



The use of pine nuts, the seeds of Pinus pinea, is on the increasing in the modern Mediterranean diet. Little more than 20 cases of allergy to this tree nut have been published, and cross-reactivity with pine pollen, peanut and almond has already been reported. We describe the case of a young boy with several episodes of anaphylaxis after pine nut ingestion. Specific IgE to pine nut and Artemisia vulgaris was demonstrated by skin prick tests and in vitro determination of specific IgE, although no IgE to pine pollen or other nuts was detected. Immunoblotting of Artemisia vulgaris and pine nut revealed two matching diffuse bands, just below 14 kDa and 30 kDa. The ImmunoCAP® inhibition assays showed complete inhibition of pine nut specific IgE after serum incubation with Artemisia vulgaris extract.
As far as we know, this is the first reported case of documented cross-reactivity between pine nut and Artemisia vulgaris.
Pine nuts are the seeds of Pinus pinea, a conifer that belongs to the gymnosperm class of the Pinaceae family. This tree blooms from March to May and is very common in south-western USA, Mexico and southern Europe, especially in Italy, southern France, Spain and Portugal, where it was spread by the Romans.
Nowadays, there is a renewed interest in pine nuts as a food. They are consumed as roasted nuts or added to vegetable salads, pastries, sauces, and even as an oil substitute.
The first authors to report a hypersensitivity reaction to pine nuts were Santos and Unger in 1958.1 Thereafter, little more than 20 cases of allergy to pine nut were reported in the literature and its allergens have been seldom investigated.2
There are some publications that describe crossreactivity between pine nut and other nuts, namely peanut2 and almond,3 or pine pollen.4
CASE REPORTWe describe the case of an 18-year-old boy with perennial complaints of atopic eczema, allergic rhinitis and asthma, from the age of 4, with documented sensitization to Dermatophagoides pteronyssinus, Dermatophagoides farinae and Artemisia vulgaris. In 2002, subsequently to an aggravation of the respiratory complaints, he started specific immunotherapy with 100% Dermatophagoides pteronyssinus extract, with clinical improvement. At the age of 9years he describes a vomiting episode 30 minutes after pine nut ingestión, without other associated symptoms. One year later he refers a vomiting episode, generalized urticaria and dyspnoea 15 minutes after pine nut ingestion, with spontaneous regression after 2 hours. When he was 14years old he again presented an episode of nausea and vomiting 15 minutes after pine nut ingestion and after that he initiated complete avoidance of this tree nut. At the age of 17 he had an episode of rhinitis, generalized urticaria and facial oedema 10 minutes after the accidental ingestion of chicken salad containing pine nuts. In this last episode the patient was admitted to the emergency department and was medicated with parenteral corticosteroids and antihistamines with complete regression of the clinical manifestations in one hour. The patient referred the ingestion of other nuts, including peanut, almond, hazelnut, walnut and pistachio, without any symptoms.
After obtaining patient's informed consent we performed the following investigation:
Skin testsSkin prick tests (LETI, Madrid, Spain) were performed with common aeroallergens (mites, pollens, moulds, and epithelia) and foods (egg, milk, cereals, nuts, fish, fruits, molluscs, crustaceans, and vegetables). Saline was used as a negative control and 10mg/mL histamine phosphate as a positive control. Results were read after 15 minutes and reactions were considered to be positive if the largest wheal diameter was 3mm over the negative control.
Skin prick tests for common aeroallergens proved to be positive to Dermatophagoides pteronyssinus (11 × 15mm), Dermatophagoides farinae (5 × 5mm), Euroglyphus maynei (5 × 5mm), Glycyphagus domesticus (7 × 4mm) and Artemisia vulgaris (10 × 7mm), but negative to pine pollen and all the other common allergens tested. Skin prick tests with foods were positive to pine nut (14 × 10mm) and negative to all the other foods tested including peanut, almond, hazelnut, walnut and pistachio (Fig. 1).
Total and specific IgE.")
Total serum IgE was determined by the Alastat method (DPC, Los Angeles, CA, USA) and specific IgE was determined by ImmunoCAP® (Phadia, Uppsala, Sweden), both performed according to the manufacturer's instructions.
Total serum IgE was elevated (310 kU/L). Specific IgE was positive to pine nut (0.63 kU/L), Artemisia vulgaris (6.7 kU/L), Dermatophagoides pteronyssinus (39.5 kU/L) and Dermatophagoides farinae (13.1 kU/L).
ImmunoCAP inhibition assays:Twenty-five microlitres of serum was mixed with 25 μL of serial dilutions of inhibitor extract, starting at 1/10 (dry weight/volume, 100mg/mL), in PBS. After overnight coincubation at 4°C, ImmunoCAP results were assessed according to the manufacturer's instructions.
The ImmunoCAP inhibition assays showed complete inhibition of pine nut specific IgE after serum incubation with Artemisia vulgaris extract but only very limited, 7 %, inhibition of Artemisia vulgaris specific IgE after serum incubation with pine nut extract.
SDS-PAGE and blottingSeparation and blotting equipment from Novex, Invitrogen, USA, except biotin protein standard and BCIP/NBT colour system (Bio-Rad, USA), Streptavidin-Alkaline phosphatase (Zymed, USA) and biotin-anti-IgE (MIAB, Sweden) was used.
