





Emotional intelligence is defined as "the ability to perceive, assimilate, understand and regulate one's own emotions and those of others, promoting emotional and intellectual growth." The published evidence on the emotional intelligence of nursing staff in charge of a critical area patient in a tertiary hospital is scarce.
ObjectiveTo analyse the emotional intelligence of nursing staff in the critical patient area.
MethodologyA descriptive, cross-sectional, single-centre study carried out in nursing staff of the Intensive Care Units (ICUs) of a tertiary hospital in Catalonia (September 2016). Variables studied: age, gender, work experience in ICU (years worked), and median score (range) of the dimensions of the Meta Mood Trait Scale (TMMS-24) with three dimensions: 1) Emotional attention (I am able to feel and express my feelings adequately); 2) Clarity of feelings (I understand my emotional states well); 3) Emotional repair (I am able to regulate emotional states correctly). A descriptive analysis was undertaken.
ResultsAll active nursing staff (n = 103) were asked to participate in the study: 92 (89%) accepted and completed the questionnaire (75 (82%) women, 17 (18%) men); 51 (55%) were aged between 21 to 30 years-old, and had more than 6 years of working experience in ICU.
The median scores (range) of the different dimensions of the TMMS-24 questionnaire by gender (women/men) were respectively: 1) Emotional attention: 24 (12−37) [Adequate: 25 to 35]; 23 (18−31) [Adequate: 22 to 32]; 2) Clarity of feelings: 29 (15−40) [Adequate: 24−34]; 27 (18−34) [Adequate: 26−35]; 3) Emotional repair: 28 (13−40) [Adequate: 24−34]; 29 (18−39) [Adequate: 24−35].
ConclusionsThe emotional intelligence of the nursing staff was adequate in the dimensions of clarity of feelings and emotional repair. However, it was not adequate in the dimension of emotional attention, therefore it is an area to improve.
La inteligencia emocional se define como "la habilidad para percibir, asimilar, comprender y regular las propias emociones y las de los demás, promoviendo un crecimiento emocional e intelectual”. Las evidencias publicadas sobre la inteligencia emocional del personal de enfermería a cargo de paciente crítico en un hospital terciario son escasas.
ObjetivoAnalizar la inteligencia emocional del personal de enfermería del área del paciente crítico.
MetodologíaEstudio descriptivo, transversal, unicéntrico, realizado en personal de enfermería en activo de las Unidades de Cuidados Intensivos (UCIs) de un hospital terciario de Cataluña (septiembre 2016). Variables estudiadas: edad, sexo, experiencia laboral en la UCI (antigüedad en años), y puntuación mediana (rango) de las dimensiones de la escala de Rasgos Meta-Mood de 24 ítems (TMMS-24) con 3 dimensiones: 1) Atención emocional (soy capaz de sentir y expresar los sentimientos de forma adecuada); 2) Claridad de sentimientos (comprendo bien mis estados emocionales); 3) Reparación emocional (soy capaz de regular los estados emocionales correctamente). Se realizóun análisis descriptivo.
ResultadosSe propuso a todo el personal de enfermería en activo (n = 103) participar en el estudio: 92 (89%) aceptaron y cumplimentaron el cuestionario 75 (82%) mujeres, 17 (18%) hombres; 51 (55%) tenían una edad entre 21 a 30 años y una antigüedad (experiencia) >6 años.
La puntuación mediana (rango) de las diferentes dimensiones del cuestionario TMMS-24 por sexo (mujeres; hombres) fueron: 1) Atención emocional: 24 (12-37) [Adecuada: 25 a 35]; 23 (18-31) [Adecuada: 22 a 32], respectivamente; 2) Claridad de sentimientos: 29 (15-40) [Adecuada: 24-34]; 27 (18-34) [Adecuada: 26-35]; 3) Reparación emocional: 28 (13-40) [Adecuada: 24-34]; 29 (18-39) [Adecuada: 24-35].
ConclusionesLa inteligencia emocional del personal de enfermería fue adecuada en las dimensiones de claridad de sentimientos y de reparación emocional. Sin embargo, no fue adecuada en la dimensión de la atención emocional, por lo tanto es un área a mejorar.
The concept of emotional intelligence (EI) was defined for the first time by the psychologists Salovey and Mayer in 1990. One of the most used definitions considers EI as “the ability to perceive emotions, to access and generate emotions so as to assist thought, to understand emotions and emotional knowledge and to reflectively regulate emotions so as to promote emotional and intellectual growth”. EI has been one of the most well researched and disseminated concepts and is the basis of current research studies.
