



Since impaired gallbladder emptying contributes to gallstone formation, the evaluation of gallbladder motility requires accurate methodology. Recently developed 3-dimensional ultrasonography may take into account various gallbladder shapes more accurately than conventional 2-dimensional ultrasonography. Therefore, volumes of water-filled balloons of various sizes were determined in vitro by 2-dimensional ultrasonography with the sum of cylinders method and by 3-dimensional ultrasonography. Also, in 15 gallstone patients and 6 healthy volunteers, fasting gallbladder volumes and postprandial motility were determined by both methods. Volumes of water-filled balloons as measured by both methods correlated strongly with true volumes (R= 0.93 for 2-dimensional and R = 0.98 for 3-dimensional ultrasonography). Gallbladder volumes measured by both methods were also correlated (R = 0.66, P < 0.001). In gallstone patients, 3-dimensional ultrasonography yielded smaller gallbladder volumes than 2-dimensional ultrasonography (P = 0.007), but not in healthy subjects. With both methods, gallstone patients exhibited decreased postprandial gallbladder motility compared to healthy subjects. In conclusion, gallbladder volume measurements by 3-dimensional and 2-dimensional ultrasonography are strongly correlated. Nevertheless, in gallstone patients, gallbladder volumes by 3-dimensional ultrasonography tend to be smaller than by 2-dimensional ultrasonography, possibly due to interference of gallstones with the volume measurement.
Gallstones frequently occur in the Western world (1012% of the adult population are gallstone carriers),1 and lead to considerable health expenses. Most of these gallstone carriers exhibit cholesterol stones.2 Cholesterol crystallization from supersaturated bile is a prerequisite for cholesterol gallstone formation. Impaired gallbladder emptying could promote gallstone formation by providing time for nucleation and subsequent aggregation of cholesterol crystals. Also, impaired emptying may enhance concentration of gallbladder bile with increased crystallization as a result.3,4 In gallstone patients, both postprandial and interdigestive (fasting) gallbladder motility are impaired.5 Also in various conditions such as pregnancy,6 obesity7 and treatment with somatostatin analogues,8 impaired gallbladder emptying is associated with increased risk of gallstone formation. Nevertheless, preserved gallbladder emptying is associated with risk of acute pancreatitis in gallstone patients.9 It remains unclear if gallbladder motility could also affect occurrence of biliary pain or other complications of gallstone disease. Several agents affect gallbladder motility.10 To study their role in pathogenesis, treatment and prevention of gallstone disease, accurate quantitation of gallbladder motility is essential.
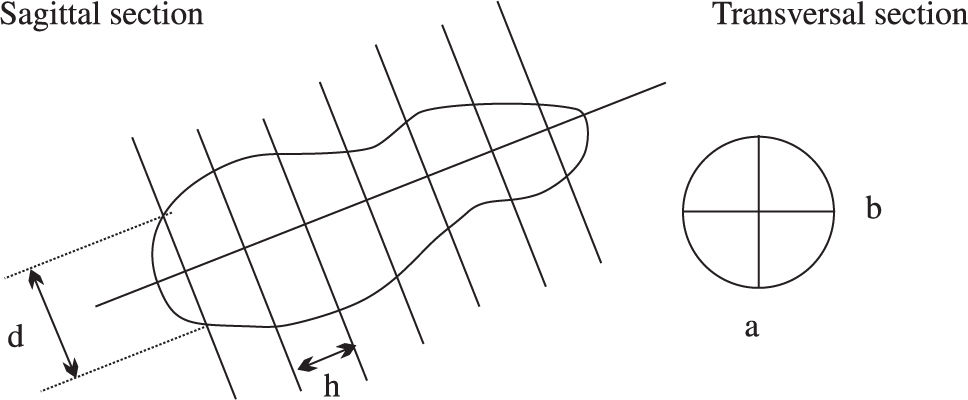
Various methods have been used to measure gallbladder emptying, such as oral cholecystography11 and 99Tc-Hida scanning.12,13 Gallbladder volumes can be determined by 2-dimensional (2D) ultrasonography by the ellipsoid method(14). This method determines gallbladder volumes using the following formula: V = • /6 * L* W * H, (L = maximum length, W = maximum width, H = maximum height). However, to date the gold standard to determine gallbladder volumes is real-time 2D ultrasonography with the sum-of-cylinders method.15,16 With this method, gallbladder volume is determined by dividing the gallbladder image on the sagittal scan in a series of cylinders of equal height. The volumes of the individual cylinders are then summated