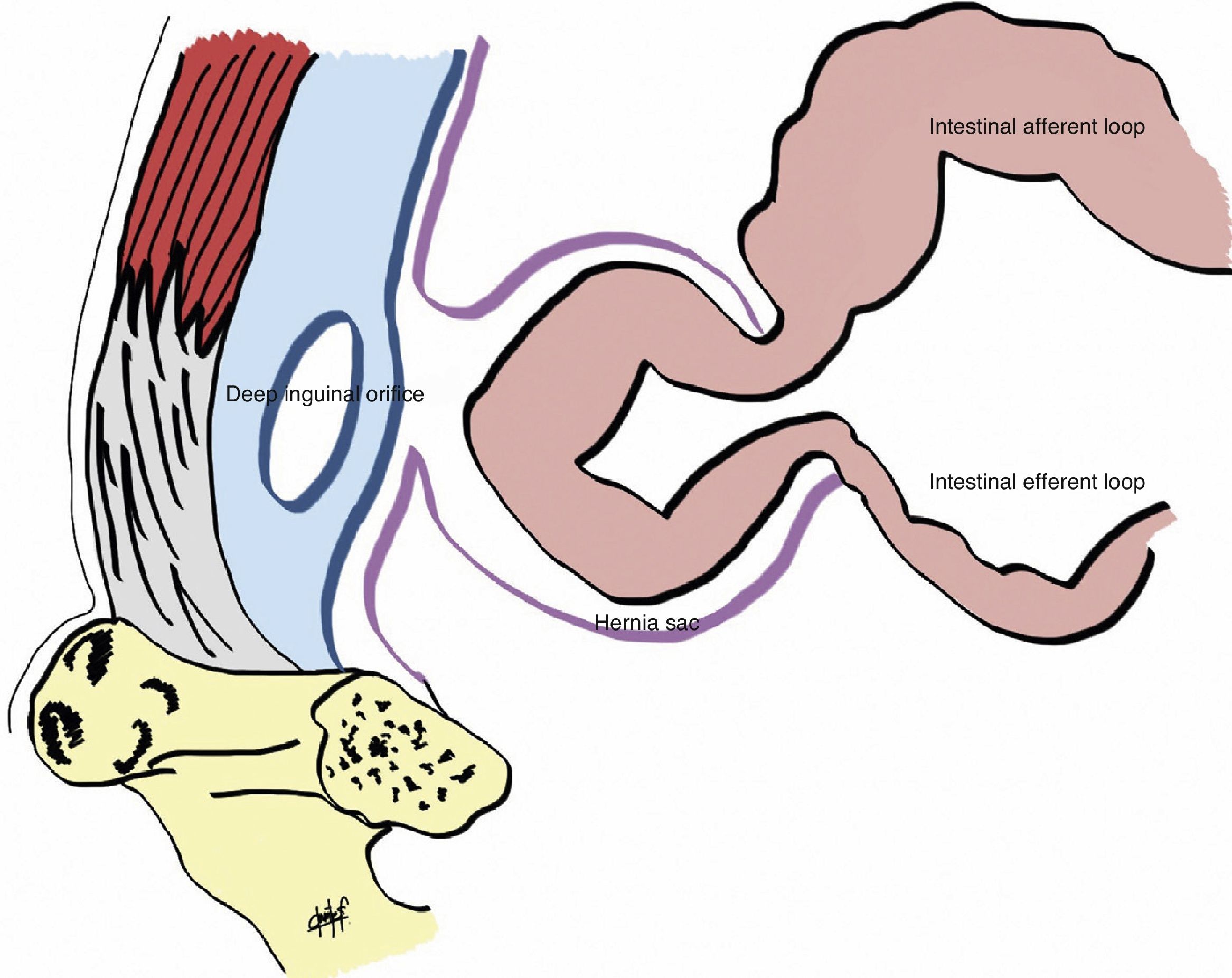
Emergency laparoscopic surgical exploration was indicated. Previous computed tomography was not ordered because the results would not modify the indication for surgery given the worsening symptoms. A 3-port approach was used: 12mm umbilical incision, and two 5mm incisions in both iliac fossae on the midclavicular lines. An indirect inguinal hernia was observed with a segment of the incarcerated ileum in a hernia sac situated in the preperitoneal space, over the deep inguinal orifice (Fig. 1). This was released by means of traction manoeuvres; the affected loop had a congested appearance, with no signs of irreversible ischaemia. Afterwards, hernia repair was performed using the transabdominal preperitoneal (TAPP) hernioplasty technique with a 15cm×10cm polypropylene mesh placed in the preperitoneal space and attached with a spiral endostapler; closure was done with a peritoneal flap. Before the conclusion of the procedure, we once again verified the viability of the affected bowel segment, which had good colour and had recovered peristalsis. The patient had an uneventful recovery, and he was discharged 3 days after the intervention.

Reduction en masse of an inguinal or femoral hernia should be suspected in patients with persistent obstructive symptoms after the apparently effective reduction of an incarcerated hernia. Examination of the inguinal canal will show no evidence of hernia. The diagnosis is confirmed by computed tomography or during surgery, as in the case of our patient. It is important for surgeons to know about this complication because, as it is an uncommon phenomenon, its diagnosis and urgent surgery can be delayed, which can negatively affect prognosis.5
Three conditions are necessary for the reduction en masse phenomenon to occur: a relatively lax deep inguinal ring, a narrow and fibrous neck of the hernia and a space for the preperitoneal sac.1 These factors usually coincide in cases of hernias that have progressed over a long period of time, with a previous history of repeated forced reductions.6 In this case, we have no idea how long the hernia had been evolving or when the acute symptoms had started. We believe that the decision to keep the patient under observation was correct, as was the indication for urgent surgery, which provided a diagnosis and treatment at the same time.
