





To explore the factors related to health-promoting lifestyles of the elderly based on social-ecosystem theory.
DesignA cross-sectional survey study was carried out to include 627 elderly people in communities in three cities of Hebei Province (Shijiazhuang, Tangshan, and Zhangjiakou) from October 2021 to January 2022 for questionnaire survey (601 validly returned cases).
VenueThree cities of Hebei Province (Shijiazhuang, Tangshan, and Zhangjiakou).
Participants627 elderly people.
InterventionsA cross-sectional survey study.
Main measurementsThe questionnaire survey was conducted by using the general demographic data, health promotion life scale, frailty scale, general self-efficacy scale, health engagement scale, General Self-Efficacy Scale, The family Adaptability, Partnership, Growth, Affection, and Resolve scale, and Perceived Social Support Scale.
ResultsThe total health promotion lifestyle score for the elderly was 100.20±16.21, which was at the lower limit of the good level, with the highest mean score for nutrition (2.71±0.51) and the lowest mean score for physical activity (2.25±0.56). Stepwise linear regression showed that exercise frequency (95% confidence interval (CI) 1.304–3.885), smoking status (95% CI −4.190 to −1.556), self-efficacy (95% CI 0.071–0.185), health management (95% CI 0.306–0.590), frailty (95% CI −3.327 to −1.162) in the microsystem, marital status (95% CI 0.677–3.660), children's attention to the elderly health (95% CI 4.866–11.305), family care in the mesosystem (95% CI 1.365–4.968), and pre-retirement occupation (95% CI 2.065–3.894), living area (95% CI 0.813–3.912), whether receive community-based chronic disease prevention and management services (95% CI 2.035–8.149), social support (95% CI 1.667–6.493) in the macrosystem were the main factors affecting health promotion of life in the elderly (P<0.05). Hierarchical regression analysis showed the microsystem accounted for 17.2%, the mesosystem accounted for 7.1%, and the macrosystem accounted for 11.4%.
ConclusionThe health promotion lifestyle of the elderly in Hebei Province was at the lower limit of good level. Among them, exercise frequency, children's attention to the elderly health, and pre-retirement occupation played a major role in relation to the health-promoting lifestyle of the elderly. Hence, it needs the joint action of individuals, families, and society to promote the elderly to adopt the health promotion lifestyle and realize healthy aging.
Explorar los factores relacionados con los estilos de vida saludables de adultos mayores a partir de la teoría del ecosistema social.
DiseñoSe realizó un estudio de encuesta transversal para incluir a 627 ancianos de la comunidad de tres ciudades de la provincia de Hebei (Shijiazhuang, Tangshan y Zhangjiakou) de octubre de 2021 a enero de 2022 para encuesta por cuestionario (601 casos válidos).
LugarTres ciudades de la provincia de Hebei (Shijiazhuang, Tangshan y Zhangjiakou).
ParticipantesSeiscientos veintisiete (627) ancianos.
IntervencionesEstudio transversal y de encuesta.
Principales medidasLa encuesta se realizó utilizando los datos demográficos generales, la escala de promoción de la salud de vida, la escala de fragilidad, la escala de autoeficacia general, la escala de compromiso con la salud, la escala de autoeficacia general, la escala de adaptabilidad familiar, asociación, crecimiento, afecto y resolución y la escala de apoyo social percibido.
ResultadosLa puntuación total de estilo de vida en promoción de la salud para los ancianos fue de 100,20 ± 16,21, que se sitúen en el límite inferior del nivel bueno, con la mayor puntuación media para nutrición (2,71 ± 0,51) y la menor puntuación media para actividad física (2,25 ± 0,56). La regresión lineal por pasos mostró que la frecuencia de ejercicio (intervalo de confianza del 95% [IC 95%] 1,304 – 3,885), el estado de tabaquismo (IC 95% -4,190 – -1,556), la autoeficacia (IC 95% 0,071 – 0,185), el manejo de la salud (IC 95% 0,306 – 0,590), la fragilidad (IC 95% -3,327 – -1,162) en el microsistema, el estado civil (IC 95% 0,677 – 3.660), la atención de los niños a la salud de los ancianos (IC 95% 4,866 – 11,305), el cuidado familiar en el mesosistema (IC 95% 1,365 – 4,968) y la ocupación previa a la jubilación (IC 95% 2,065 – 3,894), área de residencia (IC 95%: 0,813 – 3,912), recibir servicios comunitarios de prevención y manejo de enfermedades crónicas (IC 95%: 2,035 – 8,149), apoyo social (IC 95%: 1,667 – 6,493) en el macrosistema fueron los principales factores que afectaron la promoción de la salud en los ancianos (p < 0,05). El análisis de regresión jerárquica mostró que el microsistema representaba 17,2%, el mesosistema 7,1% y el macrosistema 11,4%.
ConclusiónEl estilo de vida de promoción de la salud de los ancianos de la provincia de Hebei estaba en el límite inferior de buen nivel. Entre ellos, la frecuencia de ejercicio, la atención de los niños a la salud de las personas de edad y la ocupación previa a la jubilación desempeñaron un papel importante en relación con el estilo de vida que promueve la salud de las personas de edad. Por lo tanto, se necesita la acción conjunta de los individuos, las familias y la sociedad para promover que los ancianos adopten el estilo de vida de promoción de la salud y tengan un envejecimiento saludable.
