




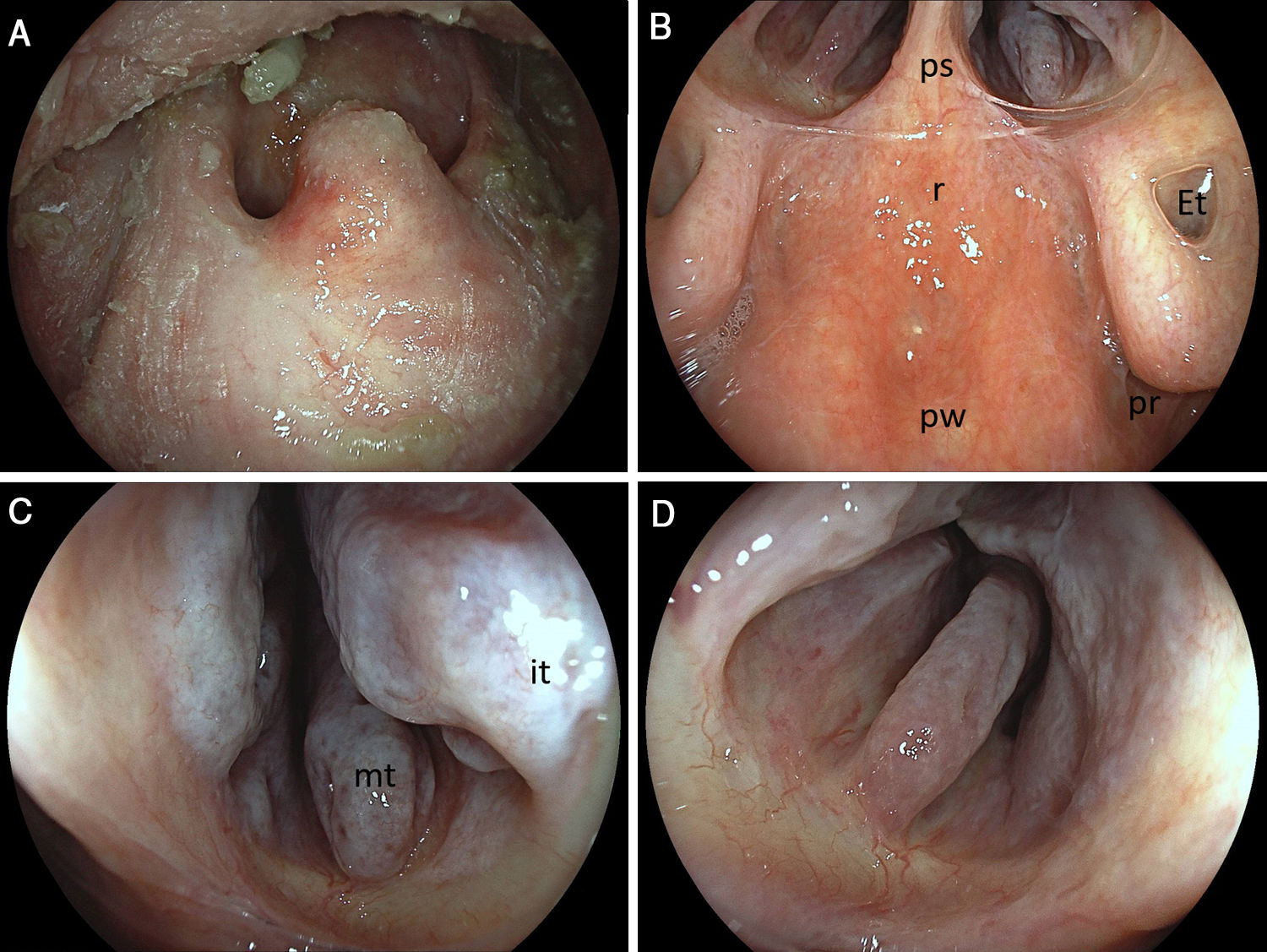
Clinical and endoscopic interest in diagnostics and therapeutics along the “ENT transitroute” during upper endoscopy by dedicated colleagues is constantly rising.1 Along such reasoning, incidental and/or dedicatedly targeted findings in the oral cavity and/or hypopharyngeal structures are increasingly reported in the GI literature. While formerly an exclusive realm of the ENT specialist and terra incognita for gastrointestinal endoscopists, the backside of the nasal cavity, albeit its anterior view may be familiar to those practising nasal-access ultra-slim endoscopy, in the form of high-definition posterior rhinoscopy, achievable during standard scope intubation during esophago-gastro-duodenoscopy and of potential clinical value in work-up of presumed, endoscopy negative upper GI bleeding, may be visualized adequately by GI endoscopy. This is illustrated in an elderly patient post head and neck cancer with marked xerostomia and post-biopsy scar formation in the hard palate close to the uvula. (Fig. 1A) After passing the soft palate and downward movements with the large handle, a panorama posterior rhinoscopy was achieved (Fig. 1B: pw, posterior nasopharyngeal wall; r, nasopharyngeal roof; ps, posterior septum; Et, Eustachian tube opening; pr, pharyngeal recess/fossa of Rosenmüller) as well as close-up visualization of the right (Fig. 1C: it, inferior; mt, middle turbinate -note marked turbinate/conchae hypertrophy potentially related to allergic rhinitis) and left (Fig. 1D) nasal passage.
 Post-biopsy scar formation in the hard palate close to the uvula. (B) A panorama view of the backside of the nasal cavity (posterior rhinoscopy: pw, posterior nasopharyngeal wall; r, nasopharyngeal roof; ps, posterior septum; Et, Eustachian tube opening; pr, pharyngeal recess/fossa of Rosenmüller). (C) Close-up view of the right and (D) left nasal passage: it, inferior; mt, middle turbinate – note marked turbinate/conchae hypertrophy.")
(A) Post-biopsy scar formation in the hard palate close to the uvula. (B) A panorama view of the backside of the nasal cavity (posterior rhinoscopy: pw, posterior nasopharyngeal wall; r, nasopharyngeal roof; ps, posterior septum; Et, Eustachian tube opening; pr, pharyngeal recess/fossa of Rosenmüller). (C) Close-up view of the right and (D) left nasal passage: it, inferior; mt, middle turbinate – note marked turbinate/conchae hypertrophy.
Nothing to declare.