One of the first tools used to assess EI was the questionnaire called the Trait Meta Mood Scale (TMMS), based on the original model of Salovey and Mayer. The original version of this questionnaire consisted of 48 items. There is a reduced version, the TMMS-24, which has been adapted into Spanish.
In the nursing environment, EI research is still a recent and low-key activity. In fact, EI is crucial for performance in this profession. The nurse* must know how to handle and respond to emotions within the patient care context. This involves both managing their own emotions that may condition the care provided, and managing the emotional needs of their patients. As far as we are aware, sufficient information does not exist in our environment on EI in the experienced nurse who cares for critically ill patients. The objective of this study was therefore to analyse EI in nurses in the critical care area of a tertiary hospital.
The concept of emotional intelligence was first defined by psychologists Salovey and Mayer in 1990.1 One of the most used definitions considers that EI as “the ability to perceive emotions, to access and generate emotions so as to assist thought, to understand emotions and emotional knowledge and to reflectively regulate emotions so as to promote emotional and intellectual growth”.2 However, the person who subsequently popularized this concept was Goleman, who affirmed in his book Emotional Intelligence, published in 1995, that EI is a more precise prediction of academic and/or workplace success than the standard measurements of intelligence (intellectual coefficient).3 Since its popularisation EI has been one of the most researched and disseminated concepts ever, and continues to be the basis of current research studies.
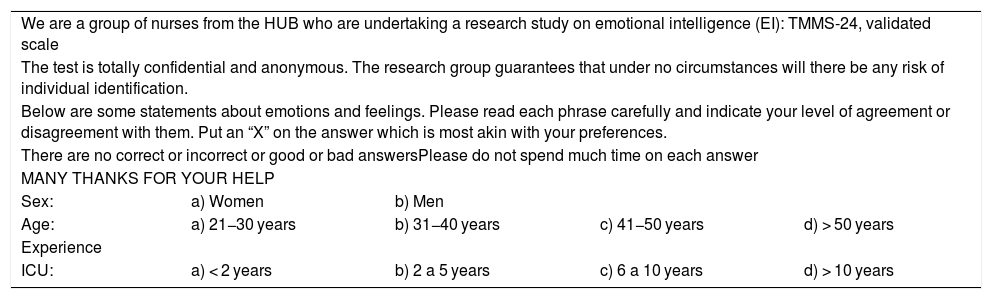
One of the first tools used to assess EI was the questionnaire called the Trait Meta Mood Scale (TMMS), based on the original model of Salovey and Mayer,1 probably one of the most used questionnaires. This tool assesses the perception individuals have of their own emotional skills and their ability to regulate2 them. The original version of this questionnaire consisted of 48 items. There is a reduced version, the TMMS-24, which has been adapted into Spanish, and has been proven to have good psychometric properties to be able to be used with Spanish speaking people.4–6 The TMMS-24 (Table 1) is freeware, easy to complete (it requires around 10 min), easy to correct and to interpret.4,7 It has the additional advantage of being low in costs for research. Although other tools exist for assessing EI, this one has been used the most for its doability.
Trait Meta Mood Scale (TMMS-24) questionnaire.
