




Pheochromocytomas are an infrequent type of neuroendocrine tumor that develop from the enterochromaffin tissue of the adrenal gland medulla, and can synthesize, accumulate and secrete catecholamines and/or their metabolites.
Between 3-36% of all paragangliomas and pheochromocytomas are malignant. Those associated with succinate dehydrogenase subunit B (SDHB) mutations involve an increased risk of malignancy.
IgG4-related disease (IgG4-RD) refers to a recently described immune mediated fibroinflammatory disorder comprising a number of conditions that share a series of histopathological, serological and clinical features. Among other conditions, the IgG4-RD spectrum includes Riedel’s thyroiditis, Mikulicz’s disease (lacrimal, parotid and submandibular gland inflammation) and Ormond’s disease (retroperitoneal fibrosis). It is characterized by infiltrating lesions comprising a dense lymphoplasmacytic infiltrate rich in IgG4-positive plasma cells that produce variable degrees of fibrosis, with a typically storiform pattern, and often also obliterative phlebitis.1,2
No association of pheochromocytoma with IgG4-RD has been reported to date.
A 38-year-old woman with no relevant personal or family history started in February 2018 with initially intermittent and subsequently continuous right-side discomfort associated with anorexia and weight loss. Her family physician requested an abdominal ultrasound study, which revealed a large rounded mass measuring 10 cm in size, of mixed echostructure. The origin of the lesion was difficult to establish, and the patient was therefore admitted for study. In addition to a palpable abdominal mass, the patient presented arterial hypertension that was treated with doxazosin, with high doses being needed to secure adequate blood pressure control.
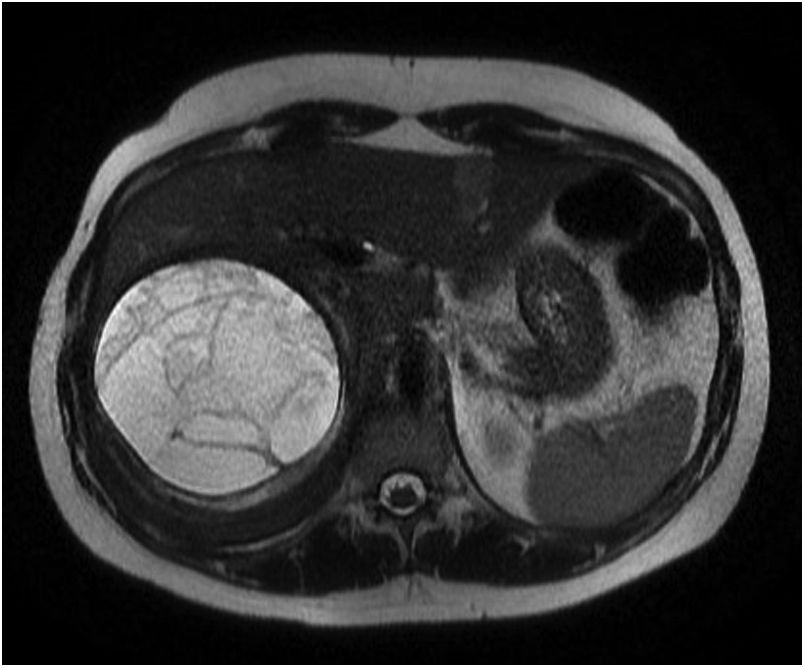
Abdominal CT and MRI confirmed the presence of a large right adrenal mass measuring 11 × 10 × 11 cm in size, with a cystic component surrounded by a retroperitoneal infiltrating lesion displacing the liver and kidney, and compressing the inferior vena cava. The MRI scan showed the lesion to be hypointense in T2-weighted sequencing (Fig. 1). Radiologically, the component surrounding the cystic portion of the lesion had a fibrous or granulomatous appearance.

Fine needle aspiration biopsy (FNAB) of the lesion was performed (with no prior hormone tests), discarding malignancy despite the limitations of cytology in establishing a diagnosis.