By 2020, the elderly population aged 60 and above account for 18.7% of the total population in China.1 According to statistics, China has the largest elderly population in the world,2 with a rapid aging rate,3 implying that the problem of population aging in China is getting serious, which has loaded a heavy burden on medical care and the economy, thus how to move closer to the achievement of healthy aging has become one of the key development directions for health projects in China. Among the coping strategies, research to help the elderly maintain healthy lifestyles and behaviors guided by the concept of health promotion has been spotlighted, with the results confirming that maintaining healthy lifestyles and behaviors can delay the diseases and disabling effects of aging,4 making it the most cost-effective way to achieve healthy aging and improve the quality of life.5 But due to the geographical influence and economic level, levels and associated factors of health promotion lifestyle vary substantially among regions, and it is a wide consensus that gender, self-efficacy, social support, and exercise frequency are the associated factors of the adoption of health promotion lifestyle by the aged people.5,6
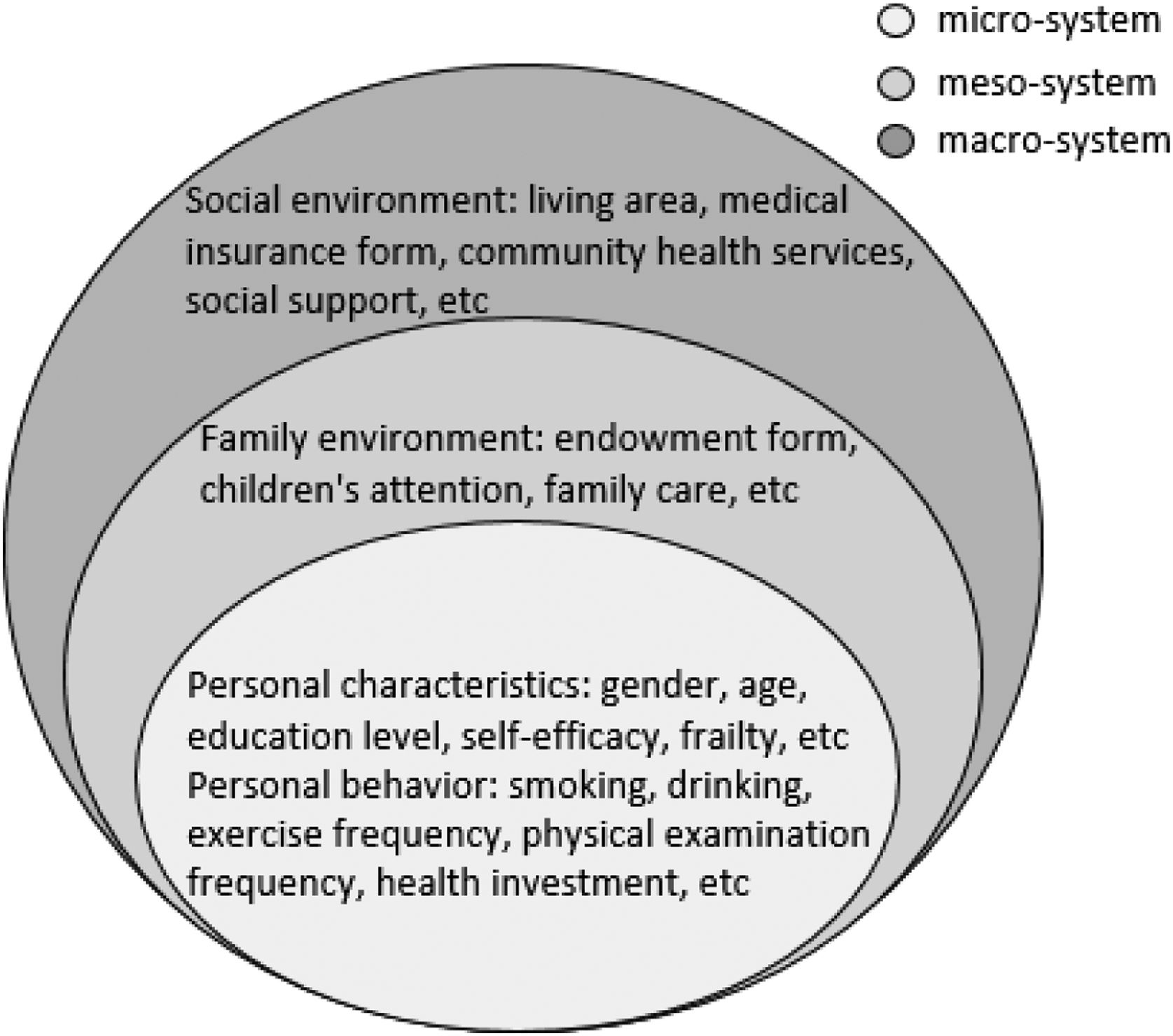
Bronfenbrenner's social ecosystem theory is based on systems theory, sociology, and ecology, and examines individual behavior as influenced by and interacting with the social environment.7 This theory considers the social environment in which people live (such as family, group or community) as a social ecosystem, and the behaviors adopted by individuals are significantly influenced by this system, and the theory emphasizes the interaction between individual development and the surrounding environment. Through continuous development, this theory can now be divided into micro, meso, and macro systems.8,9 Social ecosystem theory has now been used by a growing number of authors to examine individual and environmental factors associated with healthy aging.10 For example, Jasmine C. Mah et al.11 conducted an extensive overview of social factors associated with home care use among the elderly in communities in high-income countries based on social ecosystem theory, confirming that social factors do influence home care use. When the elderly face health challenges, not only themselves, but the entire social system in which they live is subject to multiple stressors. In addition, a study that included 485 elderly in Beijing, China, reported that social support networks play an important role in promoting healthy aging.12 A cross-sectional study that included 8526 elderly in Shanxi Province, China, found that social support is the strongest influence on the promotion of healthy lifestyle, followed by socioeconomic, health-related quality of life, and family support.13 There is a strong link between the individual development of the elderly and their surroundings, but few studies are focusing on the complete social ecosystem. This study summarized the social ecosystem theory based on the results of the existing literature, and the associated factors included in each system are shown in Fig. 1.3,14–16 Among them, the microsystem consists of personal characteristics and individual behaviors, including age, gender, and smoking status; the mesosystem is composed of the family environmental network, including form of elderly care and the children's attention; and the macrosystem contains social environment factors, such as the living area and the form of medical insurance. Based on this theory, this study intended to investigate the factors associated with the health promotion lifestyle of the elderly from three perspectives: microsystem, mesosystem and macrosystem, in order to provide realistic and guiding significance for the health management and promotion of the elderly in Hebei Province.
Material and methodsSample
This was a cross-sectional survey study. According to the general guideline and Stata software (version 15.0) that the sample size should be 5–10 times the maximum number of items (101),17 the required sample size was determined to be 505–1010 cases. According to the level of health and economic development in Hebei Province, three cities, Shijiazhuang (23 counties), Tangshan (18 counties), and Zhangjiakou (16 counties) were selected as the survey venues. Cross-sectional cluster random sampling method was used. Three counties were selected from each of the three cities as survey venues. 627 elderly people that were randomly recruited from communities in nine counties were selected for the study from October 2021 to January 2022 for questionnaire survey. Inclusion criteria were as follows: (1) Participants whose age≥60 years; (2) Participants who lived in the residential area for 3 years or more; (3) Participants who gave informed consent. Exclusion criteria were as follows: (1) Participants with speech and hearing communication impairment; (2) Participants with a history of mental illness, cognitive impairment, or dementia; (3) Participants with severe cardiac insufficiency, respiratory failure, and other major diseases unable to participate.