| We are a group of nurses from the HUB who are undertaking a research study on emotional intelligence (EI): TMMS-24, validated scale | ||||
| The test is totally confidential and anonymous. The research group guarantees that under no circumstances will there be any risk of individual identification. | ||||
| Below are some statements about emotions and feelings. Please read each phrase carefully and indicate your level of agreement or disagreement with them. Put an “X” on the answer which is most akin with your preferences. | ||||
| There are no correct or incorrect or good or bad answersPlease do not spend much time on each answer | ||||
| MANY THANKS FOR YOUR HELP | ||||
| Sex: | a) Women | b) Men | ||
| Age: | a) 21−30 years | b) 31−40 years | c) 41−50 years | d) > 50 years |
| Experience | ||||
| ICU: | a) < 2 years | b) 2 a 5 years | c) 6 a 10 years | d) > 10 years |
| 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|
| Totally disagree | Slightly agree | Quite agree | Very much agree | Totally agree |
| 1. I pay a lot of attention to feelings | 1 | 2 | 3 | 4 | 5 |
| 2. Normally I am highly concerned about what I feel | 1 | 2 | 3 | 4 | 5 |
| 3. Normally I spend time thinking about my emotions | 1 | 2 | 3 | 4 | 5 |
| 4. I think it is worthwhile paying attention to my emotions and moods | 1 | 2 | 3 | 4 | 5 |
| 5. I let my feelings affect my thoughts | 1 | 2 | 3 | 4 | 5 |
| 6. I constantly think about my mood | 1 | 2 | 3 | 4 | 5 |
| 7. I often think about my feelings | 1 | 2 | 3 | 4 | 5 |
| 8. I pay a lot of attention to how I feel | 1 | 2 | 3 | 4 | 5 |
| 9. My feelings are clear | 1 | 2 | 3 | 4 | 5 |
| 10. I can often define my feelings | 1 | 2 | 3 | 4 | 5 |
| 11. I almost always know how I feel | 1 | 2 | 3 | 4 | 5 |
| 12. I normally know my feelings about people | 1 | 2 | 3 | 4 | 5 |
| 13. I often realise my feelings about different situations | 1 | 2 | 3 | 4 | 5 |
| 14. I can always say how I feel | 1 | 2 | 3 | 4 | 5 |
| 15. I often say what my emotions are | 1 | 2 | 3 | 4 | 5 |
| 16. I can understand my feelings | 1 | 2 | 3 | 4 | 5 |
| 17. Although I sometimes feel sad, I usually have an optimistic attitude | 1 | 2 | 3 | 4 | 5 |
| 18. Even when I am in a bad mood I try to think of pleasant things | 1 | 2 | 3 | 4 | 5 |
| 19. When I am sad, I think of all the pleasures in life | 1 | 2 | 3 | 4 | 5 |
| 20. I try to have positive thoughts, even if I am in a bad mood | 1 | 2 | 3 | 4 | 5 |
| 21. If I go over things too much, complicating them, I try to calm myself down | 1 | 2 | 3 | 4 | 5 |
| 22. I am concerned about being in a good mood | 1 | 2 | 3 | 4 | 5 |
| 23. I feel energized when I feel happy | 1 | 2 | 3 | 4 | 5 |
| 24. When I am angry I try to change my mood | 1 | 2 | 3 | 4 | 5 |
In the nursing environment, EI research is still a recent and low-key activity. Nursing is considered to be a highly demanding and stressful profession, due to constant interaction with sick people, family members and healthcare personnel. The critical care nurse requires a solid base of clinical and technological knowledge and skills, which are required for handling the environment around them.8 All of this is crucial to the profession. Different studies have demonstrated that people with higher EI are more able to cope with stressful situations.9 Indeed, the higher the EI, the greater the satisfaction at work, and the physical and emotional well-being of the individual.10
It has been suggested that the nurse should learn to be a catalyst, initiator, and administrator of new situations, strengthening interpersonal relationships within the workgroup and collaborating and cooperating with the team to achieve shared goals in patient care.10,11 The nurse must handle and respond to emotions within the patient care context, with this involving both the management of their own emotions that may condition care provided, and the management of the patients’ emotional needs.12 They must therefore be aware of their strengths and weaknesses, generating feelings of self-confidence, which help the critically ill patient in an effective way, and to generate positive emotions.10 It has been defined that to establish a good nurse/patient relationship their individual emotions must be identified and understood, in addition to the emotions of the patients and their family members.9,12–14 The nurses have to know how to effectively cope with the emotions which arise when in continuous contact with sickness and death.9,12–14 It has been proven that healthcare professionals are increasingly required to offer emotional support, in addition to dealing with health problems all the time.10
According to the literature consulted, information about the EI of experienced critical care nurses is insufficient in our environment. The objective of this study was to describe the EI of nurses in the critical care area of a tertiary hospital.
MethodStudy designA descriptive, cross-sectional, single centre study conducted on the nurses of the Intensive Care Units (ICUs) of a tertiary hospital in Catalonia.
Study populationIt was suggested that all nurses employed in the 3 multi-purpose ICUs of a tertiary hospital in Catalina take part, during the month of September 2016. The following variables were studied: age, sex, working experience in the ICU (in years) and scores from the TMMS-24 items.
Emotional intelligence evaluationEI was evaluated through the TMMS-24 (Table 1). The nurses self-completed the questionnaire voluntarily and anonymously. The TMMS-24 comprises 24 items, and each item may receive a 5-option score (from 1 to 5). This is not a questionnaire with correct or incorrect answers, nor good and bad ones. This questionnaire reflects the preferences of each individual. Sincerity and agility are therefore required when answering each question, since these characteristics are essential for test authenticity.
