






Introduction
Alcohol is currently estimated to be responsible for a large number of potential years of life lost.1 However, defining the limit of excessive alcohol consumption is complex, as the amount differs for each person. There is no «magic number» for the limit of alcohol that is hazardous.2 The figures used now are variable but do not differ much in general terms. In our study we used the criteria of the Spanish Society of Family and Community Medicine (SSFCM, semFYC in Spanish) to diagnose risk drinking, because these criteria have been clearly defined.3 Many studies have shown that drinking decreases after information and educational interventions are used:4-8 when people known the limit for risk drinking, they drink less. As a measure aimed at primary prevention, health authorities should insist that information be made publicly available about hazardous levels of alcohol consumption. If heavy drinkers continue to consume large amounts of alcohol even when they know their intake is hazardous, brief interventions should emphasize other elements such as motivation, awareness and education as measures of secondary prevention.
This raises the following question: Do people know how much alcohol can be hazardous to their health? Some studies have investigated drinking habits in populations of primary care users, and we have found studies from English-speaking countries that looked into the general public's perception of risk levels related with drinking.9 However, we have found no studies that analyzed, in persons who use primary care services in our setting, their knowledge of the amounts of alcohol that can damage health and the negative effects of excess drinking.
The aims of the present study were therefore:
1. To evaluate our patients' knowledge of established limits for excess drinking and the health problems this can lead to.
2. To determine whether knowledge of the effects of drinking was related with drinking habits as entered in the patient's medical record at the health center.
Material and methods
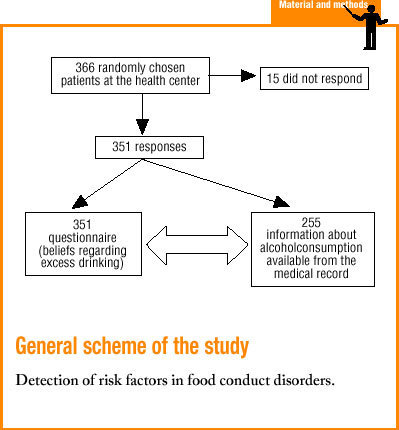
The study population consisted of all adults who were seen at any of the 12 family medicine practices at the Chantrea Health Center in the city of Pamplona, Northern Spain. This center serves 18 700 inhabitants older than 14 years, and the predominant socioeconomic level in the area is medium to low. This was a descriptive, cross-sectional study based on data obtained with a self-administered questionnaire (Annex 1) completed by a random sample of the patients who came to the health center during the fourth trimester of 2000. Additional data for alcohol consumption were obtained from the participants' medical records. To ensure representativeness of the sample, we randomly selected 11 days during the trimester to recruit participants. This method has been shown in earlier studies to be suitable for random sampling of primary care patients.10
Sample size was calculated with the formula
n=k(p)(1-p)/e2
where k=l.96; p=0.5, and e=0.05. The minimum sample was set at 366 persons, or 33 persons on each designated day. During 6 days participants were drawn from users in the waiting rooms for different practices (2 practices per day chosen randomly each day), and during 5 days participants were drawn from the waiting room for patients assigned to any of the 12 practices but who had come to the center without an appointment for that day. Two members of the research team distributed questionnaires and pens to patients in the waiting room, answered questions, and collected the completed questionnaires. Although no personal information was collected, patients were asked what time their appointment was scheduled so that they could be identified from the list of that day's patients and their medical record could be consulted to obtain information on their drinking habits.
A pilot study was carried out to identify possible problems with the questionnaire and participants' reactions. After the pilot study the item that inquired about health problems excess drinking can cause, initially designed as an open question, was redrafted in the form of a closed question with 16 specific problems: those mentioned most often in the pilot study and a few additional problems not related with drinking, but that were added as a check for the correct completion of the instrument. (Some participants marked all 16 choices on this item.)
To ensure internal consistency we included two items that referred to liver diseases caused by excess drinking, in the item about specific problems caused by excess drinking and in the final item. When we analyzed the concordance between answers, these two items yielded a kappa index of 0.98.