and, based on the transverse scan, a correction factor is applied to correct for positioning of the sagittal scan from the central axis of the gallbladder (Figure 1). Nevertheless, this method is tedious and time consuming, unless a computer program is available. Theoretically, deviations of gallbladder shape could affect results. Recently, a new modality has been developed to estimate gallbladder volumes: 3D (3-dimensional) ultrasonography. This has been established as an adequate method for measurement of intragastric volumes.17-19 A potential advantage of 3D ultrasonography is that a sagittal section of the gallbladder at its maximal diameter is not required, which may be important in patients with irregular gallbladder shapes. Therefore, 3D ultrasonography methodology may better take into account variations in gallbladder shapes. The aim of the present study was to compare 2D and 3D ultrasonography by in vitro measurements of water-filled balloons. We also compare postprandial gallbladder volumes by 3D and 2D ultrasonography in healthy volunteers and patients with uncomplicated gallbladder stones.
 * (a + b/2* dmax)2 Based on the transverse section, the correction factor: (a + b/2x d)2 is applied to correct for positioning of the sagittal scan from the central axis of the gallbladder.")
2-dimensional ultrasonography with the sum of cylinders method. A schematic representation is shown of 2-dimensional ultrasonographically obtained sections with the sum of cylinders method. a and b represent width and height of each cylinder, whereas h represents the height of each cylinder and d the diameter of each cylinder. Gallbladder volume is calculated by the formula: V= ••4 * h * (• d, 2) * (a + b/2* dmax)2 Based on the transverse section, the correction factor: (a + b/2x d)2 is applied to correct for positioning of the sagittal scan from the central axis of the gallbladder.
Volume measurements were performed by scanning water-filled balloons in a water tub. Various balloon volumes of 10, 20, 30 and 40 mL were investigated 3 times in a random order by both 2D and 3D ultrasonography. The investigator performing the measurements and analysis was blinded for these volumes.
SubjectsGallbladder volume measurements were performed in 6 healthy volunteers (1 male/5 females, 23 ± 1 yrs, BMI (body mass index) 22 ± 1 kg/m2) and 15 gallstone carriers (8 males/7 females, 52 ± 8 yrs, BMI 28 ± 1 kg/m2) with uncomplicated disease (no history of obstructive jaundice, acute cholecystitis, acute pancreatitis or cholangitis). Written informed consent was obtained from all subjects. Approval was obtained from the ethical committee of our hospital.
UltrasonographyFasting and postprandial gallbladder volumes were measured by real-time 2D ultrasonography (3.5 MHz convex transducer, Pie Medical Scanner 250, Pie Medical, Maastricht, The Netherlands) using the sum-of-cylinders method (Figure 1). The 3D imaging system consisted of a commercially available ultrasonography scanner (Esaote-Pie Medical, Maastricht, The Netherlands) with a 3.5 MHz curved ultrasonography probe and a tracking system (Esaote-Pie Medical, Maastricht, The Netherlands). The tracking system consisted of a transmitter generating a spatially varying magnetic field and a small receiver containing three orthogonal coils to sense the magnetic field strength. The receiver was firmly attached to the ultrasonography probe. Data were transferred to the computer workstation and stored on a 30 GB hard disk. Data processing was done on a Windows-NT version 4.0 workstation equipped with two 233 MHz Pentium processors and 256 MB RAM.