Instruments and variables- (1)
General demographic data were obtained using a self-defined basic information questionnaire, including gender, age, education level, pre-retirement occupation, living area, exercise frequency, and form of medical coverage.
- (2)
Health promoting lifestyle profile-II, revise (HPLP-II R): The HPLP-II R revised by Cao Wenjun et al.18 for the Chinese population was used, with 6 dimensions, namely nutrition, physical activity, health responsibility, interpersonal relations, stress management, and spiritual growth. The total score was 160, which was divided into 4 levels: poor (40–69), fair (70–99), good (100–129), and excellent (130–160). Each dimension was divided into 4 levels, with a total score of 24 for nutrition, 6–9 for poor, 10–14 for fair, 15–19 for good, and 20–24 for excellent. The total score for physical activity was 32, with 8–13 for poor, 14–19 for fair, 20–25 for good, and 16–32 for excellent. The total score of health responsibility was 44, with 11–18 for poor, 19–28 for fair, 29–35 for good, and 36–44 for excellent. The total score for interpersonal relations, stress management, and spiritual growth was 20, with 5–8 for poor, 9–11 for fair, 12–15 for good, and 16–20 for excellent. The Cronbach's α coefficient of the scale was 0.923.
- (3)
Frailty scale: Fatigue, Resistance, Ambulation, Illness, and Loss (FRAIL) for elderly translated by Wei Yin et al.19 was used, including 5 entries with a score of 0 for no and 1 for yes. The results could be classified as pre-frailty (1–2 points) and frailty (≥3 points). The Cronbach's α coefficient of the scale was 0.826.
- (4)
Health engagement scale: the health engagement scale developed by Zhu Zhiyong20 was used, including 3 dimensions (vigor, absorption, and dedication). The total score was 60 points, which was divided into high level (≥42 points), moderate level (18–41 points), and low level (<18 points). The Cronbach's α coefficient of the scale was 0.893.
- (5)
General Self-Efficacy Scale (GSES)21: The scale contained 10 items and 4-point Likert-type scale was used for each item. The results can be classified into very low (1–10 points), low (10–20 points), high (21–30 points), and very high (30–40 points) self-efficacy. The Cronbach's α coefficient of the scale was 0.816.
- (6)
Level of family function in caring: The family Adaptability, Partnership, Growth, Affection, and Resolve (APGAR) scale contained 5 items, and the family function can be leveled as good (7–10 points), moderate dysfunction (4–6 points), and severe dysfunction (0–3 points).22 The Cronbach's α coefficient of the scale was 0.771.
- (7)
Perceived Social Support Scale (PSSS): Chinese version translated by Jiang Qianjin23 was used. The scale was divided into 3 dimensions family support, friend support, and other support, with 7 response options for each item. The results were classified as low level (<36 points), medium level (<60 points), and high level (<80 points). The Cronbach's α coefficient of the scale was 0.934.
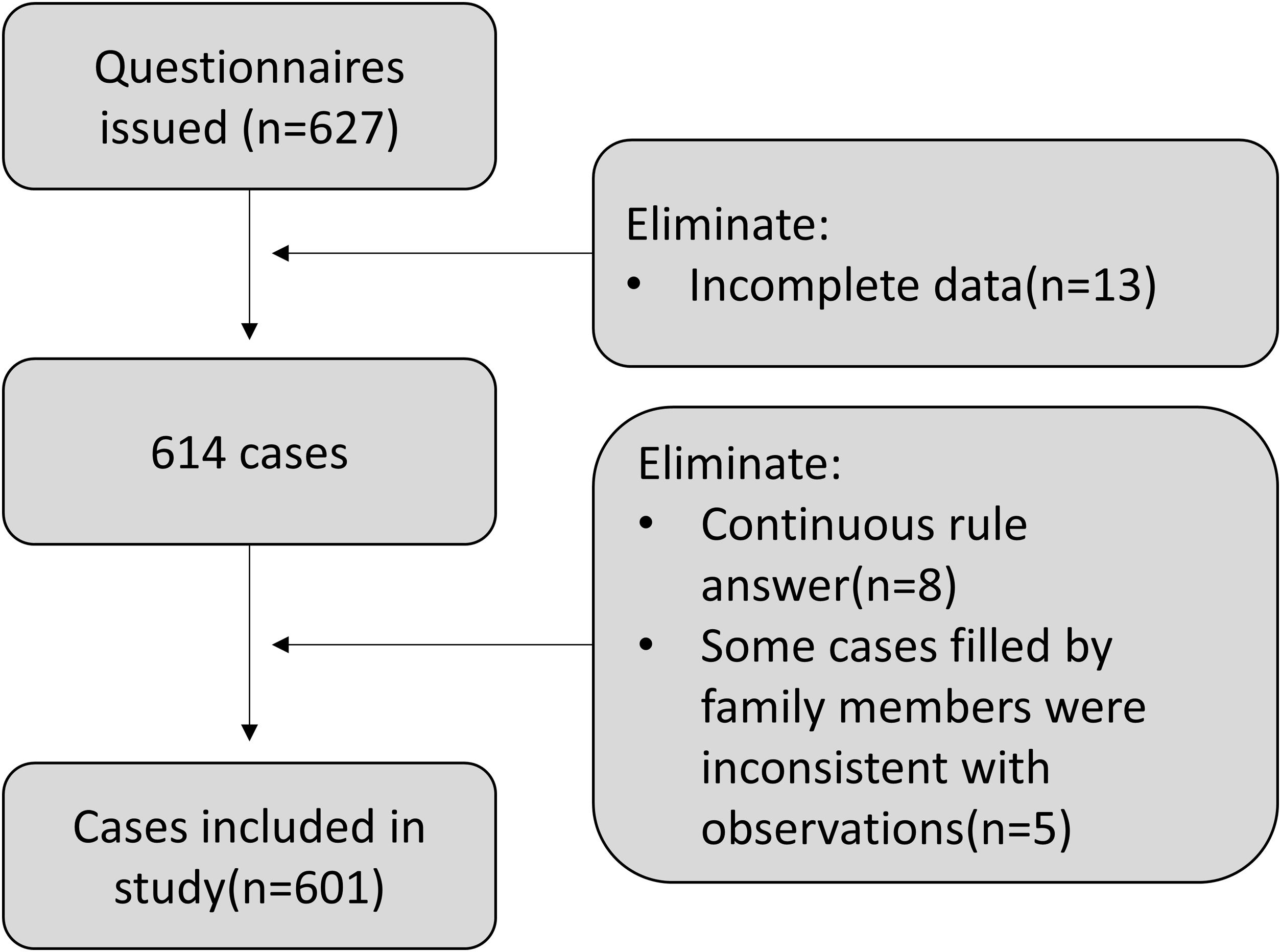
The questionnaires were distributed and collected by three uniformly trained investigators, and the purpose of this survey was fully explained to the study participants before the survey. After obtaining consent from study participants, the questionnaires were distributed to them face-to-face. The questionnaire took about 20–30min to complete. For those with reading or writing difficulties, the questionnaires could be filled out for them based on their answers. The questionnaires were collected on the spot after completion, and the privacy protection of the study participants was paid attention to throughout the process. The data were double-entered by two investigators, and the accuracy, logic and completeness of the entered data were reviewed to ensure the quality of data entry. A total of 627 questionnaires were distributed and 601 valid questionnaires were returned. Thirteen of them were excluded because they were incomplete, eight were excluded because of consecutive rules for filling in answers, and five were excluded because they were filled in by family members on their behalf, but the filling was not consistent with our observations and interviews, with a valid return rate of 95.85%.