Posteriorly, adrenal function tests were requested, revealing a normal cortisol and androgen profile, with catecholamine elevation at the expense of normetanephrine (> 4 times the upper limit of normal [ULN]), thus confirming the diagnosis of pheochromocytoma. Interconsultation with the Endocrinology Department was decided upon.
The study was completed with MIBG plus SPECT/CT, which revealed the presence of deposits within the mass.
In July 2018, the patient underwent open laparotomy with radical nephrectomy, resection of perirenal adipose tissue and adrenal tumorectomy. The operation proved uneventful, and the patient has had good blood pressure control since then, with postoperative normalization of metanephrine levels and an improvement of her clinical symptoms, though the asthenia, anorexia and indeterminate weight loss persisted for some time.
The histopathological study of the adrenal lesion confirmed the diagnosis of pheochromocytoma, and the pathology report on the retroperitoneal lesion was consistent with IgG4-RD.
The genetic study on pheochromocytoma proved negative, being carried out at the National Oncological Research Center (Centro Nacional de Investigaciones Oncológicas) using the standard next generation (massive) sequencing panel that includes all the implicated genes known to date. Serum IgG4 was seen to be normal. The study was completed with a PET scan to determine the extent of the disease. As a relevant finding, a soft tissue lesion with intense FDG uptake (SUVmax 23.8) was identified, which in part could correspond to postsurgical changes, without it being possible to rule out a relapse or locoregional tumor remnants. The control PET scan 5 months later showed a decrease in both the size and intensity of uptake of the lesion, it being interpreted as corresponding to postsurgical changes. At present, the patient continues follow-up, with a good clinical and radiological course, despite not having started treatment for IgG4-RD.
In IgG4-RD, serum IgG4 elevation occurs in only approximately 66% of all patients.3 The exact prevalence of IgG4-RD is not known, in part because of the recent recognition of the disease as such.
IgG4-related disease affects more than one organ in 60-90% of all cases, typically the orbit, salivary glands, pancreas and retroperitoneal tissue, but also the thyroid gland, lung, pleura, aorta, kidney, lymph nodes, prostate, skin, etc. Four disease phenotypes have been described: pancreatic-hepatic-biliary disease, aortitis and/or retroperitoneal fibrosis, disease limited to the head and neck, and classical Mikulicz’s disease with systemic involvement.
The etiology of the disease is not clear. However, there appears to be a possible association with malignancy, the prevalence of cancer being up to two-fold higher in patients with IgG4-RD than in the general population. Recent studies suggest that IgG4-RD could be a paraneoplastic expression of certain tumors; caution is therefore needed when diagnosing this recently described disease.4,5
Patients usually present subacute development of the disease, with the appearance of a mass in the affected organs, associated with discomfort caused by the lesion, depending on its location and size. Weight loss is also common until the disease is diagnosed and treated.
The optimal treatment for IgG4-RD has not been well established. The international consensus documents suggest the administration of corticosteroids as first line treatment to induce remission in all patients with active disease, and also in relapses.6
Of note in our case was the presence of a pheochromocytoma with atypical radiographic characteristics and of a large size in a young patient. Despite the negative findings of the complete genetic study, we suspect that the disorder could possibly be related to unknown genetic alterations. There is no evidence of malignancy to date, though in view of the described characteristics, close follow-up will be needed.7,8
In our opinion, the association of two very uncommon disorders such as pheochromocytoma and IgG4-RD is exceptional, since the combined presence of both conditions has not been previously described. We do not know whether this finding is casual or causal. Improved understanding of IgG4-RD in future will help clarify the true relationship between the two diseases.
Financial supportThe authors state that they have received no funding for carrying out this study.
Please cite this article as: Ramos Carral E, Barrio E, Pazos M, Pedrajas JM, de Miguel P. Primer caso descrito de feocromocitoma asociado a enfermedad por IgG4. ¿Causa o coincidencia? Endocrinol Diabetes Nutr. 2019. https://doi.org/10.1016/j.endinu.2019.10.005