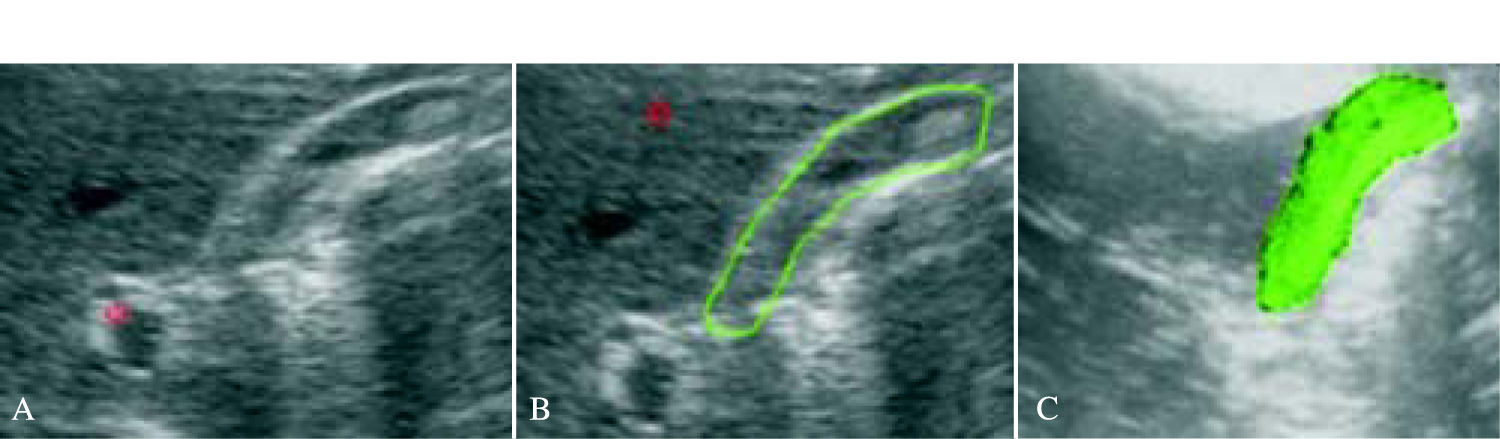
The pulse magnetic field generator positioned closely behind the subject’s chair, or water tub, was used for 3-dimensional orientation. A ‘sweep’ was performed from a point just medial of the gallbladder ending just lateral of the gallbladder, during breath-hold of the subject. In the water tub, a “sweep” was performed immobilizing the balloon, beginning where the balloon was not yet visible, ending where the balloon was no longer visible. During each sweep, about 200 images were obtained and stored within 10 seconds. Computerized post-processing (In vivo, MedCom GmbH, Germany) started with manual outlining the region of interest using the sagittal 2-dimensional slices that were obtained during the sweep. After re-sampling of the images, the gallbladder inner wall or balloon wall were used as a border for manual drawing in the selected images. When all images were well drawn (by manual outlining or interpolation), a 3-dimensional image was obtained and the computer calculated the volume of the 3-dimensional image (Figure 2). Subjects were positioned in a chair in the upright position while measurements by both methodologies were obtained.
Gallbladder volumes and postprandial motility, manual outlining, (B) and computer calculated 3-dimensional reconstruction, (C) of the gallbladder are shown.")
In the fasting state, two gallbladder volume measurements were made by 2D ultrasonography and two sweeps were performed by 3D ultrasonography. The standard semi-solid mixed meal consisted of 30 g fat, 30 g protein and 70 g carbohydrate (2815 kJ). After meal ingestion, gallbladder volumes were determined at 15 min. intervals during 2 hours. Each postprandial measurement was performed by both methods. The following gallbladder contraction parameters were determined by both methodologies in both groups: fasting volume (FV in mL), minimal residual volume (RV, in mL and in % of FV) and maximal decrease of gallbladder volume (• Vmax in mL and in %).
Statistical analysisResults are expressed as mean ± SEM. Differences between 2D and 3D ultrasonography were tested by paired Student’s t-tests in all subjects, as well as in subgroups. Differences between gallstone carriers and healthy volunteers were tested by unpaired Student’s t-tests. When data showed a non-Gaussian distribution, Mann-Whitney-U test was used to test differences. Differences between gallbladder contraction curves were tested by GLM ANOVA. Linear regression analysis was used to determine correlations between volumes obtained by 2D vs 3D ultrasonography. A two-tailed probability < 0.05 was considered statistically significant.