This questionnaire involves 3 dimensions and each of these dimensions has 8 items:
- 1)
Emotional attention (emotional perception), when the individual is able to feel and express those feelings in an appropriate manner (“attention to feelings” items from 1 to 8)
- 2)
Clarity of feelings (understanding of feelings), is given when the person is well aware of their own emotional status (“clarity of feelings”, items 9–16)
- 3)
Emotional repair (emotional regulation), when a person is able to correctly regulate their emotional states (“mood repair” items 17–24).
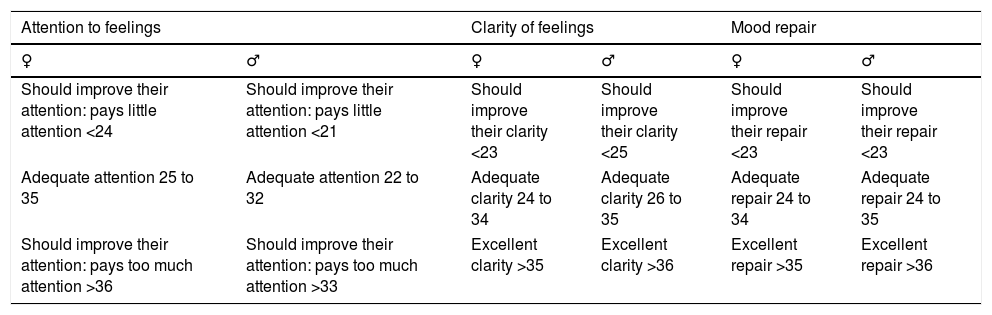
The sum of the score of each of the 8 items in each dimension leads to their assessment and the obtainment of a score for each factor (minimum score of 8 and maximum score of 40). “Appropriate” scores for each domain by sex have been established. Therefore, the scores obtained should match the corresponding reference table (Table 2) of the TMMS-24 questionnaire, without forgetting to distinguish by sex, i.e., whether a man or a woman has responded to the questionnaire.
Interpretation of the scores from the different Trait Meta Mood Scale (TMMS-24) questionnaire dimensions.
| Attention to feelings | Clarity of feelings | Mood repair | |||
|---|---|---|---|---|---|
| ♀ | ♂ | ♀ | ♂ | ♀ | ♂ |
| Should improve their attention: pays little attention <24 | Should improve their attention: pays little attention <21 | Should improve their clarity <23 | Should improve their clarity <25 | Should improve their repair <23 | Should improve their repair <23 |
| Adequate attention 25 to 35 | Adequate attention 22 to 32 | Adequate clarity 24 to 34 | Adequate clarity 26 to 35 | Adequate repair 24 to 34 | Adequate repair 24 to 35 |
| Should improve their attention: pays too much attention >36 | Should improve their attention: pays too much attention >33 | Excellent clarity >35 | Excellent clarity >36 | Excellent repair >35 | Excellent repair >36 |
Convenience sampling was used, incorporating all available volunteers during the study period.
A descriptive analysis of the study variables was made. Continuous variables were described as median and range (maximum and minimum) and categorical variables as absolute frequencies and percentages. Validity of questionnaire usage was assessed using the following variables: “number of participants who delivered the questionnaire” and “number of participants who correctly and completely responded to the questionnaire”.
Data analysis was performed with the R programme version 3.5.0 for Windows.
Ethical considerationsThis study was performed in keeping with that established in the Declaration of Helsinki, and the information collected was treated according to EU Regulation 2016/679 of the European Parliament and Council of 27th April 2016 relating to the protection of physical persons with regard to personal data treatment and free circulation of these data, in addition to the remaining applicable laws and regulations in force.
ResultsStudy populationIt was suggested that a total of 103 ICU nurses take part in the study, all active personnel, during the month of the study. Of these, 92 (89%) agreed to participate and to fill in the questionnaire: 75 (82%) women, 17 (18%) men. All of those who completed the questionnaire did so correctly and completely (they answered all the items).
