



Amyloidosis in elderly individuals can be an independent alteration and a characteristic of aging. However, the clinical, pathophysiologic, and biochemical characteristics of amyloidosis related to age remain uncertain.
OBJECTIVESThe purpose of this study was to determine the extent to which the heart and/or the brain of individuals aged 60 years or over exhibits amyloid deposits.
MATERIALS AND METHODSThe autopsy findings of individuals who were at least 60 years old were studied. The autopsies took place between the years of 1976 and 2000. A total of 10 cases were selected that had hearts without cardiopathies, had negative serology for Chagas’ disease, and had brains without morphological changes related to encephalopathies. Slides with fragments of heart and brain were processed and analyzed using polarized and common light microscopy.
RESULTSOf the 10 cases, 4 were positive for amyloidosis. All had positive findings in the brain, and 1 case also had positive findings in the heart. Among the positive cases, 50% were of people aged 60 to 69 years. There appeared to be a relationship between the presence of amyloid deposits and the ratio of brain and body weight, with the ratio in the positive cases being smaller than in the negative cases.
CONCLUSIONThe analysis of amyloid deposits in the brains and hearts of elderly individuals shows that such deposits may lead to a systemic attack of senility, common to natural aging. It is not certain that beta-amyloid deposits would alone bring such drastic repercussions to the individual. Some additional disorders of the organism could cause the breakdown of the natural balance related to the accumulation of these proteins, leading the way to the pathological contexts of amyloidosis.
A amiloidose em idosos pode ser uma alteração independente e própria do envelhecimento. Entretanto, as características clínicas, fisiopatológicas e bioquímicas da Amiloidose relacionada à idade ainda permanecem incertas.
OBJETIVOVerificar se o coração e o encéfalo de indivíduos acima de 60 anos apresentavam depósito amilóide.
MATERIAL E MÉTODOSForam estudados laudos consecutivos de autópsias de indivíduos acima de 60 anos realizadas entre 1976 e 2000, que apresentavam corações sem cardiopatias, com sorologia negativa para Doença de Chagas e encéfalos sem alterações morfológicas de encefalopatias, chegando a um n de 10 casos. Lâminas de fragmentos do coração e de encéfalo foram processadas e analisadas em microscopia de luz comum e polarizada.
RESULTADOSDos 10 casos, 3 apresentaram depósito amilóide no encéfalo e 1 no encéfalo e no coração. Em 50% dos casos, os indivíduos tinham entre 60 e 69 anos. A relação entre o peso encefálico e o peso corporal mostrou ter uma associação significativa com os casos positivos, sendo esta menor em relação aos negativos.
CONCLUSÃOA análise conjunta de depósitos amilóides em encéfalo e coração de indivíduos idosos talvez direcione para um acometimento sistêmico comum ao envelhecimento natural. Alguma alteração adicional do organismo poderia determinar a quebra de um equilíbrio natural sobre o acúmulo dessas proteínas, levando dessa forma aos contextos patológicos da amiloidose.
The elderly population has increased over time.1 With aging, several alterations, including amyloidosis (beta-fibrilosis)2 may occur. Amyloidosis, a common structural arrangement, may present different chemical characteristics.3 The most frequent are those from light chains of immunoglobulins found in the alteration of plasma cells, and from AA substance in the serum that are associated with the inflammatory process. Cardiac amyloidosis in elderly individuals can occur regardless of other diseases and is typical of aging, with the heart being the most frequently affected organ.4 In these cases, amyloidosis may be associated with cardiovascular lesions, such as electrocardio-graphic anomalies,5 congestive heart, and atrial fibrillation.6
In recent years, interest in amyloidosis associated with aging has increased, largely due to Alzheimer's disease, a chronic degenerative disease with a high incidence in our population.7 Alzheimer's disease presents extracellular deposits of beta-fibrils.8 With aging, the brain loses the capacity to eliminate these naturally formed proteins, leading to deposits.9 Areas such as the hippocampus and amygdala that constitute the limbic system are common locations for the deposits of these beta-fibril plaques.10,11 Amyloidosis may thus be conceived as the morphological expression of Alzheimer's disease.12 Nevertheless, controversies exist.8,13 Some authors believe that amyloidosis in Alzheimer's disease is not formally associated with aging.14 The only systemic form of amyloidosis formally associated with aging is senile systemic amyloidosis, also called senile cardiac amyloidosis, due to the prevalence of these deposits in the hearts of elderly individuals, described in 25% of the cases of individuals above the age of 80 14 and in 65% of the patients above 90 years of age, but not frequent in individuals under 60 years of age.6
The influence of the aging process as a factor that contributes to the deposits of these proteins is well known. However, the clinical, the pathophysiologic, and the biochemical characteristics of amyloidosis associated with aging remain uncertain. Therefore, the aim of this study was to determine the extent to which the hearts and brains of individuals over the age of 60 contain amyloid material.