The following variables were analyzed: age in years; sex (male or female); 16 specific health problems, some related with excess drinking, others not (Annex 1); the number of alcoholic drinks per day and per week that the participant considered the limit above which further drinking was hazardous to health; and drinking habit as noted in the clinical record (only for patients whose consumption was clearly recorded as a given amount of a specific alcoholic beverage, or grams of alcohol per day, even when the information was not recent).
Although participants were asked about their employment status and whether they customarily drove a motor vehicle, and although the frequency of drinking was obtained from the medical record, these variables were not taken into account as the preliminary analysis showed that they were strongly influenced by age and sex. To compare the limit of risk identified by each person with the recommended standard limits, we used the SSFCM recommendations:3 280 g/week in men and 168 g/week in nonpregnant women, or the daily equivalents (4 units/day for men, 2.4 units/day for women). To keep the questionnaire as simple as possible, we did not include an item on the complementary criterion «drinking 50 g in 24 h at least once per month.» To convert the amounts of alcoholic beverages into grams of alcohol we used the following equivalents: 1 standard drink unit (SU)=two 100-mL glasses of beer=one 100-mL glass of wine=1/2 glass of distilled spirits, mixed drinks or whisky (25 mL). A standard unit was considered 10 g de alcohol, the value that was easiest to convert accurately for alcoholic drinks consumed in our setting.11,12
All data were entered in a database built with Access. Statistical analyses were done with the Epi-Info and Epitable programs. Analysis of variance (ANOVA) and Student's t test were used for comparisons of mean values, and the chi-squared test was used to compare qualitative variables.
Results
Fifteen persons did not complete the questionnaire for various reasons: lack of time, incapacitating acute illness or lack of interest in the study. Of the 351 persons who responded, we were able to locate the health center's clinical records for 318. No medical record could be found for 2 patients, and 31 others were not assigned to our center (and therefore their medical records were presumably held elsewhere). Clear information about drinking habits was available in 255 of the 318 records. In 21 records the information was unclear, and no information on drinking habits was entered in 42 records. Of the medical records that contained imprecise or no information about drinking habits (63 in all), 68% were for persons aged 15 to 34 years. Of the 351 persons who completed the questionnaire, 39.9% were men and 60.1% were women. Mean age was 49.8 years (SD 18.4 years), and did not differ significantly between men and women.
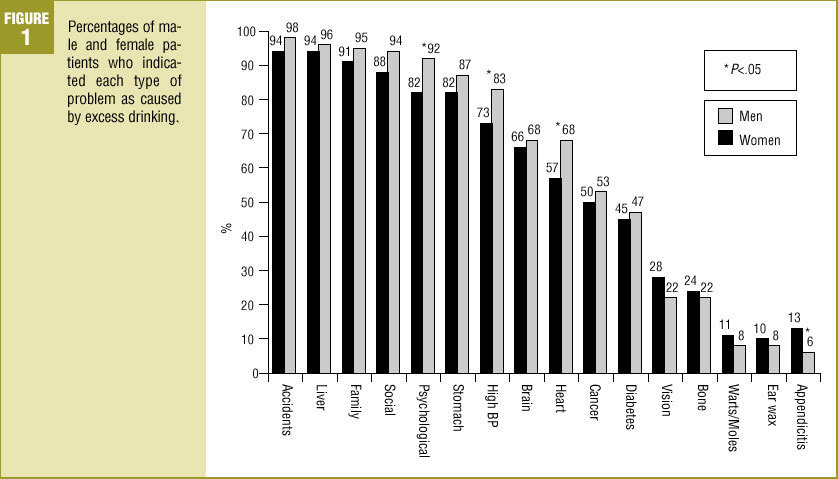
Knowledge of problems caused by excess drinking Figure 1 shows the proportion of responses for each type of disease on the item «Please make a cross in the box next to each type of problem you believe excess drinking can cause.» Almost all participants (98%) identified at least one problem as clearly related with excess drinking. However, 32% of the participants also marked specific problems known not to be related with drinking. This group did not differ from the rest of the sample with regard to sex or alcohol consumption, but their mean age was significantly higher (60.6; SD, 16.1 years, vs 44.7, SD, 17.2 years; P<.001).