ResultsIn vitro measurements of water-filled balloons
Volumes of water filled balloons determined by 2D ultrasonography correlated strongly to true volumes (R = 0.93, r = 1.19, P < 0.001). A strong correlation was also found between volumes determined by 3D ultrasonography and true volumes (R = 0.98, r = 1.09, P < 0.001).
In vivo measurements by 2D vs 3D ultrasonography in human subjects
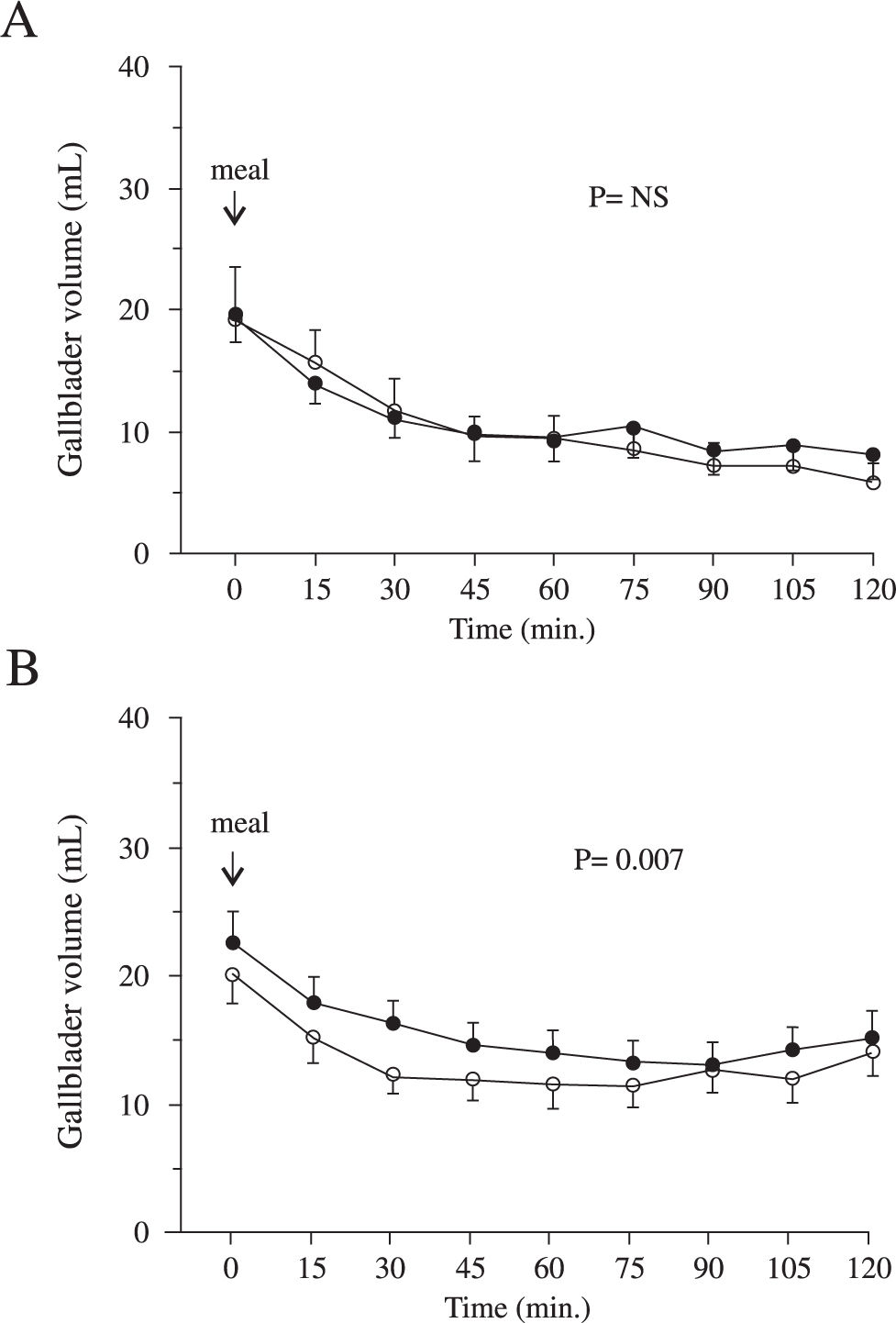
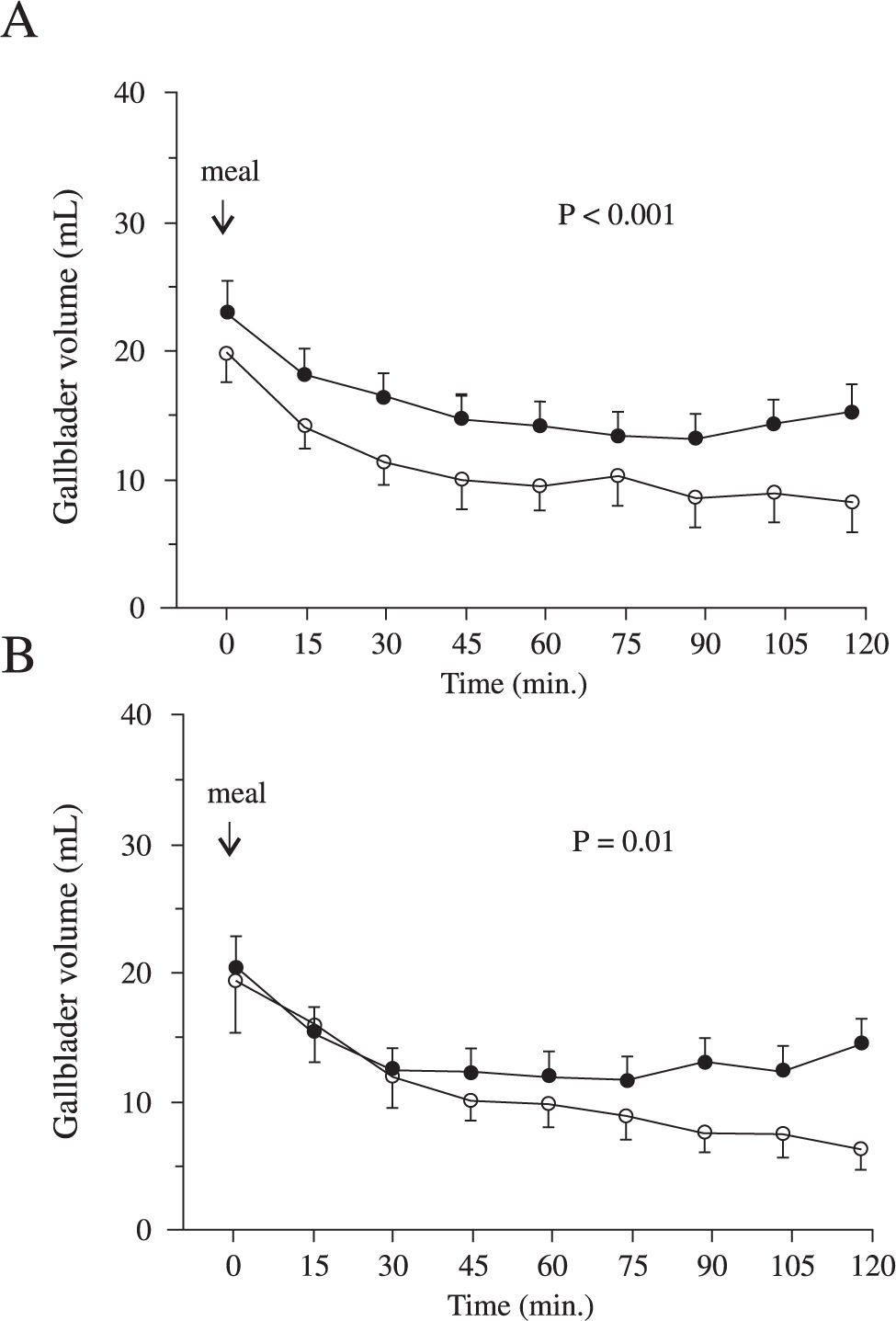
In healthy subjects, fasting volumes determined by 2D and 3D ultrasonography were virtually identical (20 ± 2 vs 19 ± 4 mL, P = NS). Minimal residual volumes were also comparable (8 ± 2 vs 6 ± 4 mL, P = NS). No differences were found between 2D and 3D ultrasonography in other gallbladder contraction parameters (not shown). Postprandial contraction curves in healthy subjects were also comparable as determined by 2D and 3D ultrasonography (Figure 3A).