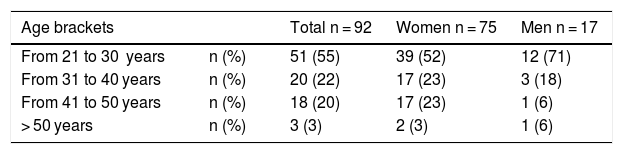
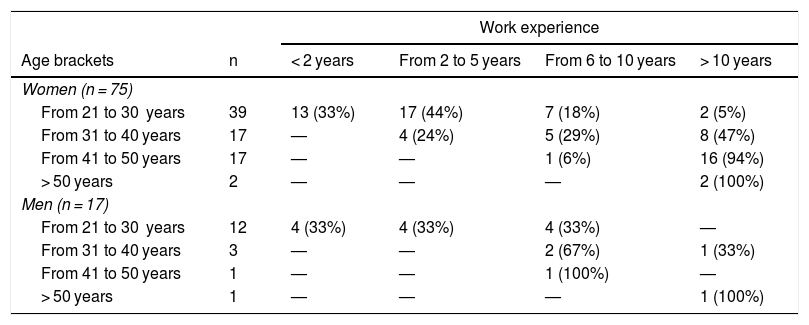
Table 3 shows the distribution of the participants by age and sex. Working experience in the ICU (years) was: <2 years, 17 of 92 (18%) nurses;2 to 5 years, 25 of 92 (27%); 6 to 10 years, 20 of 92 (22%); > 10 years, 30 of 92 (33%). Table 4 shows the distribution of the group of women (n = 75) and of the group of men (n = 17) by age and working experience brackets.
Distribution of the participants by age and gender brackets.
| Age brackets | Total n = 92 | Women n = 75 | Men n = 17 | |
|---|---|---|---|---|
| From 21 to 30 years | n (%) | 51 (55) | 39 (52) | 12 (71) |
| From 31 to 40 years | n (%) | 20 (22) | 17 (23) | 3 (18) |
| From 41 to 50 years | n (%) | 18 (20) | 17 (23) | 1 (6) |
| > 50 years | n (%) | 3 (3) | 2 (3) | 1 (6) |
Distribution of the group of women and the group of men by age brackets and work experience.
| Work experience | |||||
|---|---|---|---|---|---|
| Age brackets | n | < 2 years | From 2 to 5 years | From 6 to 10 years | > 10 years |
| Women (n = 75) | |||||
| From 21 to 30 years | 39 | 13 (33%) | 17 (44%) | 7 (18%) | 2 (5%) |
| From 31 to 40 years | 17 | — | 4 (24%) | 5 (29%) | 8 (47%) |
| From 41 to 50 years | 17 | — | — | 1 (6%) | 16 (94%) |
| > 50 years | 2 | — | — | — | 2 (100%) |
| Men (n = 17) | |||||
| From 21 to 30 years | 12 | 4 (33%) | 4 (33%) | 4 (33%) | — |
| From 31 to 40 years | 3 | — | — | 2 (67%) | 1 (33%) |
| From 41 to 50 years | 1 | — | — | 1 (100%) | — |
| > 50 years | 1 | — | — | — | 1 (100%) |
The overall median (range) score of the TMMS-24 questionnaire was 27 (14–37) in women (n = 75) and 26 (20–33) in men (n = 17).
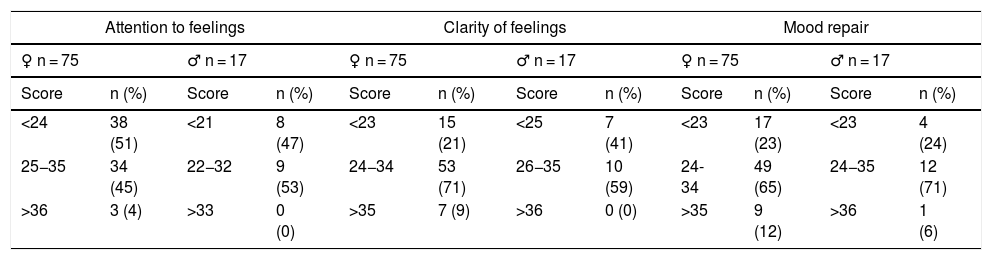
Table 5 presents the median (range) scores from the different dimensions of the TMMS-24 questionnaire by sex, and Table 6 shows the distribution by sex of the scores of the different TMMS-24 questionnaire dimensions.