MATERIAL AND METHODSConsecutive autopsy reports of elderly individuals over the age of 60 were studied. The autopsies were performed at the Triângulo Mineiro Federal University Medical School Hospital in the city of Uberaba during the period of 1976 to 2000, by the General Pathology Service. Samples and slides of hearts and brains corresponding to the selected reports were located. A spreadsheet was prepared to include the following variables: the number of the report and the year of the autopsy, age, gender, ethnicity, origin, cause of death, body weight, height, body mass index (BMI), weight of the heart, weight of the brain, ratio of the weights of the heart and body, and ratio of the weights of the brain and body. These data were obtained from the autopsy reports.
Amyloidosis was studied in hearts without cardiopathies. Ischemic, hypertensive, chagasic, and valvar cardiopathies, as determined by anatomic/pathological examinations, were excluded. Furthermore, hearts from individuals who tested positive for Chagas disease were excluded. Cases with brains having morphological alterations related to encephalopathies were also excluded. Of a total of 576 cases, 10 cases autopsied during the 1980s and 1990s were selected for the study.
In order to quantify the amyloid deposits, for each autopsy, two 8-micrometer slides of serial cuts of fragments of the aorta, pulmonary trunk, atria, ventricles of the heart, and right and left hippocampus were processed. One of the slides was stained with hematoxylin-eosin for general morphological analysis, while the other was stained with Congo red to identify amyloidosis. For the confirmation of the amyloid deposits, analysis of the slides was done both under common and polarized light microscope.
The nutritional status of the individuals was considered using the BMI.2. For values below 22 or above 27 kg/m2, the individuals were considered undernourished or overweight, respectively.15
Statistical analysis was performed using the Kolmogorov-Smirnof test. Comparison between 2 groups with normal distribution was verified by the Student t test, and the association between qualitative variables was verified using Fischer's Exact test. The level of significance was established at P < 0.05 (5%).
RESULTSThe average age of the elderly individuals was 73.6 ± 10.5 years, with a predominance of Caucasian individuals (60%) between 60 and 79 years of age (80%), of the female gender (60%). As for the geographic origins, the individuals were predominantly from the city of Uberaba (80%). The most frequent cause of death was infection (60%) (Table 1). The average BMI was 20.5 ± 3.8 kg/m2 (mean ± std dev), with a majority of the individuals considered undernourished (60%). The average weight of the brain was 1307 ± 180.1 g, and the ratio of weight of the brain and the body was 0.60 ± 0.63%. Amyloidosis was observed in 4 brains (40%), with 2 of the cases being of beta-fibril deposits found in the hippocampus of both hemispheres (Figure 1). The deposits were characterized by a focal and discrete distribution, appearing as dark orange-colored amorphous deposits under common light and apple-green birefringent under polarized light. Additionally, the amyloid deposit was located next to the cell body of neurons, and in 1 field, the deposit was seen on the wall of a blood vessel. The average age of individuals with amyloid (75.0 ± 10.8 years) was greater than that of individuals without amyloid deposits (72.7 ± 11.1 years); however, this difference was not statistically significant (t = 0.356; P = 0.753). In the positive cases, the ratio of the weight of the brain and body was significantly smaller than in the negative cases (t = 2.683; P = 0.028). There was no significant difference between the average BMI in the positive compared to the negative cases (Table 2).