Ethical considerationsThis study was approved by the Ethics Committee of North China University of Science and Technology (2021163).
Statistical methodsThe raw data were recorded in pairs on an Excel sheet, and SPSS 26.0 software was used for data analysis. The scores of each item and the total HPLP-II R scores of health promotion lifestyle of the elderly were expressed as (X¯±s), and the distribution of the health promotion lifestyle dimensional ranks was expressed as n (%). Stepwise multiple regression was used to screen associated factors of health promotion lifestyle (P<0.05), and hierarchical regression analysis was used to determine the values of the influence of each system on health promotion lifestyle. The test was at α=0.05, and P<0.05 indicated a statistically significant difference.
ResultsCurrent status of health promotion lifestyles of the elderly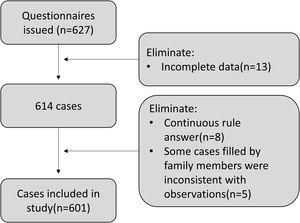
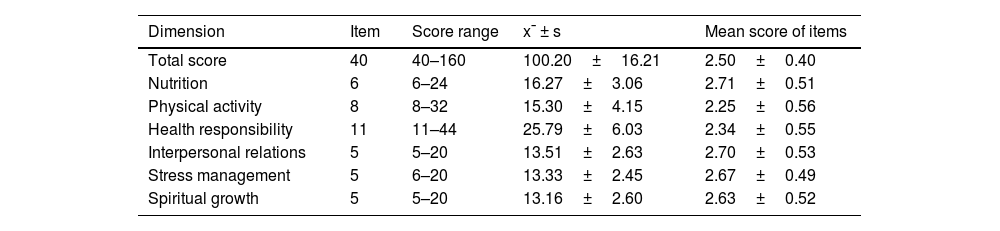
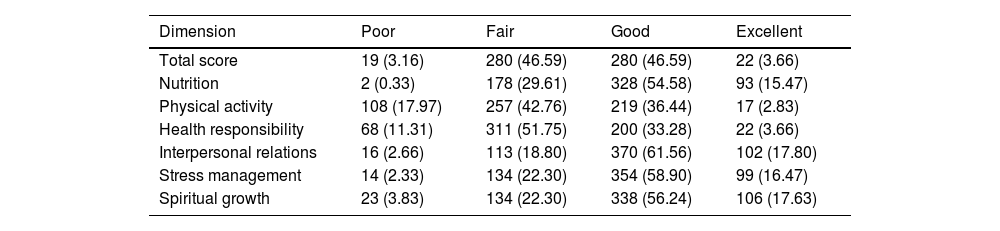
The mean score of health promotion life level of the study participants was 100.20±16.21, which was in the lower limit of good level overall, with good and excellent rates of 46.59% and 3.66%, respectively; the percentages of poor and fair were 3.16% and 46.59%, respectively. For the dimensional standard scores, dimensions were ranked by scores from highest to lowest as nutrition, interpersonal relations, stress management, spiritual growth, health responsibility, and physical activity. The detailed scores are listed in Table 1. The grades of each dimension are detailed in Table 2.
Health promotion life scale (revise) dimension scores of study participants (x¯ ± s).
| Dimension | Item | Score range | x¯ ± s | Mean score of items |
|---|---|---|---|---|
| Total score | 40 | 40–160 | 100.20±16.21 | 2.50±0.40 |
| Nutrition | 6 | 6–24 | 16.27±3.06 | 2.71±0.51 |
| Physical activity | 8 | 8–32 | 15.30±4.15 | 2.25±0.56 |
| Health responsibility | 11 | 11–44 | 25.79±6.03 | 2.34±0.55 |
| Interpersonal relations | 5 | 5–20 | 13.51±2.63 | 2.70±0.53 |
| Stress management | 5 | 6–20 | 13.33±2.45 | 2.67±0.49 |
| Spiritual growth | 5 | 5–20 | 13.16±2.60 | 2.63±0.52 |
Grade of health promotion lifestyle of study participants in different dimensions n (%).