 Fasting gallbladder volumes and postprandial contraction curves in healthy subjects determined by 2-dimensional (•) and 3-dimensional ultrasonography (o) are virtually identical. B) Fasting and postprandial gallbladder volumes in gallstone carriers determined by 2-dimensional (•) and 3-dimensional ultrasonography (o). Postprandial volumes were larger by 2D ultrasonography in gallstone carriers.")
2-vs. 3-dimensional ultrasonography in healthy subjects and gallstone carriers. A) Fasting gallbladder volumes and postprandial contraction curves in healthy subjects determined by 2-dimensional (•) and 3-dimensional ultrasonography (o) are virtually identical. B) Fasting and postprandial gallbladder volumes in gallstone carriers determined by 2-dimensional (•) and 3-dimensional ultrasonography (o). Postprandial volumes were larger by 2D ultrasonography in gallstone carriers.
In gallstone carriers, fasting gallbladder volumes determined by 3D ultrasonography were slightly lower than by 2D ultrasonography, without reaching significance (20 ± 2 vs 23 ± 3 mL, P = NS). Minimal residual gallbladder volumes in gallstone carriers exhibited a similar tendency (9 ± 1 vs 11 ± 1 mL, P = NS). Postprandial contraction curves indicated smaller gallbladder volumes during the whole