




Abstracts from XVII Mexican Congress of Hepatology
Más datosThe "overlap syndrome" is a variant of autoimmune hepatitis (AIH) in addition to cholestatic liver disease. AIH can present concurrently with primary biliary cholangitis (PBC) 7% to 13%, primary sclerosing cholangitis (PSC) 6% to 11% or autoimmune cholangitis (AIC) 3% to 9%, the rarest and associated with a poor prognosis. Diagnosis requires biochemical alteration, immunological studies and biopsy, plus the exclusion of viral, toxic, metabolic and hereditary etiologies. Therapy, including corticosteroids, ursodeoxycholic acid and immunosuppressants, should be individualized and guided by the severity of the cholestasis findings.
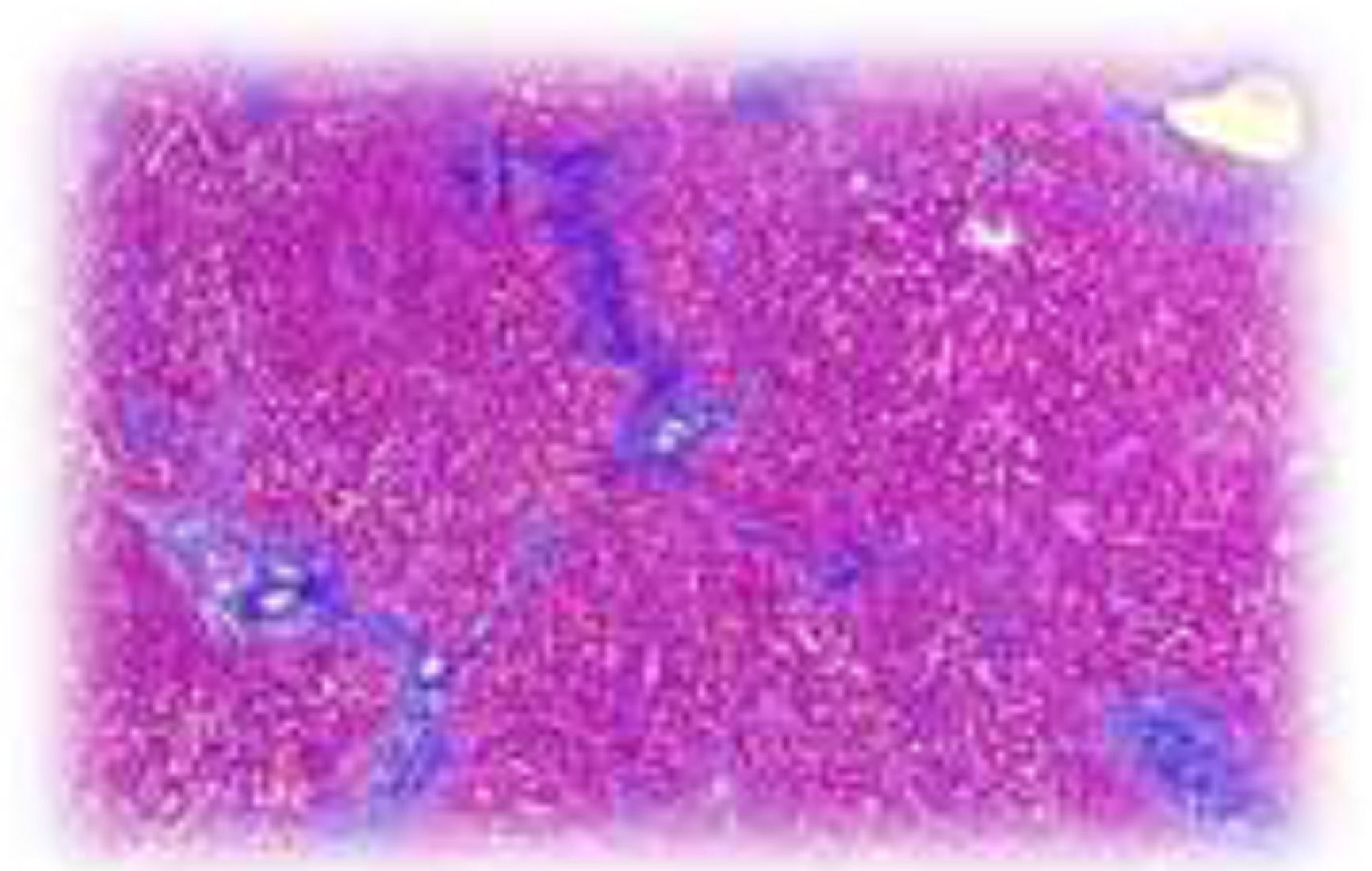
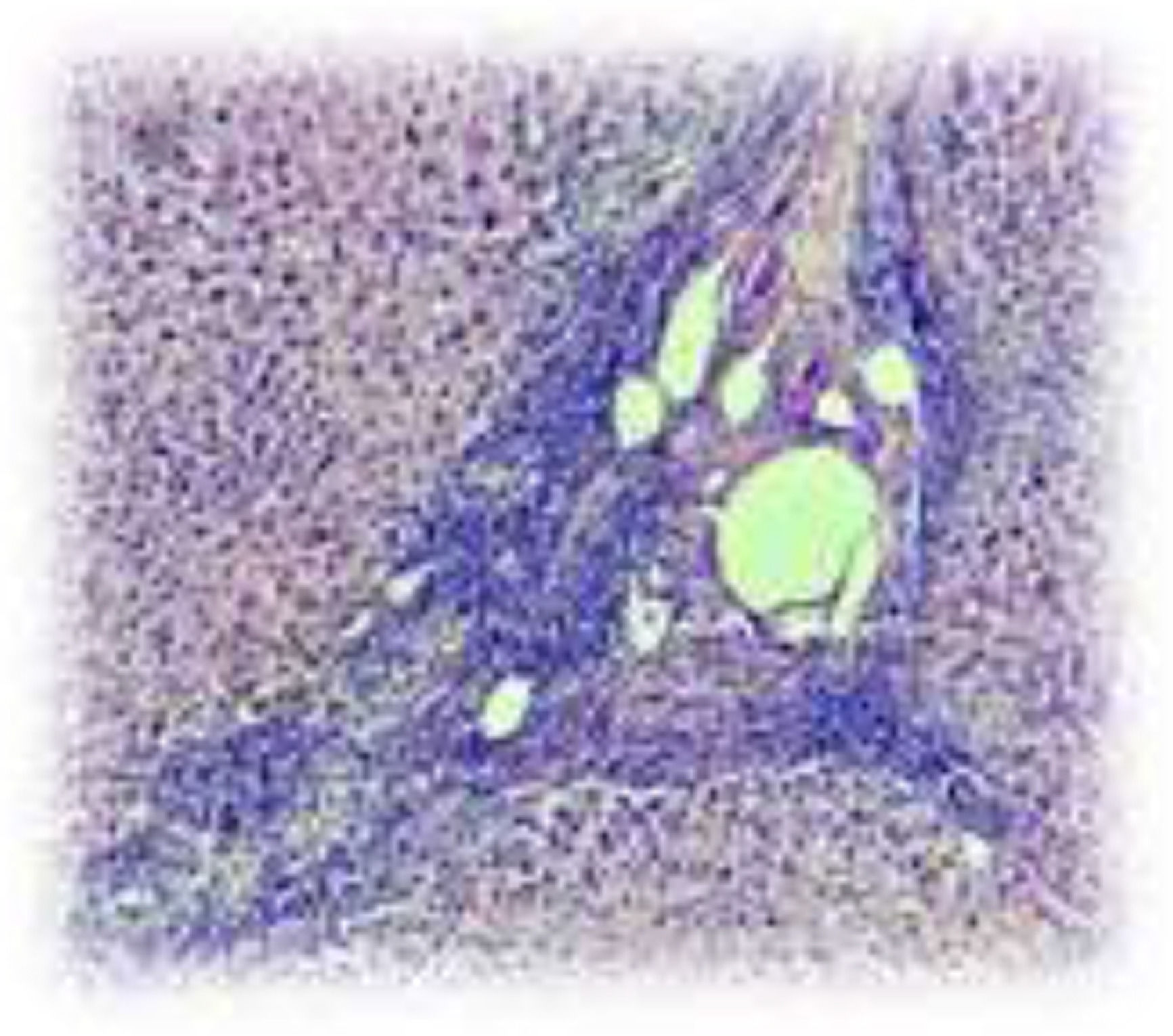
Materials and Methods66-year-old female. She presented in 2018 with the detection of hepatic steatosis, a weight loss of 32 kg in 2 years. Asthenia, adynamia, pruritus and scleral jaundice progressing to generalized. In laboratories: BT 11.37 (BI 8.5), AST 187, ALT 148, GGT 1761, FA 1819, ANAs positive anti centromere 1:40 and Hep-2 cells 1:640, cholangioresonance without data of CEP. Treatment with ursodeoxycholic acid was started, with no response, and a liver biopsy was performed compatible with HAI+CAI, Fig. 1 and 2. We started therapy with prednisone and azathioprine.
ConclusionsRecognizing that AIH and IAC are diseases with high morbidity that progress to chronic liver damage with fibrosis and cirrhosis, their early identification would help in the establishment of timely and effective treatment.
FundingThe resources used in this study were from the hospital without any additional financing
Declaration of interestThe authors declare no potential conflicts of interest.

Fig.1: Masson's trichrome stain: fibrous portal expansion with the formation of incomplete portal-port bridges.

Fig. 2: No bile duct, granulomatous inflammation with inflammatory infiltrate predominantly lymphocytes, plasma cells and epithelioid macrophages that exceed the limiting plaque. Intracellular cholestasis.