| Dimension | Poor | Fair | Good | Excellent |
|---|---|---|---|---|
| Total score | 19 (3.16) | 280 (46.59) | 280 (46.59) | 22 (3.66) |
| Nutrition | 2 (0.33) | 178 (29.61) | 328 (54.58) | 93 (15.47) |
| Physical activity | 108 (17.97) | 257 (42.76) | 219 (36.44) | 17 (2.83) |
| Health responsibility | 68 (11.31) | 311 (51.75) | 200 (33.28) | 22 (3.66) |
| Interpersonal relations | 16 (2.66) | 113 (18.80) | 370 (61.56) | 102 (17.80) |
| Stress management | 14 (2.33) | 134 (22.30) | 354 (58.90) | 99 (16.47) |
| Spiritual growth | 23 (3.83) | 134 (22.30) | 338 (56.24) | 106 (17.63) |
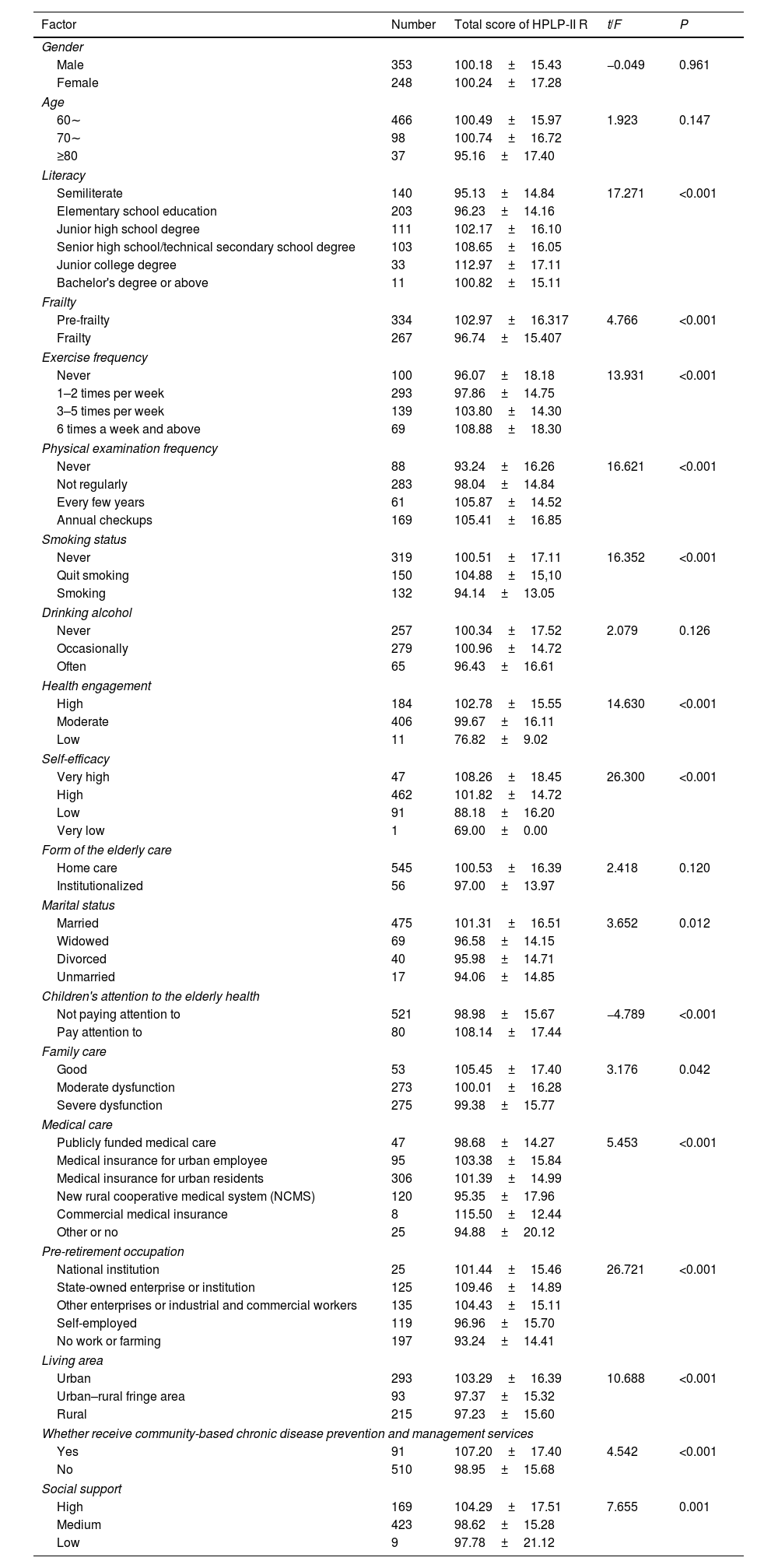
The results of univariate analysis showed that literacy, frailty, exercise frequency, physical examination frequency, smoking status, self-efficacy, and health engagement were statistically significant in the microsystem (P<0.05), marital status, children's attention to the elderly health, and family care in the mesosystem (P<0.05), and medical coverage, pre-retirement occupation, living area, whether receive community-based chronic disease prevention and management services, and social support in the macrosystem (P<0.05) were statistically significant, as detailed in Table 3.
Univariate analysis of health promotion lifestyles of study participants (x¯ ± s).
| Factor | Number | Total score of HPLP-II R | t/F | P |
|---|---|---|---|---|
| Gender | ||||
| Male | 353 | 100.18±15.43 | −0.049 | 0.961 |
| Female | 248 | 100.24±17.28 | ||
| Age | ||||
| 60∼ | 466 | 100.49±15.97 | 1.923 | 0.147 |
| 70∼ | 98 | 100.74±16.72 | ||
| ≥80 | 37 | 95.16±17.40 | ||
| Literacy | ||||
| Semiliterate | 140 | 95.13±14.84 | 17.271 | <0.001 |
| Elementary school education | 203 | 96.23±14.16 | ||
| Junior high school degree | 111 | 102.17±16.10 | ||
| Senior high school/technical secondary school degree | 103 | 108.65±16.05 | ||
| Junior college degree | 33 | 112.97±17.11 | ||
| Bachelor's degree or above | 11 | 100.82±15.11 | ||
| Frailty | ||||
| Pre-frailty | 334 | 102.97±16.317 | 4.766 | <0.001 |
| Frailty | 267 | 96.74±15.407 | ||
| Exercise frequency | ||||
| Never | 100 | 96.07±18.18 | 13.931 | <0.001 |
| 1–2 times per week | 293 | 97.86±14.75 | ||
| 3–5 times per week | 139 | 103.80±14.30 | ||
| 6 times a week and above | 69 | 108.88±18.30 | ||
| Physical examination frequency | ||||
| Never | 88 | 93.24±16.26 | 16.621 | <0.001 |
| Not regularly | 283 | 98.04±14.84 | ||
| Every few years | 61 | 105.87±14.52 | ||
| Annual checkups | 169 | 105.41±16.85 | ||
| Smoking status | ||||
| Never | 319 | 100.51±17.11 | 16.352 | <0.001 |
| Quit smoking | 150 | 104.88±15,10 | ||
| Smoking | 132 | 94.14±13.05 | ||
| Drinking alcohol | ||||
| Never | 257 | 100.34±17.52 | 2.079 | 0.126 |
| Occasionally | 279 | 100.96±14.72 | ||
| Often | 65 | 96.43±16.61 | ||
| Health engagement | ||||
| High | 184 | 102.78±15.55 | 14.630 | <0.001 |
| Moderate | 406 | 99.67±16.11 | ||
| Low | 11 | 76.82±9.02 | ||
| Self-efficacy | ||||
| Very high | 47 | 108.26±18.45 | 26.300 | <0.001 |
| High | 462 | 101.82±14.72 | ||
| Low | 91 | 88.18±16.20 | ||
| Very low | 1 | 69.00±0.00 | ||
| Form of the elderly care | ||||
| Home care | 545 | 100.53±16.39 | 2.418 | 0.120 |
| Institutionalized | 56 | 97.00±13.97 | ||
| Marital status | ||||
| Married | 475 | 101.31±16.51 | 3.652 | 0.012 |
| Widowed | 69 | 96.58±14.15 | ||
| Divorced | 40 | 95.98±14.71 | ||
| Unmarried | 17 | 94.06±14.85 | ||
| Children's attention to the elderly health | ||||
| Not paying attention to | 521 | 98.98±15.67 | −4.789 | <0.001 |
| Pay attention to | 80 | 108.14±17.44 | ||
| Family care | ||||
