





To analyse susceptibility/risk of suffering COVID-19 among adults with distinct underlying medical conditions.
MethodsPopulation-based cohort study involving 79,083 individuals ≥50 years old in Tarragona (Southern Catalonia, Spain). Baseline cohort characteristics (demographic, pre-existing comorbidities, chronic medications and vaccinations history) were established at study start (01/03/2020) and primary outcome was laboratory-confirmed COVID-19 occurred among cohort members throughout 01/03/2020–30/06/2020. Risk of suffering COVID-19 was evaluated by Cox regression, estimating multivariable hazard ratios (HRs) adjusted for age/sex and pre-existing comorbidities.
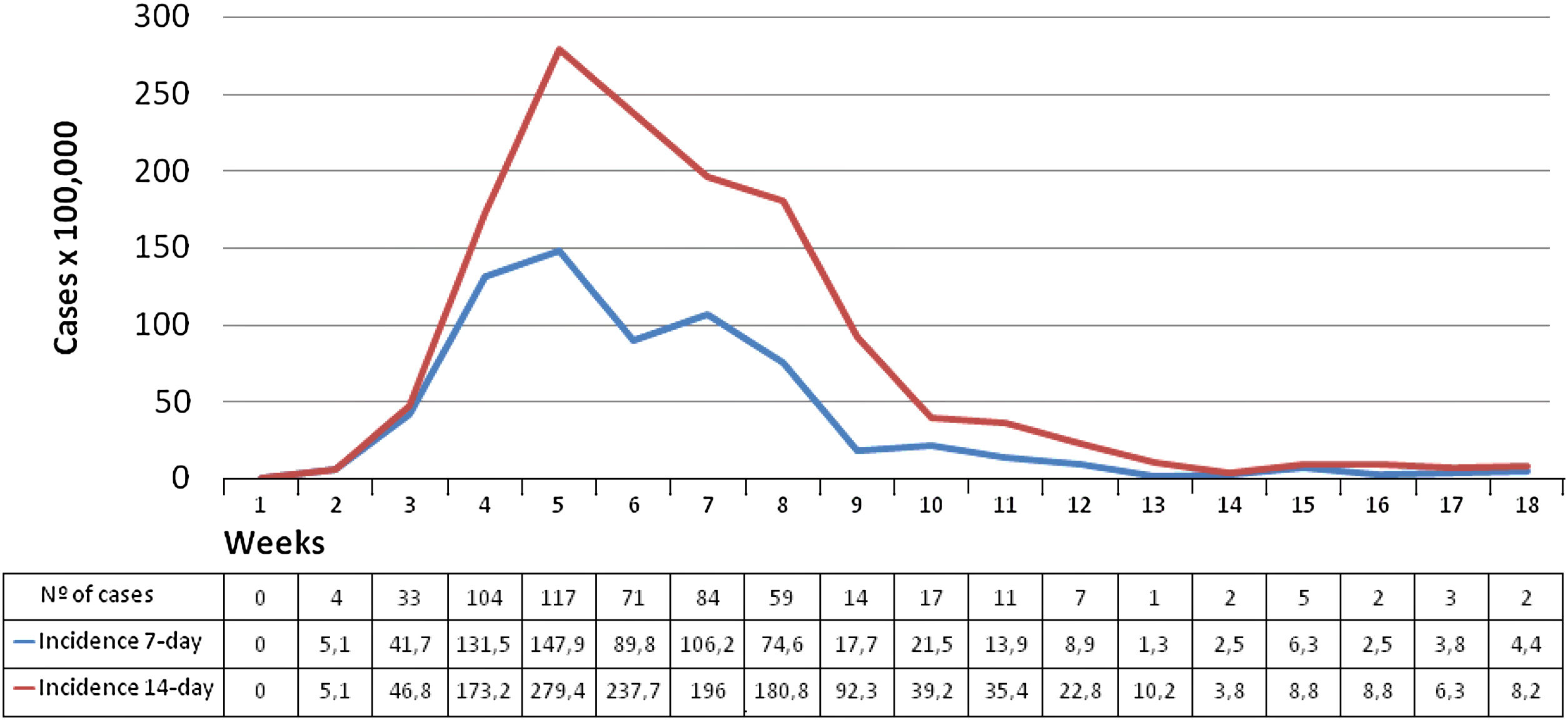
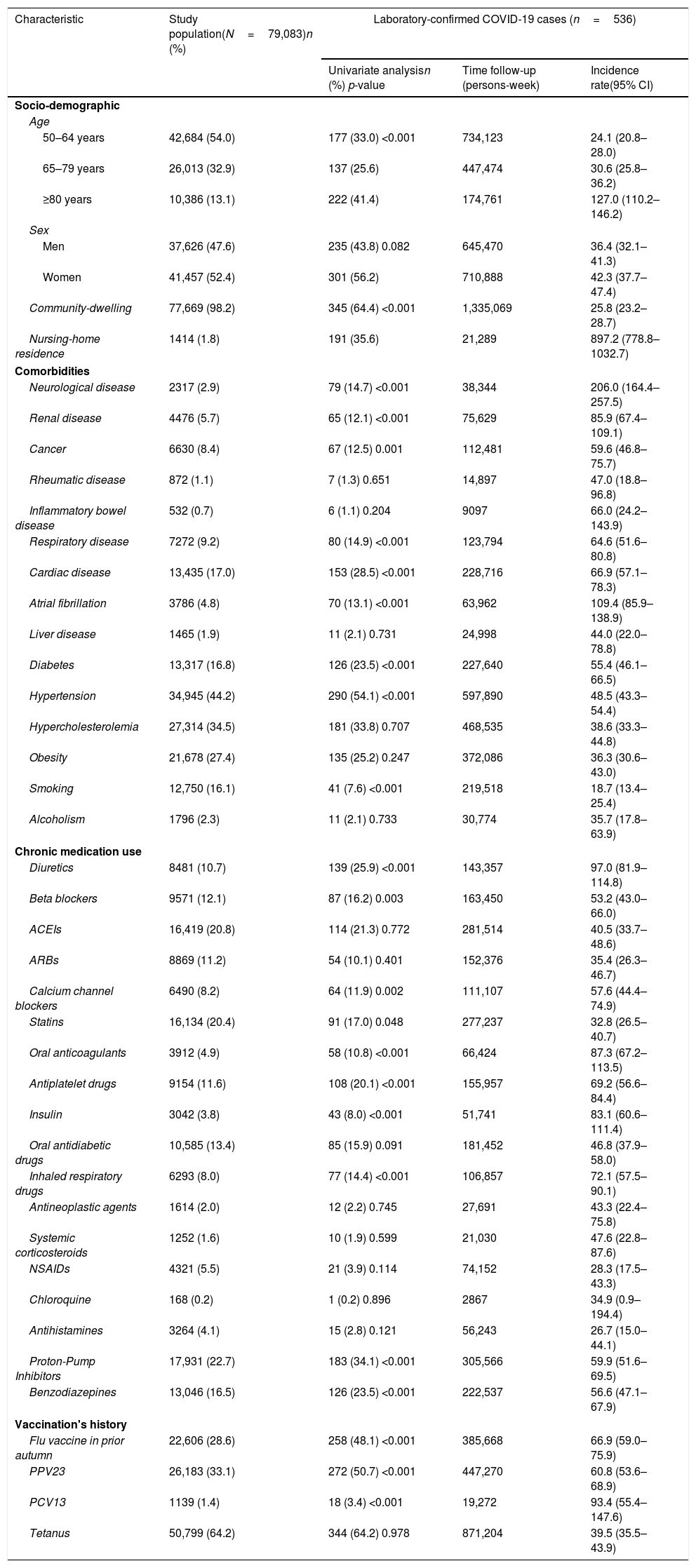
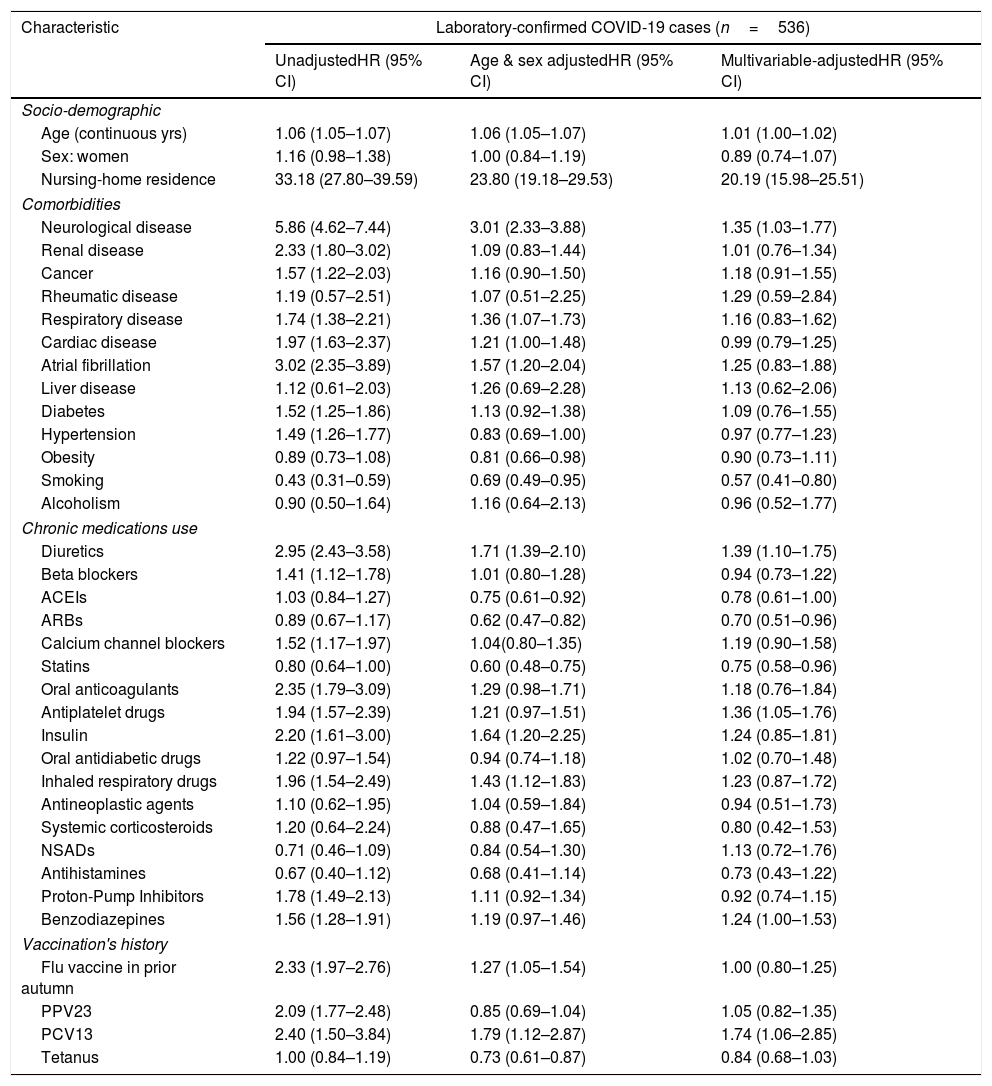
ResultsAcross study period, 536 laboratory-confirmed COVID-19 cases were observed (mean incidence: 39.5 cases per 100,000 persons-week). In multivariable-analysis, increasing age/years (HR: 1.01; 95% CI: 1.00–1.02), nursing-home (HR: 20.19; 95% CI: 15.98–25.51), neurological disease (HR: 1.35; 95% CI: 1.03–1.77), taking diuretics (HR: 1.39; 95% CI: 1.10–1.75), antiplatelet (HR: 1.36; 95% CI: 1.05–1.76) and benzodiazepines (HR: 1.24; 95% CI: 1.00–1.53) increased