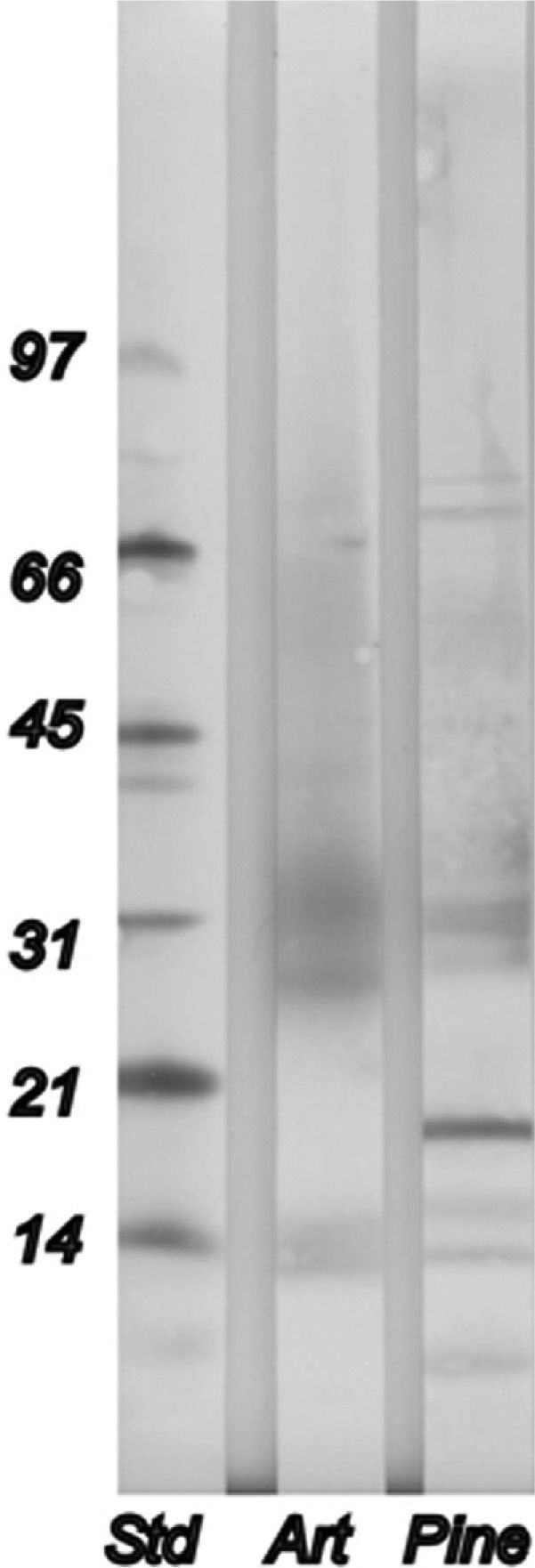
Immunoblotting to Artemisia vulgaris and pine nut revealed two matching diffuse bands, one just below 14kDa, and one below 30kDa (Fig. 2).
DISCUSSION and pine nut (Pine), in relation to a protein standard (Std).")
Allergens of pine nut have been studied and characterized by immunoblotting assays in a few reports, and some cross-reactivities have been described.
In 1990 Koepke JW et al. proved, by electrophoresis of pine nut extracts, 30 proteic bands, three of which were in the range of 66 to 68kDa.5 De las Marinas et al. reported, in 1998, an important allergenic band with molecular weight of 50kDa, which disappeared after blotting inhibition with an almond extract, in a patient previously sensitized to almond who presented systemic reactions after ingestion of pine nuts.3 Garcia-Menaya et al. detected through SDS-PAGE a new 17kDa band not previously described, with the interesting property of being rendered nonreactive upon either the transfer to nitrocellulose using conventional electrophoretic methods or reduction.6
In 2002, Añó et al. described, in a patient with pine nut allergy, bands of 30 and 44kDa that disappear after blotting inhibition with peanut.2
With regard to cross-reactivity to aeroallergens, pine nut allergy has been described in only one patient with pine pollinosis but the allergens were not studied.7 On the other hand, Senna et al. described IgE reactivity with peptides in extracts from both pine nut and pine pollen in patients who were symptomatic to the nut but not to the pine pollen.4
In our patient the clear history of severe reaction to pine nut and the skin prick test positivity with standardized pine nut extract obliged us to consider unethical to perform the confirmatory oral challenge test. Furthermore, since acute anaphylactic reactions after pine nut prick-prick skin testing have already been reported8 we decided not to perform this type of skin test in our patient. Nevertheless, the clear clinical history, the skin test and specific IgE positivity to pine nut allowed us to establish with a high probability the diagnosis of pine nut allergy. Consequently, we recommended strict pine nut avoidance and prescribed an epinephrine auto-administration kit.
Regarding cross-reactivity between Artemisia vulgaris and pine nut, as shown by immunoblotting, there were no obvious, clear bands with molecular weight match between the two allergens, however there were two diffuse bands of molecular weight, one just below 14kDa and one below 30kDa for both allergens. Moreover, ImmunoCAP inhibition assays showed complete inhibition of pine nut specific IgE after serum incubation with Artemisia vulgaris extract but only very limited, 7 %, inhibition of Artemisia vulgaris specific IgE after serum incubation with pine nut extract, demonstrating cross-reactivity between pine nut and Artemisia vulgaris.
These results also suggest that the primary sensitization was to Artemisia vulgaris which is in harmony with the clinical history, since Artemisia vulgaris sensitization was first documented when he was 4years old and the first episode of pine nut allergy happened at the age of 9years.
Cross-reactivity between Artemisia vulgaris and nuts has been reported, namely hazelnut,9 chestnut,10 peanut,11 and almond.11 As far as we know this is the first reported case of documented cross-reactivity between pine nut and Artemisia vulgaris.