| Good | 53 | 105.45±17.40 | 3.176 | 0.042 |
| Moderate dysfunction | 273 | 100.01±16.28 | ||
| Severe dysfunction | 275 | 99.38±15.77 | ||
| Medical care | ||||
| Publicly funded medical care | 47 | 98.68±14.27 | 5.453 | <0.001 |
| Medical insurance for urban employee | 95 | 103.38±15.84 | ||
| Medical insurance for urban residents | 306 | 101.39±14.99 | ||
| New rural cooperative medical system (NCMS) | 120 | 95.35±17.96 | ||
| Commercial medical insurance | 8 | 115.50±12.44 | ||
| Other or no | 25 | 94.88±20.12 | ||
| Pre-retirement occupation | ||||
| National institution | 25 | 101.44±15.46 | 26.721 | <0.001 |
| State-owned enterprise or institution | 125 | 109.46±14.89 | ||
| Other enterprises or industrial and commercial workers | 135 | 104.43±15.11 | ||
| Self-employed | 119 | 96.96±15.70 | ||
| No work or farming | 197 | 93.24±14.41 | ||
| Living area | ||||
| Urban | 293 | 103.29±16.39 | 10.688 | <0.001 |
| Urban–rural fringe area | 93 | 97.37±15.32 | ||
| Rural | 215 | 97.23±15.60 | ||
| Whether receive community-based chronic disease prevention and management services | ||||
| Yes | 91 | 107.20±17.40 | 4.542 | <0.001 |
| No | 510 | 98.95±15.68 | ||
| Social support | ||||
| High | 169 | 104.29±17.51 | 7.655 | 0.001 |
| Medium | 423 | 98.62±15.28 | ||
| Low | 9 | 97.78±21.12 | ||
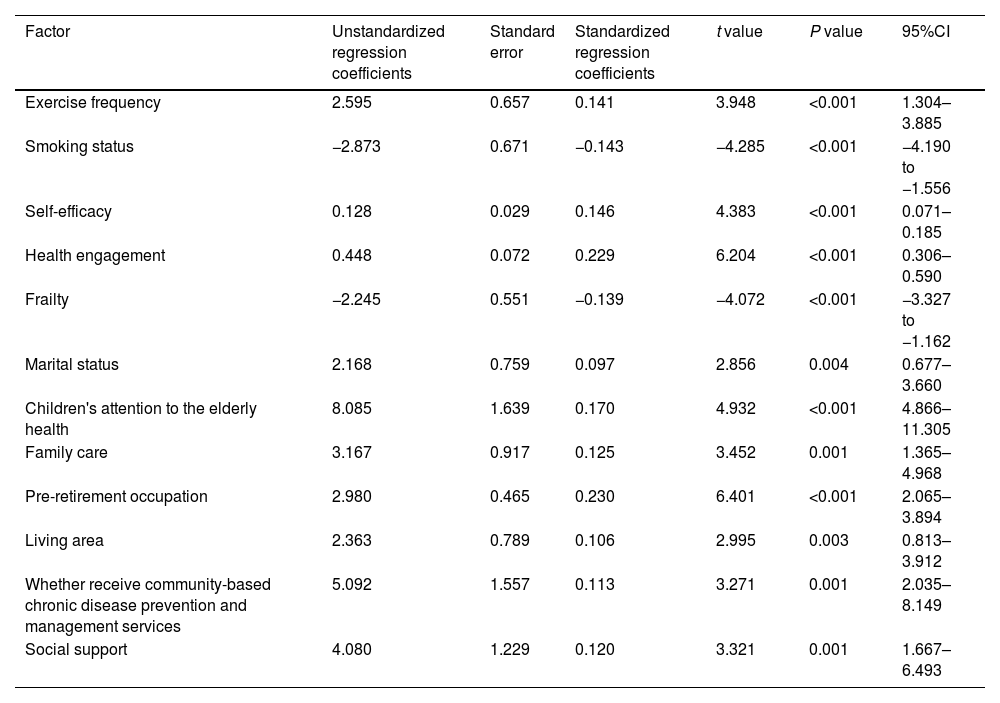
Using health promotion lifestyle as the dependent variable, variables that were statistically significant in the univariate analysis were used as independent variables, and stepwise regression was used for the analysis to gradually add each variable in the micro, meso, and macro systems to examine the effects of each factor on the health promotion lifestyle of the elderly while controlling for other variables. The results showed that exercise frequency, smoking status, self-efficacy, health engagement, and frailty at the micro level, marital status, children's attention to the elderly health, and family care at the meso level, and pre-retirement occupation, living area, whether receive community-based chronic disease prevention and management services, and social support at the macro level finally entered the model as associated factors of health-promoting lifestyles of the elderly (Table 4).
Stepwise multiple regression analysis of health promotion lifestyles of study participants (n=601).
| Factor | Unstandardized regression coefficients | Standard error | Standardized regression coefficients | t value | P value | 95%CI |
|---|---|---|---|---|---|---|
| Exercise frequency | 2.595 | 0.657 | 0.141 | 3.948 | <0.001 | 1.304–3.885 |
| Smoking status | −2.873 | 0.671 | −0.143 | −4.285 | <0.001 | −4.190 to −1.556 |
| Self-efficacy | 0.128 | 0.029 | 0.146 | 4.383 | <0.001 | 0.071–0.185 |
| Health engagement | 0.448 | 0.072 | 0.229 | 6.204 | <0.001 | 0.306–0.590 |
| Frailty | −2.245 | 0.551 | −0.139 | −4.072 | <0.001 | −3.327 to −1.162 |
| Marital status | 2.168 | 0.759 | 0.097 | 2.856 | 0.004 | 0.677–3.660 |
| Children's attention to the elderly health | 8.085 | 1.639 | 0.170 | 4.932 | <0.001 | 4.866–11.305 |
| Family care | 3.167 | 0.917 | 0.125 | 3.452 | 0.001 | 1.365–4.968 |
| Pre-retirement occupation | 2.980 | 0.465 | 0.230 | 6.401 | <0.001 | 2.065–3.894 |
| Living area | 2.363 | 0.789 | 0.106 | 2.995 | 0.003 | 0.813–3.912 |
| Whether receive community-based chronic disease prevention and management services | 5.092 | 1.557 | 0.113 | 3.271 | 0.001 | 2.035–8.149 |
| Social support | 4.080 | 1.229 | 0.120 | 3.321 | 0.001 | 1.667–6.493 |
Note: R2=0.357, adjusted R2=0.344, F-value=27.197, P<0.001.