risk; conversely, taking angiotensin-converting-enzyme inhibitors (HR: 0.78; 95% CI: 0.61–1.00), angiotensin-receptor-blockers (HR: 0.70; 95%CI: 0.51–0.96) and statins (HR: 0.75; 95% CI: 0.58–0.96) were associated with reduced risk. Among community-dwelling individuals, pre-existing cancer, renal and cardiac disease appeared also related with an increased risk, whereas influenza vaccination was associated with reduced risk.
ConclusionIn a setting with relatively low incidence of COVID-19 across the first wave of pandemic period, increasing age, nursing-home residence and multiple comorbidities appear predisposing for COVID-19 among middle-aged/older adults. Conversely, statins, angiotensin-receptor blockers/inhibitors and influenza vaccination were related with decreased risk.
Analizar incidencia y riesgo/susceptibilidad de sufrir la COVID-19 en adultos según distintas condiciones médicas preexistentes.
MétodosCohorte de base poblacional que incluyó 79.083 personas ≥50 años en Tarragona. Características basales de la cohorte (edad/sexo, comorbilidades, medicaciones crónicas) se establecieron a 01-03-2020 y se registraron todos los casos de COVID-19 confirmada ocurridos en miembros de la cohorte hasta el 30-06-2020. Para estimación de riesgos se realizó regresión de Cox, con cálculo de hazard ratio (HR) ajustados por edad, sexo y comorbilidad.