Scores of the different dimensions from the Trait Meta Mood Scale (TMMS-24) questionnaire by gender.
| TMMS-24 | Womenn = 75 | Menn = 17 | |
|---|---|---|---|
| Attention to feelings | Median (range) | 24 (12−37)(Adequate: 25 to 35) | 23 (18−31)(Adequate: 22 to 32) |
| Clarity of feelings | Median (range) | 29 (15−40)(Adequate: 24 to 34) | 27 (18−34)(Adequate: 26 to 35) |
| Mood repair | Median (range) | 28 (13−40)(Adequate: 24 to 34) | 29 (18−39)(Adequate: 24 to 35) |
Scores of the different dimensions from the Trait Meta Mood Scale (TMMS-24).
| Attention to feelings | Clarity of feelings | Mood repair | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ♀ n = 75 | ♂ n = 17 | ♀ n = 75 | ♂ n = 17 | ♀ n = 75 | ♂ n = 17 | ||||||
| Score | n (%) | Score | n (%) | Score | n (%) | Score | n (%) | Score | n (%) | Score | n (%) |
| <24 | 38 (51) | <21 | 8 (47) | <23 | 15 (21) | <25 | 7 (41) | <23 | 17 (23) | <23 | 4 (24) |
| 25−35 | 34 (45) | 22−32 | 9 (53) | 24−34 | 53 (71) | 26−35 | 10 (59) | 24- 34 | 49 (65) | 24−35 | 12 (71) |