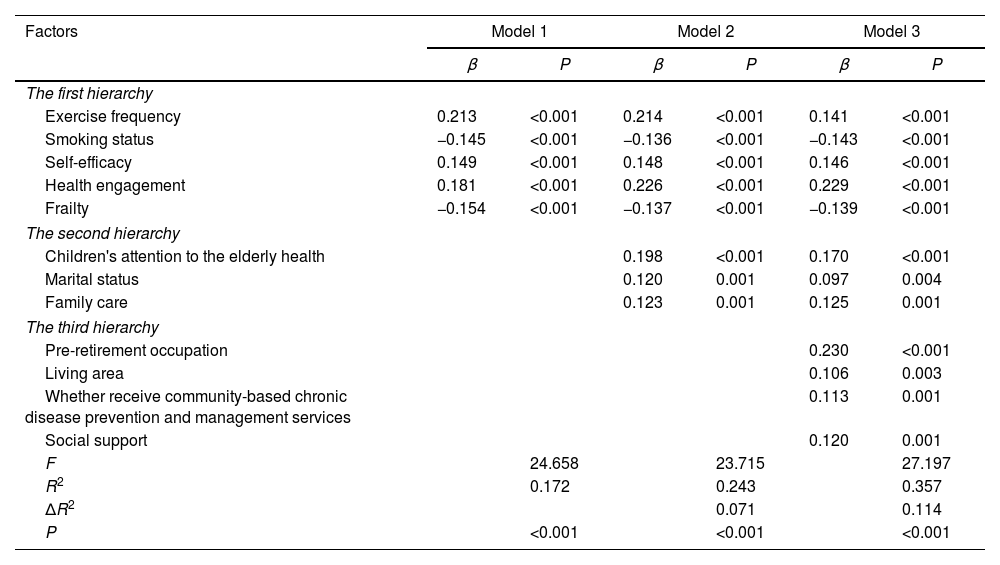
To complete the investigation on the influence of each system on health promotion lifestyles of the elderly, based on the social ecosystem theory, hierarchical regression analysis was conducted with the health promotion lifestyle of the elderly as the dependent variable and the factors with P<0.05 in the stepwise regression as the independent variables. The first hierarchy incorporated the microsystem associated factors, the second hierarchy incorporated the mesosystem associated factors, and the third hierarchy incorporated the macrosystem associated factors. The results presented that the R2 of microsystem was 0.172, with statistical significance (P<0.001), where exercise frequency played a major role in influencing the health promotion lifestyle of the elderly (β=0.213). The R2 rose to 0.243 after the incorporation of mesosystem in the second hierarchy, with statistical significance (P<0.001), where children's attention to the elderly health exerted a major relevant effect (β=0.198). An increase in R2 value to 0.357 was observed after the incorporation of macrosystem in the third hierarchy, with statistical significance (P<0.001), where pre-retirement occupation had a major relevant effect (β=0.230). See Table 5.
Hierarchical regression analysis of health promotion lifestyles of study participants.
| Factors | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| β | P | β | P | β | P | |
| The first hierarchy | ||||||
| Exercise frequency | 0.213 | <0.001 | 0.214 | <0.001 | 0.141 | <0.001 |
| Smoking status | −0.145 | <0.001 | −0.136 | <0.001 | −0.143 | <0.001 |
| Self-efficacy | 0.149 | <0.001 | 0.148 | <0.001 | 0.146 | <0.001 |
| Health engagement | 0.181 | <0.001 | 0.226 | <0.001 | 0.229 | <0.001 |
| Frailty | −0.154 | <0.001 | −0.137 | <0.001 | −0.139 | <0.001 |
| The second hierarchy | ||||||
| Children's attention to the elderly health | 0.198 | <0.001 | 0.170 | <0.001 | ||
| Marital status | 0.120 | 0.001 | 0.097 | 0.004 | ||
| Family care | 0.123 | 0.001 | 0.125 | 0.001 | ||
| The third hierarchy | ||||||
| Pre-retirement occupation | 0.230 | <0.001 | ||||
| Living area | 0.106 | 0.003 | ||||
| Whether receive community-based chronic disease prevention and management services | 0.113 | 0.001 | ||||
| Social support | 0.120 | 0.001 | ||||
| F | 24.658 | 23.715 | 27.197 | |||
| R2 | 0.172 | 0.243 | 0.357 | |||
| ΔR2 | 0.071 | 0.114 | ||||
| P | <0.001 | <0.001 | <0.001 | |||
A health-promoting lifestyle is a model for individuals to control, maintain and/or enhance their health.24 Currently, the age of “elderly” has not been clearly defined, and this study defines elderly as those aged≥60 years.25 This study demonstrated that the total score of health promotion lifestyle of the elderly in Hebei Province was 100.20±16.21, and the mean score of items was 2.50±0.40, which was in the lower limit of good level, slightly higher than the findings of Dong Yameng,26 but the excellent rate was only 3.66%, suggesting a large room to be improved in the healthy living level of the elderly in Hebei Province. In terms of dimensions, physical activity, as one of the elements of a healthy lifestyle, had the lowest standard score and excellent rate. Overall self-esteem, life functioning, social health, and cognitive functioning are significantly improved in the elderly with regular and moderate physical activity, and the effect of group exercise form is higher than that of individual exercise.27 Chinese Veteran's Sports Association has been established and government departments have consciously boosted the construction of grassroots sports facilities, but some issues still exist, such as single equipment and low utilization rate.28 This view was also evidenced in this study that 65.39% of the elderly exercised less than 2 times a week, which was lower than the standard of 3–5 times a week recommended by the General Administration of Sport of China.29 Additionally, the results of hierarchical regression analysis revealed that the physical frequency in the microsystem had the greatest impact on the health promotion lifestyle of the elderly (β=0.213). Thus, it is recommended that community managements popularize group exercise programs for the elderly at grassroots as appropriate, such as square dancing and walking, to increase the participation of the elderly in physical activities.