postprandial period in case of 3D ultrasonography compared to 2D ultrasonography, as depicted in Figure 3B (P = 0.007). Other gallbladder contraction parameters were not significantly different (not shown).
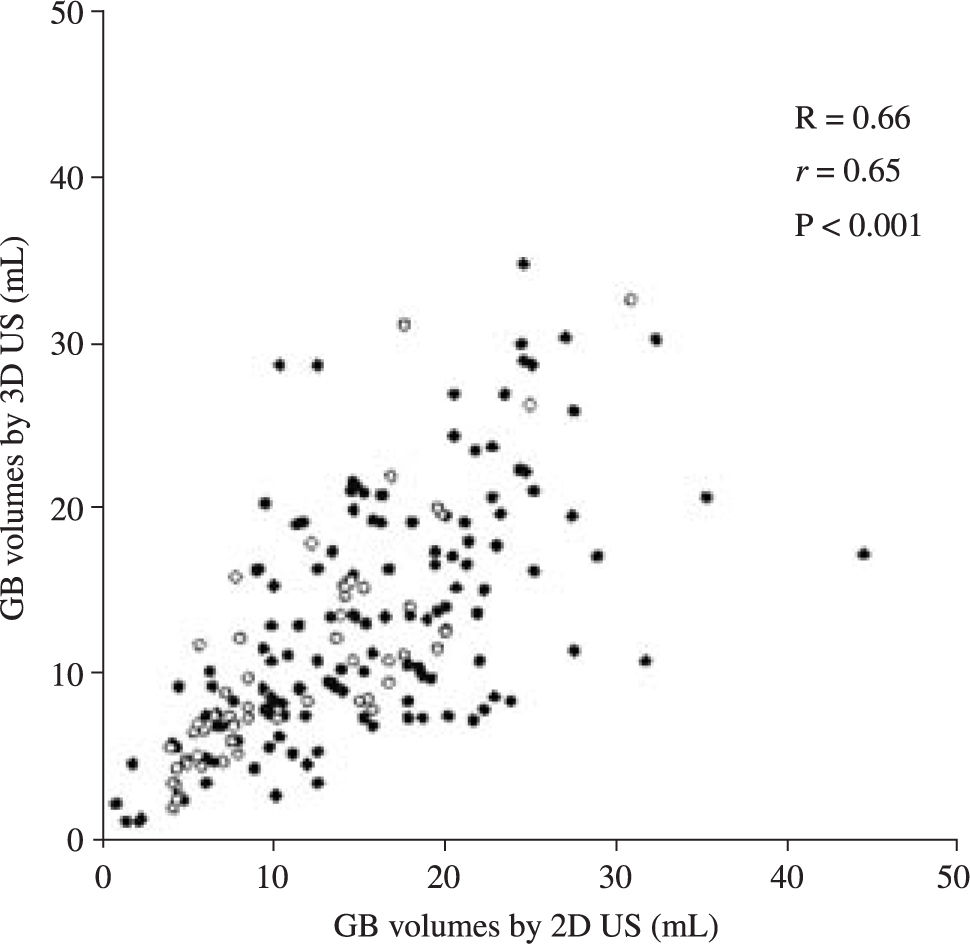
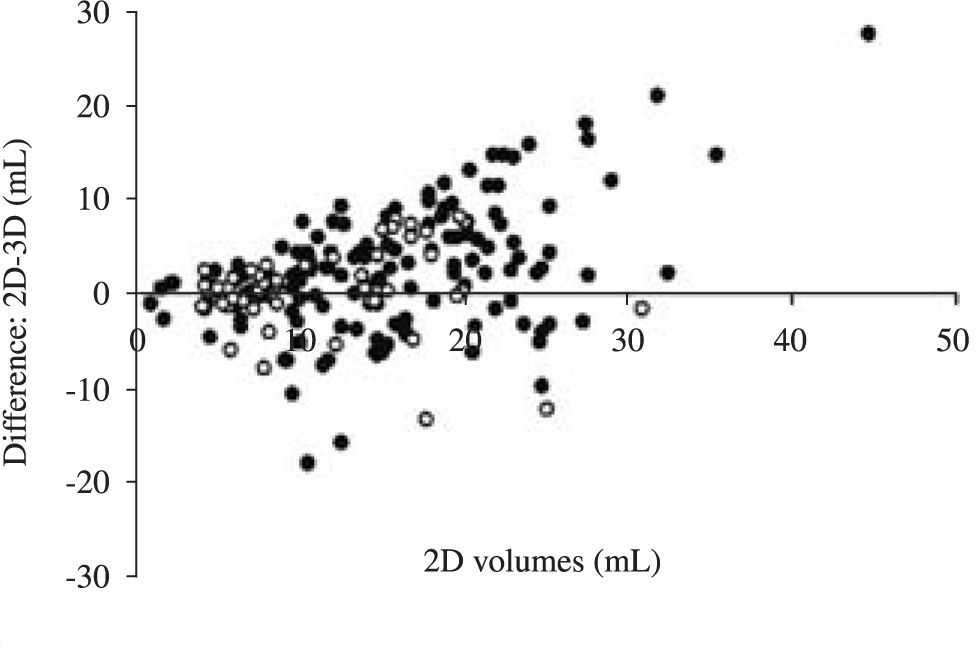
Volumes obtained by 2D and 3D ultrasonography were significantly correlated (R = 0.66, r = 0.65, P < 0.001:Figure 4). InFigure 5, differences between volumes of the same gallbladders according to 2D and 3D ultrasonography are given as a function of volumes according to 2D ultrasonography. This is the most appropriate way to show potential differences between methods that are highly correlated. Especially at higher gallbladder volumes and in the gallstone group, gallbladder volumes by 3D ultrasonography appear smaller than corresponding volumes by 2D ultrasonography.
 and gallstone carriers (•) are significantly correlated. GB, gallbladder.")
 and gallstone carriers (•) according to 2-dimensional and 3-dimensional ultrasonography are given as a function of volumes according to 2 dimensional ultrasonography. Especially at higher gallbladder volumes and in the gallstone group, gallbladder volumes by 3-dimensional ultrasonography appear smaller than by 2-dimensional ultrasonography.")