| >36 | 3 (4) | >33 | 0 (0) | >35 | 7 (9) | >36 | 0 (0) | >35 | 9 (12) | >36 | 1 (6) |
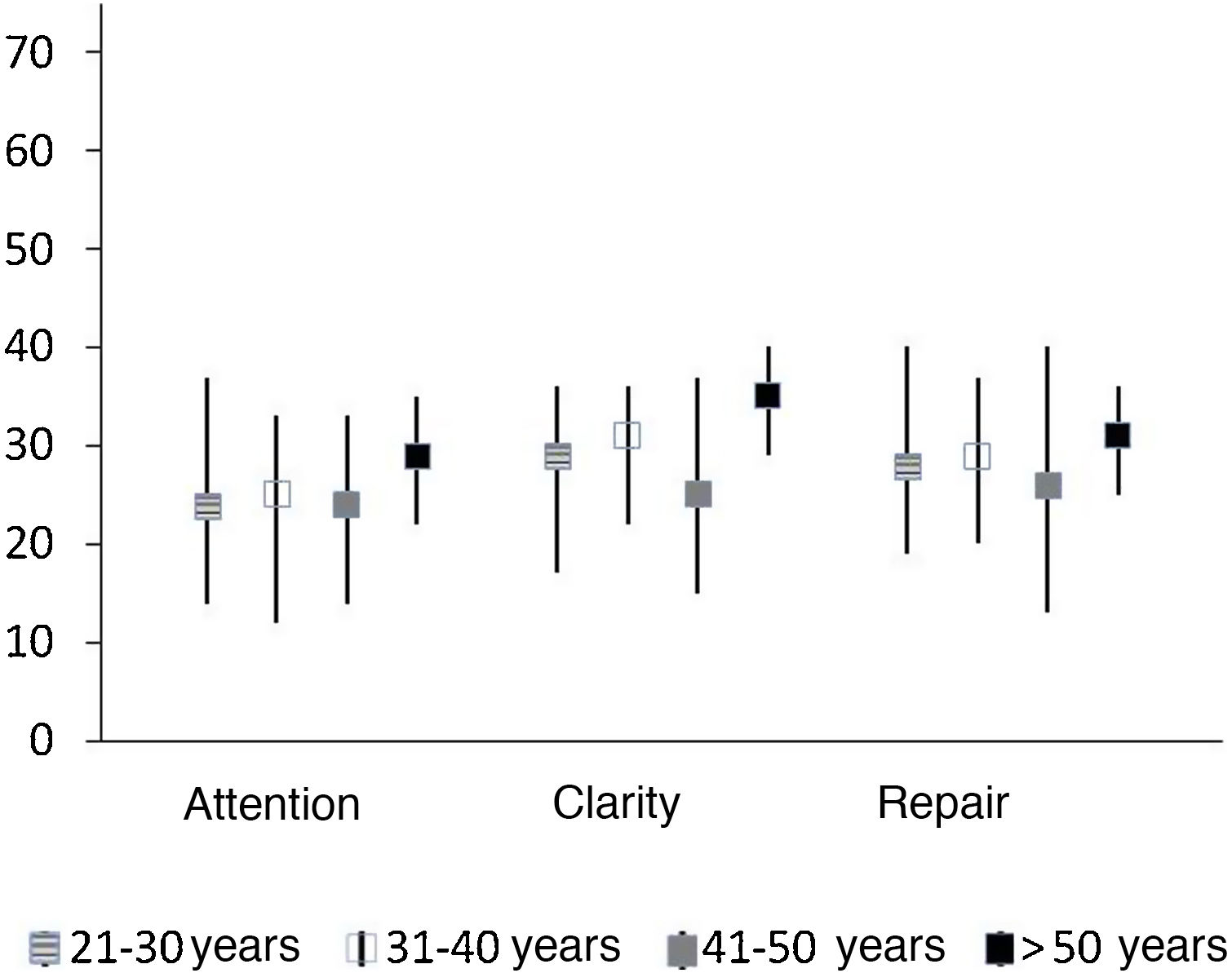
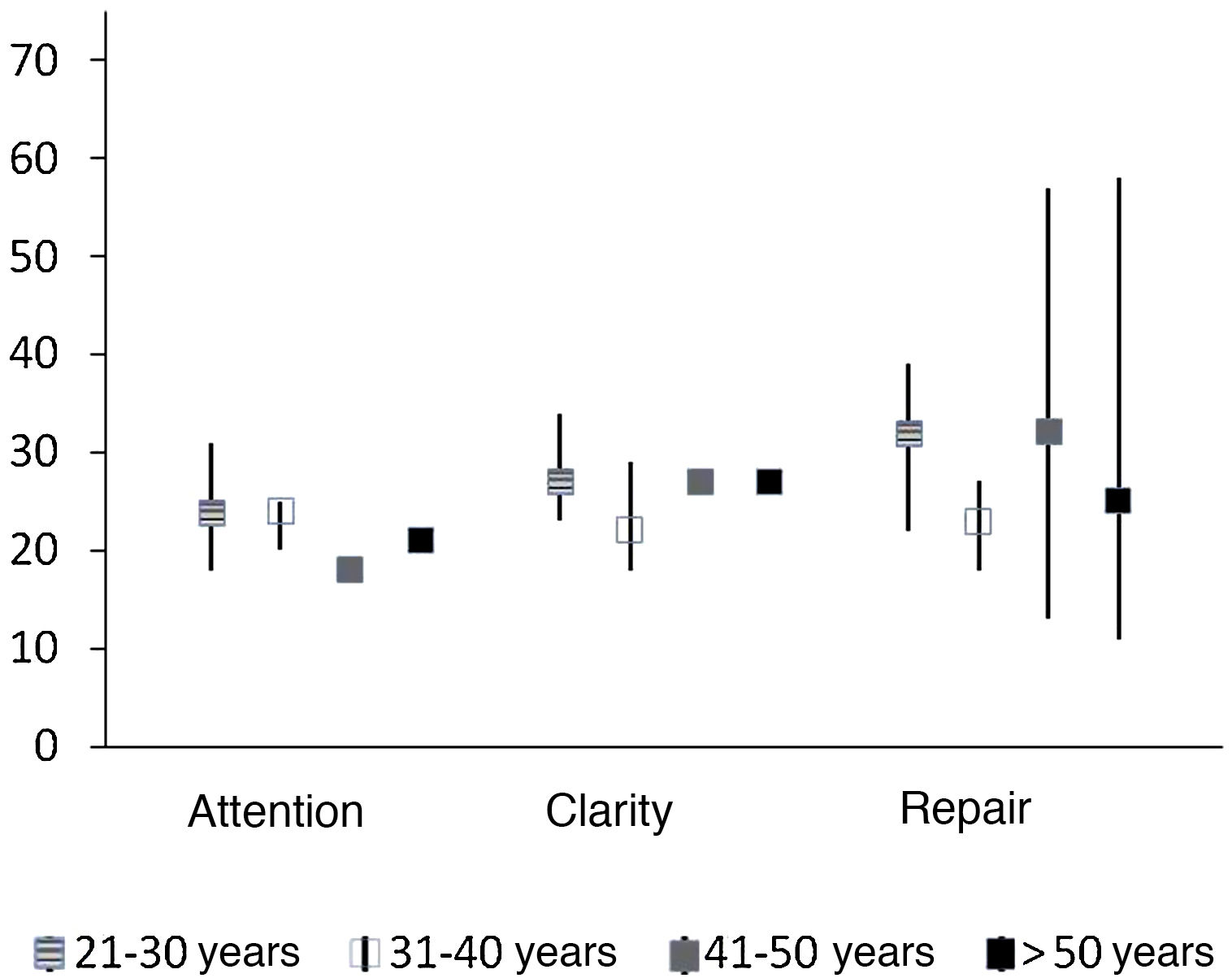
In the emotional attention domain gender differences were observed: 53% (9/17) of the men participants had appropriate attention, compared with 45% (34/75) of the women. Therefore, 47% (8/17) of the men and 55% (41/75) of the women [by defect 51% (38/75) and by excess 4% (3/75)] presented a score which should be improved. In the clarity of feelings domain, it was outstanding that 41% (7/17) of the men also should have improved in understanding their feelings, whilst only 21% (15/75) of the women should have. In the mood repair domain, in both sexes, over 65% [men 71% (12/17) and women 65% (49/75)] of the respondents maintained appropriate emotional regulation. Fig. 1 shows the results of each dimension in keeping with the ages in the group of women (n = 75), and Fig. 2 shows the results of each dimension in keeping with the ages in the group of men (n = 17).
