


Rheumatoid arthritis (RA) is a common chronic, autoimmune disorder, that affects several tissues and organs, principally synovial joints. RA can damage virtually any extraarticular tissue due to a systemic proinflammatory state.1 The prevalence of RA is of 0.5–1.0% in industrialized countries,2 Pelaez-Ballestas et al.3 found a prevalence of 0.7–2.8% in Mexican patients. Rheumatoid nodules present as a local swelling or tissue lump, which occurs almost exclusively in association with RA. Nodules are seen in the heart and usually they are asymptomatic and rarely need surgical intervention.4 Cardiovascular disease is considered an extraarticular manifestation and a major predictor of poor prognosis, but the excess mortality is due largely to ischemic heart disease and stroke.5 Clinically significant valvular disease attributable to RA appears to be uncommon. Echocardiography is a very important tool in detecting even minor cardiac muscle, valvular and pericardial involvement, also in asymptomatic individuals.4,6
The aim of this study is to present a case of a woman in the sixth decade of life with multivalvular nodules most marked on the right side of the heart.
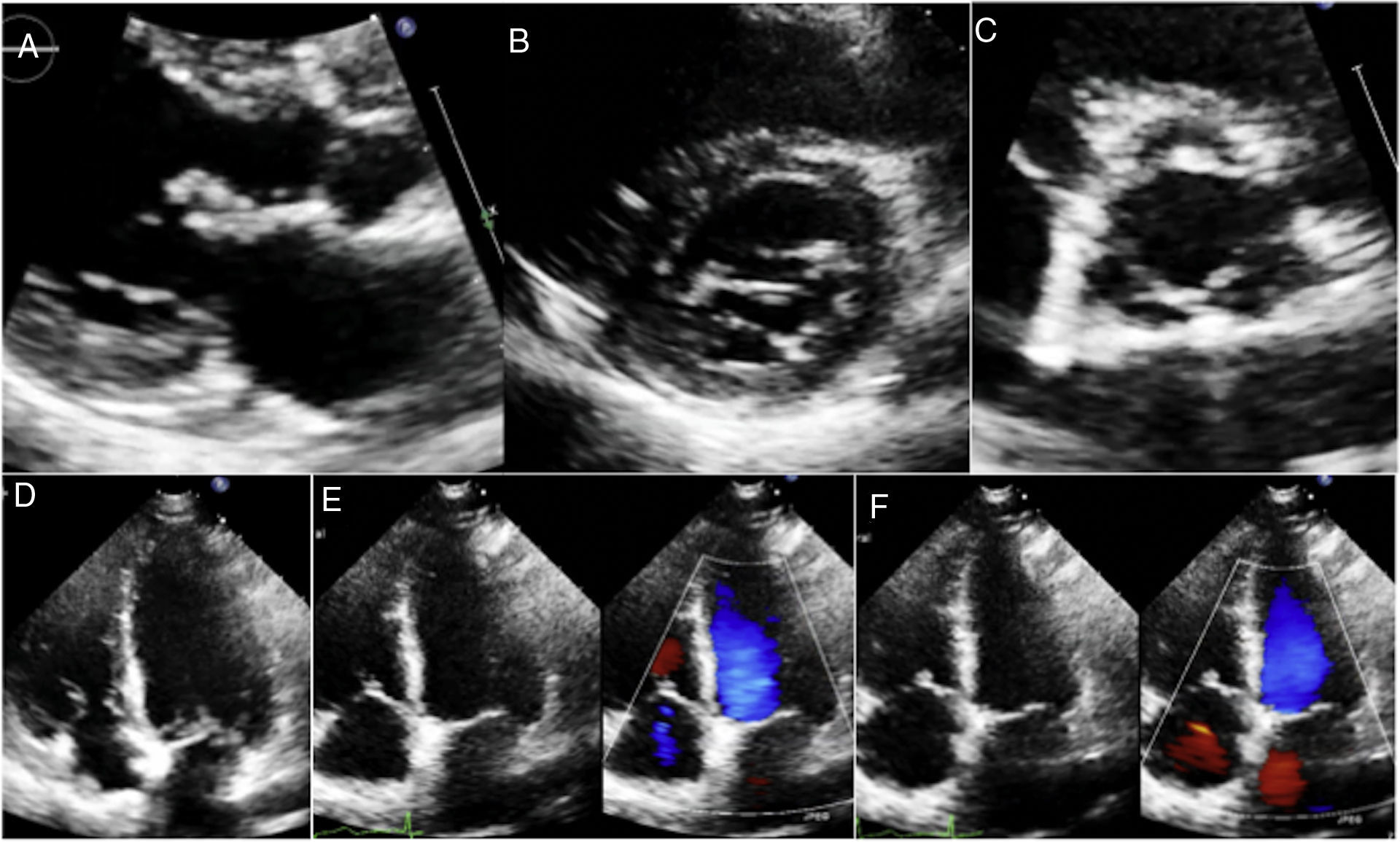
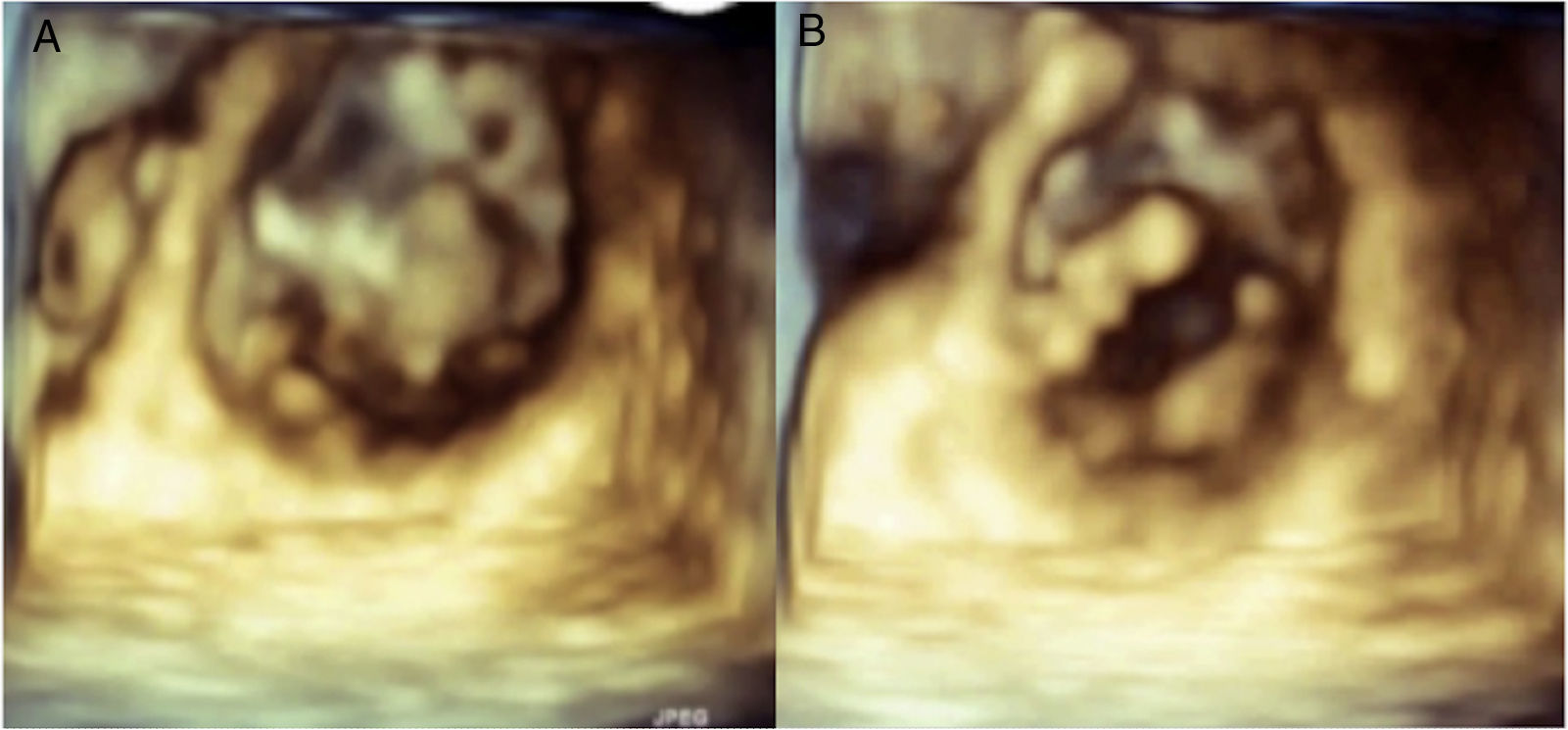
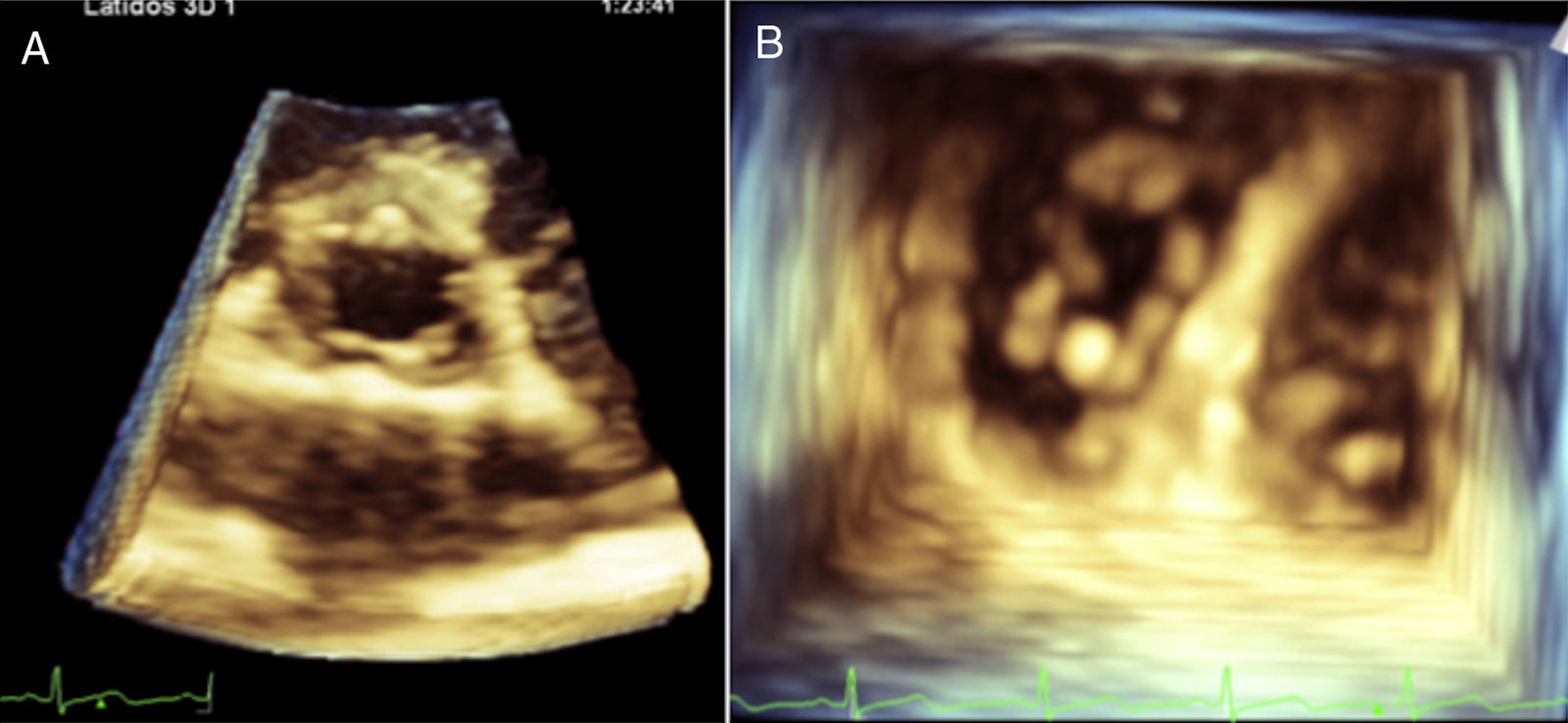
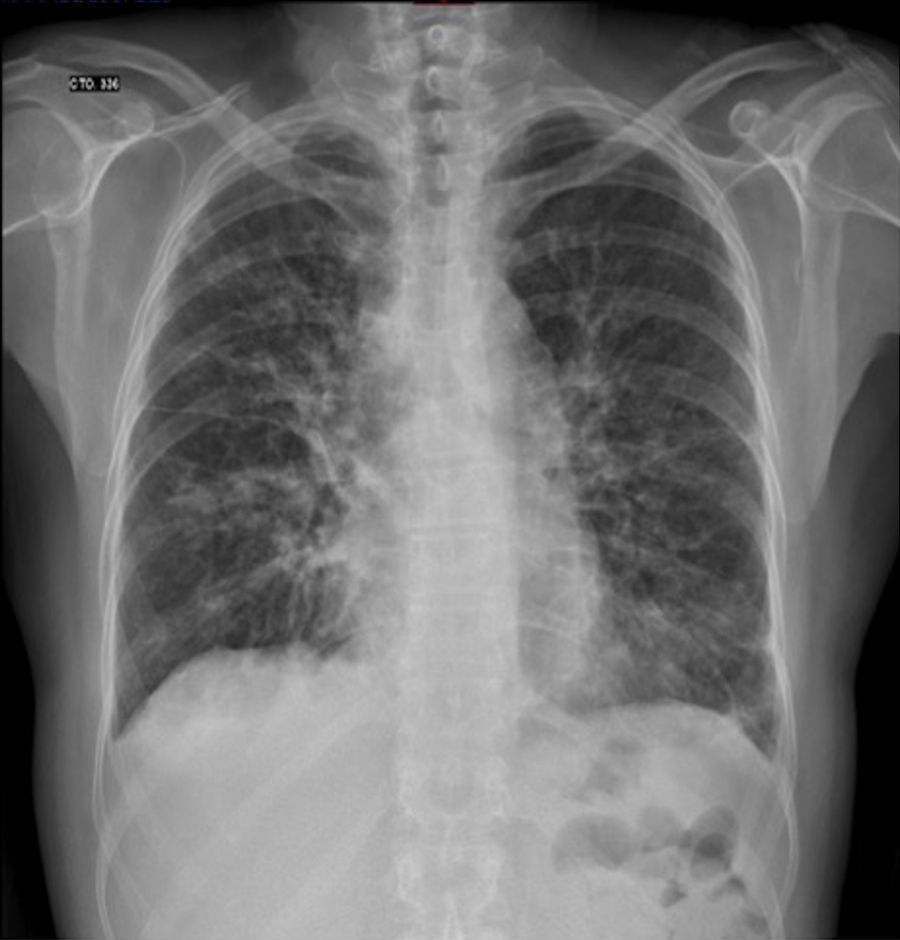
MLG is a female 58 years old with a history of rheumatoid arthritis diagnosed in December 2011 based on elevated rheumatoid factor, erythrocyte sedimentation rate and C-reactive protein, the presence of anticyclic citrullinated peptide antibody (anti-CCP), and bony erosions in the hands. She initially received