Distribution of the demographic data of the 10 individuals
| Demographic dada (n = 10) | Positive Amyloidosis | Negative Amyloidosis | Total | (%) |
|---|---|---|---|---|
| Autopsy (decade) | ||||
| 1981 to 1990 | 1 | 2 | 03 | 30 |
| 1991 to 2000 | 3 | 4 | 07 | 70 |
| Age (years) | ||||
| 60 to 69 | 2 | 2 | 04 | 40 |
| 70 to 79 | 1 | 3 | 04 | 40 |
| ≥ 80 | 1 | 1 | 02 | 20 |
| Gender | ||||
| Male | 1 | 3 | 04 | 40 |
| Female | 3 | 3 | 06 | 60 |
| Ethnicity | ||||
| Caucasian | 2 | 4 | 06 | 60 |
| Noncaucasian | 2 | 2 | 04 | 40 |
| Origin | ||||
| Uberaba | 4 | 4 | 08 | 80 |
| Not Uberaba | 0 | 2 | 02 | 20 |
| Nutritional status | ||||
| Normal Nutrition | 1 | 3 | 04 | 60 |
| Undernonrished | 3 | 3 | 06 | 60 |
| Cause of death | ||||
| Infection (I) | 3 | 3 | 06 | 60 |
| Neoplasia | 0 | 3 | 03 | 30 |
| Heart Disease | 1 | 0 | 01 | 10 |
Fischer's Exact Test: Amyloidosis X: decades (81-90); (91-00), P = 0.467; Age (60-79, >=80), P = 1.000; Nutritional status (NN; UN), P = 0.571; gender (M; F), P = 0.571; ethnicity (C; NC), P = 1.000; origin (U; NU), P = 0.467; cause of death (I; NI*), P = 0.464; *(NI): noninfectious
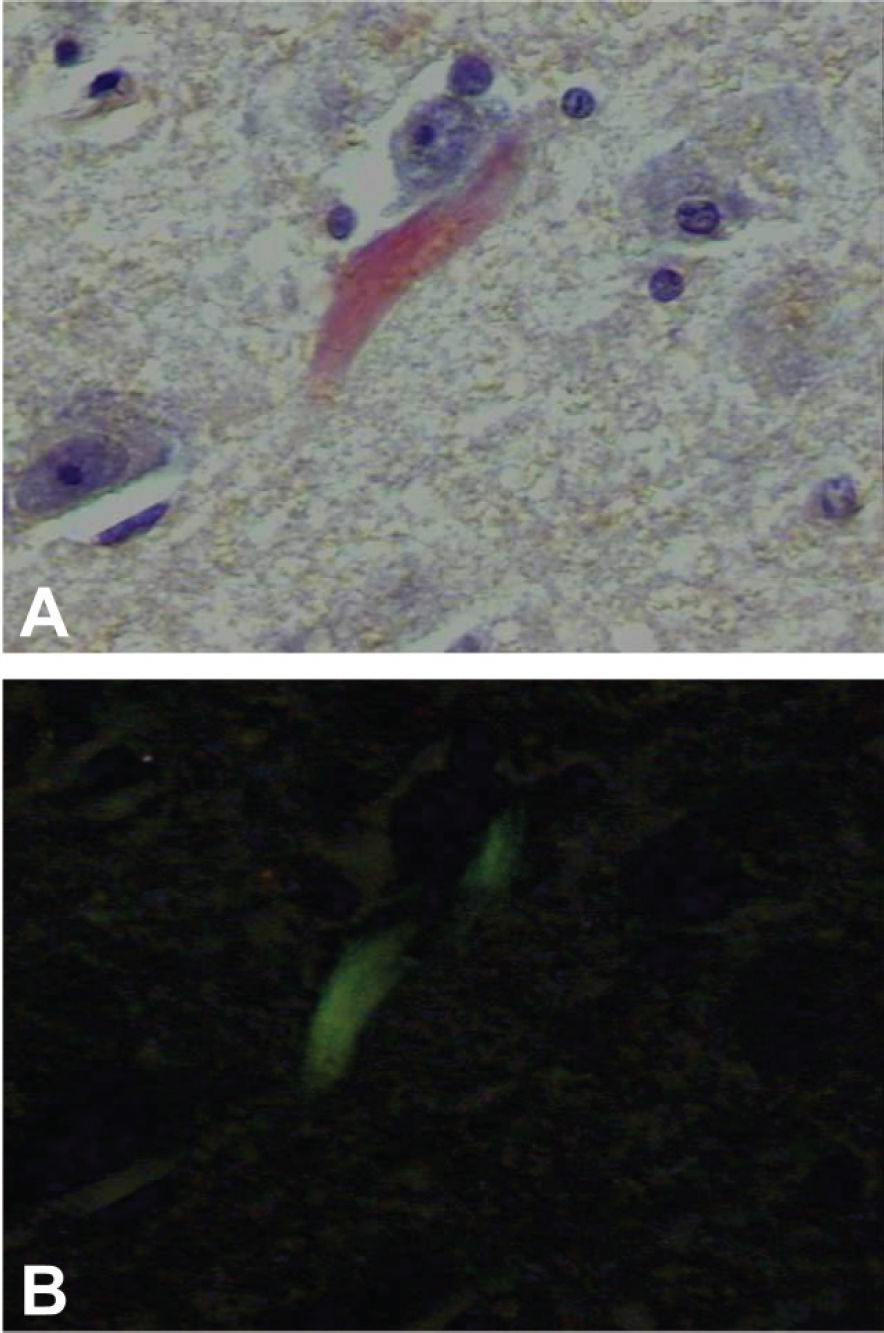
")
Histological section from the hippocampus of an autopsied patient. Note the deposit of congophilic material, in orange, seen under common light, birefringent in apple-green under polarized light, characterizing amyloidosis (Congo-red stain, 40x, under common light – A and under polarized light – B)
Relationship of the demographic data and the amyloidosis of the 10 individuals
| Amyloidosis (Mean ± std dev) | ||
|---|---|---|
| Positive | Negative | |
| Age (years) | 75.0 ± 10.8 | 72.66 ± 11.12 |
| Brain weight (g)* | 1435 ± 146.17 | 1208.33 ± 127.97 |
| Brain weight/Body weight (%)* | 0.58 ± 0.10 | 0.62 ± 0.61 |
| Body Mass Index (kg/m2) | 19.3 ± 3.62 | 21.32 ± 4.02 |
Age: t = -0.326; P = 0.753; Brain weight: t = 2.829, P = 0.022; Brain weight/Body weight: t = 2.683, P = 0.028; Body Mass Index: t = 0.806, P = 0.444
The amyloid process was identified in only 1 heart (10%). The weight of this heart was 280 g, and the ratio of the weight of the heart and the body was 0.55%. Similarly to the findings in the brain, the deposits were characterized by a focal and discrete distribution. The amyloid deposit was found among the cardiac myocytes of the left atrium. In this particular case, deposits of amyloid protein were also present in the individual's brain.
DISCUSSIONThe present study characterized amyloidosis in the hippocampus of both hemispheres of autopsied elderly individuals. The positive cases in this study represent 40% of the cohort. For centenary individuals, deposits of amyloidosis have been reported in over 90% of the cases.16 Accordingly, the hypothesis that individuals with ages above 60 present deposits of amyloid material is supported by our findings.
In the present study, deposits of beta fibrils did not significantly increase with age, which differs from reports in the literature.17 However, the discrepancy may be due to the small size of the sample in this study.