ResultadosSe observaron 536 casos confirmados de COVID-19 (incidencia media: 39,5 casos por 100.000 personas-semana). En análisis multivariante, edad/años (HR: 1,01; IC el 95%: 1,00-1,02; p=0,050), estar institucionalizado/residencia (HR: 20,19; IC 95%: 15,98-25,51; p<0,001), enfermedad neurológica (HR: 1,35; IC el 95%: 1,03-1,77), diuréticos (HR: 1,39; IC 95%: 1,10-1,75), antiagregantes plaquetarios (HR: 1,36; IC 95%: 1,05-1,76) y benzodiacepinas (HR: 1,24; IC 95%: 1,00-1,53) se asociaron con un riesgo aumentado de la COVID-19 analizando la totalidad de la cohorte; contrariamente, medicación IECA (HR: 0,78; IC el 95%: 0,61-1,00), ARA-II (HR: 0,70; IC el 95%: 0,51-0,96) y estatinas (HR: 0,75; IC el 95%: 0,58-0,96) se asociaron con menor riesgo. Entre personas no institucionalizadas, cáncer, nefropatía y cardiopatía se asociaron con mayor riesgo y vacunación antigripal con menor riesgo.
ConclusiónEn un área con relativamente baja incidencia de COVID-19, edad, institucionalización y múltiples comorbilidades aumentaron el riesgo/susceptibilidad de sufrir la COVID-19. Contrariamente, estatinas, inhibidores del sistema renina-angiotensina y vacunación antigripal se asociaron con menor riesgo.