The microsystem accounted for 17.2%, and the results of stepwise multiple regression model showed that frailty, self-efficacy, and health engagement eventually entered the model. The elderly with serious frailty is less likely to adopt a healthy lifestyle, which is in line with Liu LK et al.30 Frailty, a distinctive personal characteristic of the elderly, becomes a risk factor for health-promoting lifestyle when it is severe and the body's ability to respond and reserve cognition declines.31 Self-efficacy, which refers to the ability to confidently adopt adaptive behaviors confronting challenges, is considered by efficacy theory to have irreplaceable value in controlling and regulating individual behavior.32 It was theorized to be an important protective factor for health-promoting lifestyle in this study, congruous with existing views.33 The results illustrated that health engagement is also an important positive factor in health promotion among the elderly. In view of this, we proposed the hypothesis that higher self-efficacy of the elderly was more possible to drive more health engagement and ultimately make this population live higher levels of healthy lifestyle. The validation of this hypothesis is ongoing.
The mesosystem accounted for 7.1%, children's attention to the elderly health, marital status, and family care eventually entered the regression model. Influenced by the traditional Chinese concept, home care is still the main form of living out life in retirement in China.34 The family system has become an important source of life care, emotional comfort, and financial support for the elderly, among which the spouse is the closest and most trusted person, and the health-promoting lifestyle of the elderly with a spouse is much higher than that of others.35 In this work, the health-promoting lifestyle of married elderly was found at a good level, much higher than that of the elderly in other types of marital status, which coincides with the above view. Children's attention to the health of the elderly is the most influential protective factor in the mesosystem, and children supervising the health of the elderly is also a process of positive interaction with the elderly, which, in addition to maintaining nutrition and supervising exercise, can generate a sense of well-being and spirituality, in agreement with the theme of healthy aging.36 As suggested by scholars, a shared living pattern with a spouse is most beneficial for improving the poor lifestyle of the elderly, while maintaining a “separate but not apart” living pattern with children, where the married children live near the elderly, profits most for promoting their health.37 Nevertheless, with the miniaturization of family structure, the proportion of empty nest elderly in China is as high as 49.3%, and the family function is seriously weakened.38 This situation prompted us to think deeply about how to establish a mechanism for interaction between children and the elderly in the multiple contexts of aging, empty nest, and developed Internet, so as to bring into play the family function and ensure that the elderly achieve a healthy lifestyle.
The macrosystem accounted for 11.4%. Pre-retirement occupation, living area, whether receive community-based chronic disease prevention and management services, and social support entered the stepwise regression model. In China, retirement ages differ for employees of different sexes. According to the relevant documents issued in 1978, the retirement age for men and women is 60 and 50 years old, respectively.39 As the relational networks of the elderly shrink with age, their community becomes a macrosystem for them to obtain health information, and pre-retirement occupation tends to determine the social resources available in that system, such as neighborhoods, friend support, and health services. Pre-retirement occupation became the most associated variables in Model 3 in this study (β=0.230). The social support for the elderly was proportional to levels of health-promoting lifestyles, the same as the results of Yang Xiaojiao et al.,40 where cordial neighborhood relationships and extensive friend support substantially decreased discrepancy in health lifestyles among the elderly with different characteristics. Due to the unbalanced development, older people living in urban areas, objectively, have an advantage in sharing health service resources and accessing the social security system over those in urban-rural fringe areas and rural areas. Univariate analysis revealed that the elderly living in urban areas has a higher level of health promotion lifestyle, in line with the results of Yanxia Hu et al.41 Community-based chronic disease prevention and management services are a critical health resource available to the elderly and play a pivotal role in the tertiary prevention of chronic diseases. The accessibility of community health services has a fundamental protective effect on the health promotion of the elderly.42 In this study, the accessibility of community health services was an important factor influencing the health promotion of the elderly, however, the proportion of the elderly who had received community-based chronic disease prevention and management services in this study was only 16.5%. This data laterally reflects the low coverage and lack of implementation of grassroots community health services in our province, which needs to be paid attention to. Accordingly, it is suggested that health promotion for the elderly should be realized in terms of improving publicity methods, medical equipment, and medical experience.
There are some limitations. Firstly, because this study was a cross-sectional study, it was impossible to infer the causal relationship between healthy aging and the variables. More longitudinal studies are needed to develop interventions more accurately. Secondly, this study excluded participants with cognitive decline, dementia, heart failure, and respiratory failure, and the selection of participants may cause bias in the results, thus affecting the representativeness of the results. Finally, because we selected only one city in China for the survey, the study population was not representative of the general elderly population in China, and also the social environment in China cannot be equated with other countries, so the results may not be generalized for generalization throughout China and the world. Therefore, we consider conducting a multicenter study with a large sample size in China. Additionally, it is difficult to investigate the elderly in other countries and may require their assistance to do so.
ConclusionHealth promotion lifestyles of the elderly in Hebei Province were at the lower limit of good levels. This study confirmed the important role of individual characteristics of the elderly and their surrounding environment in health promotion lifestyle based on the social ecosystem theory, in which the roles of microsystem and macrosystem were slightly bigger than that of mesosystem. In addition, exercise frequency, the children's attention to the elderly health, and pre-retirement occupation were key factors related to the health promotion lifestyle of the elderly. This study conducted an important exploration of health promotion lifestyles of the elderly and provided some theoretical basis for corresponding policy formulation. Our ongoing object is to investigate the influence of self-efficacy-related factors on the acquisition of healthy lifestyles by the elderly in the face of health challenges.
Authors’ contributionsYing Han participated in the design and drafted the manuscript, Fengmei Xing and Jiali Huang conducted the experiments and revised it, Mengyi Wang collected and assembled the data. All authors read the article and approved submitted version.
Contributions- 1.
The aging situation in China is severe and may cause a huge economic burden in the coming decades. This study investigated the associated factors of health promotion lifestyles of the elderly based on the social ecosystem theory, with the aim of providing realistic and guiding implications for the health management and promotion of the elderly in Hebei Province.
- 2.
This study confirmed the important role of individual characteristics of the elderly and their surrounding environment in the health promotion lifestyle based on the social ecosystem theory.
- 3.
Exercise frequency, children's attention to the elderly health, and pre-retirement occupation were the key factors related to the health promotion lifestyle of the elderly.
This study was approved by the Ethics Committee of North China University of Science and Technology (2021163).
Availability of data and materialsThe data and materials in the current study are available from the corresponding author on reasonable request.
FundingThis study was supported by an empirical study on the health promoting lifestyle of the elderly based on social ecosystem (20210301129).
Conflict of interestThe author reports no conflicts of interest in this work.