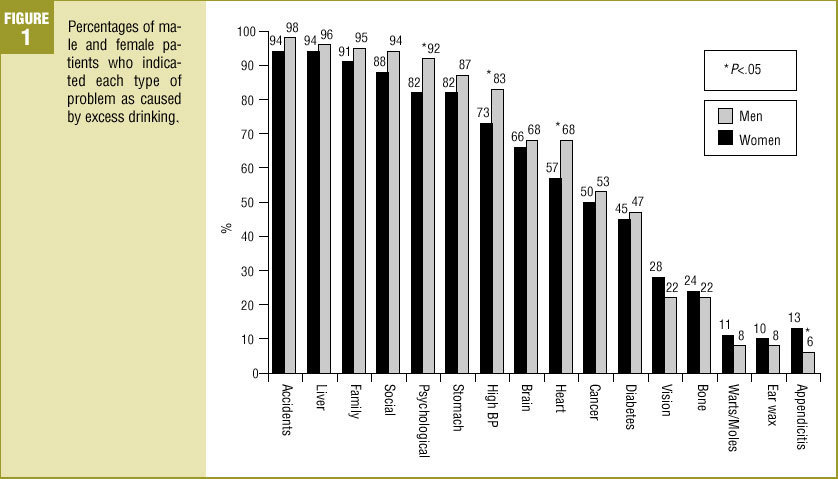
FIGURE 1. Percentages of male and female patients who indicated each type of problem as caused by excess drinking.
Opinion on the limits of alcohol consumption that are hazardous to health (LAHH)
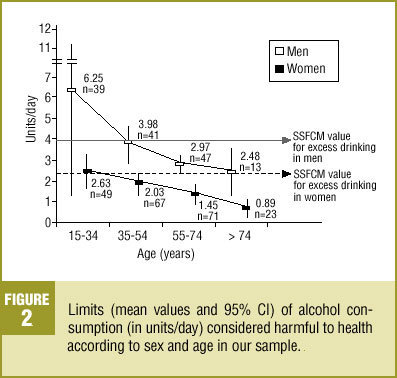
Figure 2 illustrates the results for men and women in different age groups.
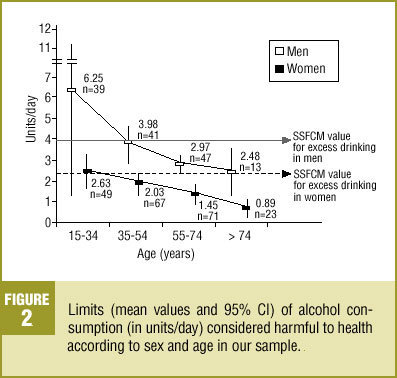
FIGURE 2. Limits (mean values and 95% CI) of alcohol consumption (in units/day) considered harmful to health according to sex and age in our sample.
Concordance for the limit of hazardous drinking between daily and weekly amounts
To check whether participants' knowledge of the daily limit of drinking that is hazardous to health matched their knowledge of the weekly limit, we analyzed the concordance between the two values by calculating the kappa index. The resulting value was 0.69. We considered two groups for daily and weekly alcohol consumption: persons who indicated a LAHH equal to or below the value recommended by the SSFCM, and persons who indicated a LAHH higher than the SSFCM value. The values given for weekly consumption were found to be consistent with the limits for daily consumption.