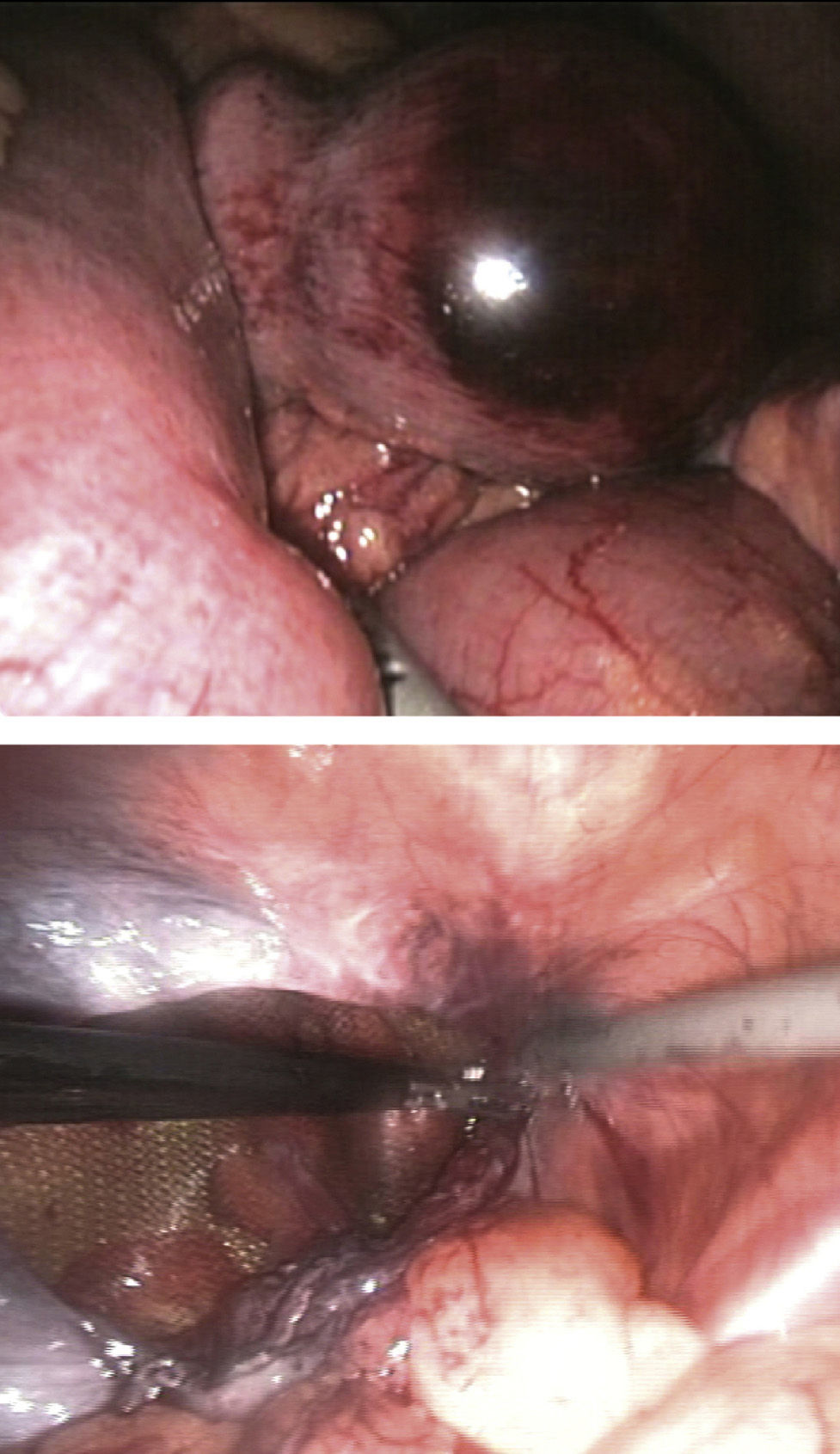
Several authors have used the laparoscopic approach in this phenomenon to verify the visibility of the affected loop7 as well as to provide definitive treatment.8 Hernioplasty using the TAPP technique can be used to manage incarcerated hernias with satisfactory results.9 First of all, the incarceration is released, which will occasionally require a small herniotomy on the fibrous neck and later hernia repair10 (Fig. 2). Although it was not the case in this patient, if there were irreversible ischaemia of the affected loop, bowel resection can be done by mini-laparotomy after concluding the hernioplasty. We should also mention the option of an open preperitoneal approach (which allows for the affected loop to be evaluated), bowel resection without midline laparotomy (if needed), and hernia repair (which could also be done with locoregional anaesthesia).
.")
In conclusion, reduction en masse is an uncommon complication that requires a high rate of suspicion for early diagnosis and treatment. We suggest the laparoscopic surgical approach and hernia repair with the TAPP technique as an effective, less invasive method that accelerates the recovery process, which justifies its use in these patients.
Conflict of InterestsThe authors declare having no conflict interest.
Please cite this article as: Maupoey Ibáñez J, Carreño Sáenz O, Beltrán Herrera H, Moya Sanz A, Carbonell Tatay F. Reducción en masa de una hernia inguinal incarcerada. Abordaje urgente por laparoscopia. Cir Esp. 2015;93:603–605.