treatment with immunosuppressors (methotrexate) and later with biological (abatacept) therapy with improvement and remission of the disease. She presented to the emergency room of our institution with a 3 weeks-history of a progressive dyspnea from great to moderate efforts, palpitations, fever (38.8°C), malaise, dry cough and headache. On examination, she was tachycardic (HR: 101/min), with oxygen desaturation (P02=70%) and had bibasilar lung rales. The laboratory analysis showed leukocytosis (21.4×103/m3) and mild anemia (Hb – 12.7g/dL and Htc – 40%). Blood cultures were negative. The chest computed tomography showed areas of bilateral alveolar occupation in relation to acute inflammatory process without pleural effusion. The transthoracic bidimensional (Fig. 1A–F) and three-dimensional echocardiogram revealed nodular thickening on the both mitral leaflets and in the subvalvular apparatus of the mitral valve without mitral regurgitation (Fig. 2A and B), small nodules in the aortic leaflets (Fig. 3A and prominent nodules on the tricuspid valve with mild tricuspid regurgitation (Fig. 3B), mild pulmonary hypertension, left ventricular diastolic dysfunction type I and normal left ventricular systolic function. The patient was treated with intravenous steroids and broad spectrum antibiotics with clinical improvement, but without changes in the valvular lesions. Actually she is in NYHA functional class I and the chest radiograph after the resolution of infectious process showed interstitial lung bilateral thickening and reticulonodular parahiliar and basal pattern, the left cardiac profile is abnormal and the aorta unrolled (Fig. 4).