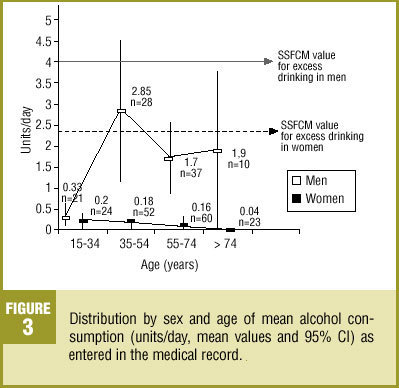
Description of alcohol consumption in our sample (Figure 3)
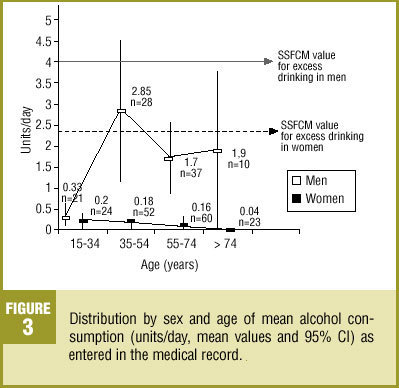
FIGURE 3. Distribution by sex and age of mean alcohol consumption (units/day, mean values and 95% CI) as entered in the medical record.
Mean alcohol consumption for the 255 participants who completed the questionnaire and whose medical record provided precise information on drinking habits was 0.76 units/day (SD, 2.01 units/day).
Profile of excess or risk drinkers
We found 14 persons (14/255=5.4%) who apparently drank in excess. The 13 men represented 14% of all men in the sample, and the 1 women in this group represented 1% of all women in the sample. Mean age was 55 years (95% CI, 29-81 years). These 14 participants did not differ from the rest of the sample in mean age or in LAHH (mean LAHH in the group of 13 men was 3.73 units/day; SD, 2.24 units/day). Regarding problems related with excess drinking, risk drinkers' responses were similar to those of the rest of the sample, except for the significantly lower percentages of the former who indicated a connection between drinking and accidents (85%), liver disease (78%), family problems (71%) and heart disease (35%).
Comparison of alcohol consumption according to degree of awareness
We compared 2 groups defined by the difference between the LAHH and the standard limits:
LAHH lower than or equal to the SSFCM value (aware): 269/351 (76%).
LAHH greater than the SSFCM value (unaware): 82/351 (24%).
The drinking patterns for these two groups are contrasted in Table 1.
Personal congruence
We compared individuals' actual alcohol consumption (according to information from the medical record) with individual LAHH as indicated on the questionnaire. Ten percent of the participants (26/255) drank more than what they considered their LAHH; the drinking pattern in these individuals was considered incongruent in the present study. Most individuals (229/255, 90%) drank the same amount or less than their LAHH; these persons were considered congruent. The characteristics and alcohol consumption in each group are shown in table 2. In the group of incongruent drinkers, men were clearly in the majority. These individuals drank more than members of the congruent group regardless of sex, and most excess drinkers were members of the incongruent group. The responses provided by these participants to the item regarding specific problems caused by excess drinking were similar to those given by participants in the congruent group.
Discussion
This study was based on results obtained with a self-administered questionnaire. The results may have been biased by misunderstanding some of the items; possible bias was reduced by having the researchers present to answer participants' questions. This measure favored correct completion of the instrument and led to a high response rate (96%). To check the reliability of the instrument we included two versions of the same question, and found concordance between the responses to be high (kappa=0.98). Also of note was the high proportion of medical records that correctly noted the patient's alcohol consumption (80%), although we caution that we considered this information as it appeared without taking into account whether it was up to date. This is a potential limitation to the validity of our conclusions.
Awareness of problems that alcohol can cause
Practically all participants (98%) believed that excess drinking could cause at least one of the problems listed in the questionnaire. Women in general were more aware of the effects of excess drinking. Certain health problems were noted to be related with excess drinking by more than 70% of the participants, whereas other problems such as cerebral and heart disease and cancer were related with drinking by only slightly more than half of them. We also found that 32% of the participants indicated a relationship between excess drinking and diseases that in fact are unrelated to alcohol intake. Mean age in this group was higher than in the rest of the sample, which may indicate that older persons tend to attribute more problems to excess drinking than are actually the case.
In general, awareness of the limits of alcohol consumption that could be hazardous to health was good: 76% of the participants placed their personal LAHH at or below the SSFCM value. However, men below the age of 35 years were found to be less aware of the limits of hazardous drinking than the rest of the sample. Table 2 shows that younger persons who drank more (mean 1.28 units/day) were less well informed than participants who drank less (mean 0.63 units/day). These findings should serve as a stimulus for preventive efforts based on health education, with emphasis on information about harmful limits and recommendations to drink less. These efforts should be aimed at all users of the health center, but especially at younger men. The questionnaire did not inquire about heavier drinking on certain days, such as on weekends. This information might have been useful to analyze younger persons' beliefs regarding alcohol use.