 in women, classified by age bracket and separated by each dimension.")
 in men, classified by age bracket and separated by each dimension.")
According to the review of the literature, few studies describe the EI of ICU nurses in tertiary hospitals based on the TMMS-24 questionnaire. In line with other studies, the use of this questionnaire in the context of nursing has been a tool that has provided information on the EI, particularly in the abilities perceived for interpreting and handling emotions.8,15–18
EI acquires relevant value in the nurse/patient interaction.14 Appropriate management of emotions – both their own, those of the critically ill patient – has a positive impact on the outcome of the healthcare service, therefore on the patient’s health.14,19,20 The scores obtained in the clarity of feelings, mood repair dimensions correspond to results that must be, considered adequate. However, a deficit has been highlighted in the ability to feel, express feelings appropriately, which is a similar result to that observed in other studies.21,22 It is important to underline that in this study active nurses in critical care were the target. In contrast, other authors studied EI in nursing, medical students or in primary care or general nursing, but not in the critical care area.10,15,18,20,21 It is also important to comment that the results obtained concur with one of the conclusions of the doctoral thesis of Ms., Aradilla Herrero 201316: “Nursing professionals tend to pay less attention to emotions but score better in clarity, mood repair”. It is reasonable to think that professionals perceive of better skills due to their greater training, working experience.22 Furthermore, the ability to manage emotions is positively associated with self-esteem, well-being, negatively associated with anxiety, depression.16,23,24 An improvement in this area is therefore that a reduction in stress may be, achieved in healthcare personnel, a better relationship may be, provided for the patients, with an improvement in care quality.
One of the strengths of this study is the high participation of nurses (89%), completing the TMMS-24 questionnaire correctly and fully (no items were left blank or without a response). According to the National Institute of Statistics data, 87% of registered nurses in Barcelona are female.25 As was to be expected, most of the population studied was also female (81%). Another strength of this study was that it is one of the first to provide proof of EI in ICU nurses from a tertiary hospital. In contrast, certain limitations should be considered prior to reaching a conclusion. It was not possible to perform an analysis to correlate the different dimensions of EI with the sociodemographic characteristics of the sample, since this information was not contained within the questionnaire. Although the study design (cross-sectional) may provide information on the viability of the TMMS-24 questionnaire usage and on the emotional status of the nurses, it is not the ideal design for assessing emotional status in keeping with how experience is acquired. Moreover, the sample size (this study is exploratory), and particularly regarding the male sex (17 participants) may under or overestimate the results obtained. As a single centre study extrapolation to other nurses from other ICUs may be limited. The relatively young age of the participants (over 50% were between 21 and 30 years of age) may under or overestimate results obtained. The choice of study period could a priori condition results. To minimize their impact, the month of September was chosen as this is a month that represents a more standard annual population. In other studies, stress felt by nurses and EI have been linked.13,14 The people who presented with lower levels of stress had a higher score in comprehension and regulation of emotions, i.e. they understood and were clear about their emotions as they occurred, were able to regulate or control them and to suffer from lower levels of stress.13
ConclusionsThe results from this study may conclude that the EI of the critical care nurses was appropriate in the dimensions of clarity of feelings and mood repair. However, the attention to feelings dimension was inadequate. As a result, a plan of action should be devised to improve this dimension. In a future study, we should assess the impact of this new plan of action in the IE of nurses in the critical care area.
FinancingThis research did not receive any specific funding from public sector, commercial or not-for-profit entities.
Conflict of interestsAll the authors have no conflict of interests to declare.
The authors wish to thank the cooperation provided by the nurses through their participation in the study and for making the writing of this paper possible.
Please cite this article as: Ordoñez-Rufat P, Polit-Martínez MV, Martínez-Estalella G, Videla-Ces S. Inteligencia emocional de las enfermeras de cuidados intensivos en un hospital terciario. Enferm Intensiva. 2021;32:125–132.