2-vs. 3-dimensional ultrasonography Blant-Altman plot. Differences between volumes of the same gallbladders in healthy subjects (o) and gallstone carriers (•) according to 2-dimensional and 3-dimensional ultrasonography are given as a function of volumes according to 2 dimensional ultrasonography. Especially at higher gallbladder volumes and in the gallstone group, gallbladder volumes by 3-dimensional ultrasonography appear smaller than by 2-dimensional ultrasonography.
With both methods, fasting and minimal residual gallbladder volumes tended to be larger in gallstone carriers than in healthy subjects. Also, maximal decreases of gallbladder volumes in mL and % of fasting volumes were smaller in the gallstone group (not shown). Overall gall-bladder contraction curves according to both methods revealed clearly larger postprandial volumes in gallstone carriers (Figure 6).
 and gallstone carriers (•) determined by 2-dimensional (A) or 3-dimensional ultrasonography (B) are shown. With both methods, gallstone carriers exhibit larger postprandial gallbladder volumes than healthy subjects, indicating impaired gallbladder contractility.")
Gallbladder volumes of healthy subjects vs gallstone carriers by 2-and 3-dimensional ultrasonography. Fasting and postprandial gallbladder volumes in healthy subjects (o) and gallstone carriers (•) determined by 2-dimensional (A) or 3-dimensional ultrasonography (B) are shown. With both methods, gallstone carriers exhibit larger postprandial gallbladder volumes than healthy subjects, indicating impaired gallbladder contractility.
Impaired gallbladder emptying plays an important role in cholesterol gallstone formation. Several methods have been used to determine gallbladder emptying, such as oral cholecystography,1199Tc-HIDA scanning12,13 and 2D ultrasonography with ellipsoid14 and sum of cylinders method.15,16 The current study evaluated the feasibility of 3D ultrasonography for determining gallbladder volumes and compared results to 2D ultrasonography with the sum of cylinders method, both in vivo and in vitro. In vitro measurements revealed that both methods estimated true volumes adequately. Also in healthy subjects, no differences were found between both methods. In gallstone patients however, postprandial gallbladder volumes measured by 3D ultrasonography were smaller than those measured by 2D ultrasonography. Our impression is, that differences may be explained by difficulties outlining the gallbladder wall correctly during 3D ultrasonography: due to the presence of gallstones, the gallbladder wall was not always entirely visible after re-sampling. On the other hand, overestimation of gallbladder volumes by 2D ultrasonography cannot be excluded. In vitro measurement of water-filled balloons by 2D ultrasonography showed indeed some overestimation compared to true volumes. Compared to 2D ultrasonography, 3D ultra-sonography of gallbladder volumes is more time-consuming, and resolution may be lost during re-sampling of computerized 3D ultrasonography data. Furthermore, obesity may reduce the feasibility of 3D ultrasonography more than 2D ultrasonography, since a sweep over a larger area may be more difficult than a static measurement in obese subjects.
Limited data are available on gallbladder volume measurements by 3D ultrasonography. Hashimoto et al. evaluated gallbladder volumes measured by 3D ultrasonography in vitro and in vivo, and compared this method to 2D ultrasonography.20In vivo, gallbladder volumes of fourteen male healthy volunteers were comparable as measured by 2D and 3D ultrasonography, in agreement with the current results. In a study by Yoon et al., 3D ultrasonography was compared to oral cholecystography for visualization of the gallbladder and gallbladder stones.21 In some gallstone carriers, the gallbladder showed no opacification, and not all gallbladder stones were visualized by oral cholecystography. This was however always the case when 3D ultrasonography was applied. Gallbladder volumes were not obtained by oral cholecystography in that study.
Regardless the ultrasonography method used, we found significantly larger postprandial gallbladder volumes in gallstone patients than in healthy subjects, indicating impaired gallbladder motility in the gallstone group. Since comparing gallbladder contraction in gallstone patients and normal subjects was not the primary aim of our study, we did not match both groups for age and BMI. Nevertheless, these results are in agreement with many previous studies by our group and others.22-24
In conclusion, gallbladder volume measurements by 3-dimensional and 2-dimensional ultrasonography are strongly correlated. Nevertheless, in gallstone carriers, gallbladder volumes by 3-dimensional ultrasonography tend to be smaller than by 2-dimensional ultrasonography.