Although the aim of this study was not to analyze drinking behavior, we note that alcohol consumption was significantly lower in persons aged 15 to 34 years than in the rest of the sample. In school-aged persons, most drinking is known to take place on specific days of the week. These persons are also known to be largely unaware of the effects of alcohol.13 A study in Navarra found that approximately 30% of all young persons drank very little, and that 60% drank only on weekends.14 Although mean daily consumption in young people is lower than at other ages, this drinking pattern is associated with a high level of risk, especially of being involved in traffic accidents. In this connection it is important to recall that drinking habits were infrequently noted in the medical records of younger persons who participated in our study (68% of the 63 records that contained imprecise or no information on drinking habits were for persons between 15 and 35 years of age). Health centers should be encouraged to record drinking patterns and note the actual amounts of alcohol consumed, especially for young persons, and to update this information every 2 years in accordance with the recommendations of the PAPPS (Preventive and Health Promotion Activities Program)15 in quantitative terms. Drinking 50 g or more of alcohol in 24 h at least once a month is also considered a type of risk drinking.
We identified 5.4% of the participants in our sample as excess drinkers: 14% of the men and 1% of the women. This figure was slightly lower than expected,11,15 as earlier studies reported excess drinking in 15%-20% of the men and 2%-5% of the women. The profile of excess drinkers was that of a man older than 30 years who was aware of the problems caused by excess drinking, but who underestimated the effects of alcohol on certain health problems.
Regarding the congruence between beliefs and actual drinking, participants in our study generally drank in accordance with their self-reported LAHH. However, 10% of these individuals drank more than what they themselves considered to be an excessive amount of alcohol. Most of these participants were men, and most of the problem drinkers (80%) formed part of this group. The mean LAHH stated by problem drinkers was lower than the SSFCM figure. Due regard must be given to the limitations imposed by the fact that the information about drinking recorded in the medical record may not have been up to date. However, our findings indicate that excess drinkers are aware of the limit beyond which drinking can be hazardous to their health. In addition, these participants seemed to underestimate the effects of excess drinking on certain diseases. The usefulness, for this group, of additional information on the limits of drinking that can be hazardous to health seems debatable, as these persons drink more than the amounts they themselves consider harmful, although they are unaware of this. It is important to make excess drinkers aware of this incongruence, although blame-laying should be avoided.
In addition, providing information about the consequences of excess drinking would seem useful, particularly with regard to the risk of accidents, family problems, heart disease and liver disease. When necessary, messages about the effects of drinking on the latter can be reinforced with the results of laboratory tests.
Because most excess drinkers in the present study were members of the group of incongruent drinkers, future studies should investigate whether persons with incongruent drinking behavior but who are not excess drinkers are at greater risk than congruent drinkers for becoming problem drinkers. If incongruent drinking is a marker of risk or constitutes a stage that precedes excess drinking, measures could be designed to prevent the progression to risk drinking--an important primary care intervention. Additional studies will be needed to shed light on this issue.
Conclusions
1. There is good general awareness, especially among women, of the limits of alcohol that can be hazardous to health, and of the consequences of excess drinking. However, gaps in the participants' knowledge were found regarding the associations between excess drinking and cerebral and heart disease and cancer.
2. Younger men tended to state a LAHH higher than the recommended limit. Because the low level of consumption in this group may be the result of underrecording of drinking habits in younger persons, we emphasize the need to question them about both their usual drinking patterns and their sporadic drinking episodes, and to inform them of the limits and consequences of excess drinking.
3. Excess drinkers in our sample stated a daily LAHH that was lower than the value set by the SSFCM. Hence excess drinking does not appear to be related with lack of information about amounts of alcohol that can be hazardous to health. Other educational measures such as awareness-raising are therefore necessary.