The ratio of the weight of the brain and body showed a significant association with the positive cases, with a smaller ratio in the positive cases. No similar data was found in the literature. A possible explanation for the smaller value in the brain weight/body weight ratio of the positive cases could be in the systemic edema presented by all positive cases, which could be overvaluing the body weight. Nevertheless, when this hypothesis was tested, no statistically significant difference was found. On the other hand, a possible cerebral atrophy of these patients could be a contributing factor for this finding.
Amyloidosis is considered by some authors to be an activity index for the process of Alzheimer's disease. This is because the beta-fibril deposits represent a sum of several processes that generate neuronal lesions, and their presence is an indication of the activity of the disease.12
The natural history of Alzheimer's disease seems to be more dramatic when it affects younger individuals.18 On the other hand, the accuracy of the Alzheimer's disease diagnosis is lower than 80% to 90%, especially in the early stages of the disease.19 The average life span of patients with diagnosis made between the age of 60 and early 70s varies from 7 to 10 years, dropping to less than 3 years when diagnosis occurs after the age of 90.20 This fact demonstrates a relationship between age of the diagnosis and a prognosis for the patient.21 Early detection of Alzheimer's disease might result in a better prognosis for these patients, emphasizing the importance of studies that contribute to a better understanding of the disease. In the present study, 40% of the cases were positive for amyloidosis. Of these cases, 50% were in the 60 to 69 age range. As described above, this age range constitutes the most critical and important period for performing the diagnosis. The more complete the findings of the natural history of this disease, the greater are the chances for the developing of an early intervention aimed at impeding the progress of this class of disease. Furthermore, the development of antiamyloid medication may be essential in elucidating the pathophysiology of Alzheimer's disease.8
In this study, an 89-year-old individual presented focal amyloidosis in the left atrium corresponding to 10%, an index lower that those described in the literature.22,23 The focal distribution of amyloidosis was similar to that described in literature characterizing the senile cardiac amyloidosis. No statistically significant relationship was found in this study between the positive cases and gender, age, ethnical origin, BMI, weight of the heart, and ratio of the weights of the heart and body. Senile cardiac amyloidosis may increase the weight of hearts.14
In conclusion, the findings of amyloidosis in the brains and hearts of elderly individuals without morphological alterations compatible with pathological entities in these organs may guide us towards treating systemic occurrences of amyloidosis in elderly individuals. Amyloid deposits are a result of a common process in the natural aging of human beings. Some organic disorder might cause the loss of the natural balance for the deposits of these proteins, leading to the pathological context of amyloidosis.