, aortic valve (C) and tricuspid valve (D,E). Mild tricuspid regurgitation was found with color flow (E,F).")
 and diastole (B), showing nodular thickening in both leaflets.")
. Transthoracic three-dimensional ventricular view of the tricuspid valve in diastole, showing prominent nodules in their cusps (B).")
.")
Among those extra-articular features of RA are cardiovascular diseases, including pericarditis, myocardial disease, coronary vasculitis, diastolic dysfunction, accelerated atherosclerotic disease and valvular lesions.7 In the literature the prevalence of RA valvular heart disease varies from 3% to 70%.8 Valvular lesions in RA result from non specific inflammatory process in the valvular base followed by fibrosis and, sometimes, calcification. Rheumatoid granulomata are more specific findings that can be found within cusps causing valvular insufficiency.8 In a study of 184 patients with RA, the valvular lesions were monovalvar and the aortic valve was the most affected.4 In comparison to this study, our case is very rare, because it had multivalvular cardiac nodules, small in aortic valve, of moderate size in mitral leaflets with involvement of mitral apparatus and more prominent in tricuspid valve.
However, at least 3 reasons are relevant for searching these findings: (1) these patients are prone to bacterial endocarditis; (2) some of the valvular lesion may cause rapid hemodynamic abnormalities requiring surgical treatment; (3) valvular disease may act as source of thromboembolic material causing ischemic vascular lesions and (4) rheumatoid nodules can cause also complete atrioventricular block.9
Valvular heart lesions associated with RA is described in pathologic studies as valve nodules and leaflet fibrosis that may extend to valve rings and subvalvular apparatus, without commisures and cusps fusion and cause valve regurgitation.6 Rheumatic fever instead leads to commissural fusion, valve thickening, and calcification with abnormal motion of the leaflets, prominent thickening of subvalvular apparatus just below the valve and shortening of chordal structures.10
Actually, three-dimensional echocardiography has been conceived as one of the most promising methods for the diagnosis and follow-up of valvular heart disease. In particular, for mitral valve diseases, this new approach has proven to be the most unique, powerful, and convincing method for understanding the complicated anatomy and dynamism of the mitral valve and also of the other cardiac valves.11 This technique should be performed in RA, because the resolution of the nodules is very clear as we observed in our patient. It has been shown that untreated systole in patients with RA is an important problem and joint efforts of rheumatologists and cardiologists may help to improve the cardiovascular morbidity and mortality in RA.5,8
This case highlights that RA granulomatous inflammation may cause multivalvular lesions, which is an extra-articular manifestations with poor prognosis. Our findings underscore the importance of three-dimensional echocardiographic assessment at least in clinical research when RA patients are involved.
List of abbreviationsRA rheumatoid arthritis anticyclic citrullinated peptide antibody New York Heart Association
OBG have been participated in the interpretation of the images and in the review of the literature, MES have been involved in revising critically the manuscript for important intellectual content, KVZ have been participated in the review of the literature, ELH have given final approval of the version to be published and NEZ have been involved in the conception, design, interpretation of data and in drafting the manuscript and have given final approval of the version to be published.
FundingNo grants or industrial support.
ConsentWritten informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Conflict of interestThe authors declare no conflict of interest.