



GeneXpert is one of the recent technological instruments used to diagnose tuberculosis in a short span of time. In this study, the performance of GeneXpert MTB/RIF assay for the diagnosis of extrapulmonary tuberculosis (EPTB) was compared with light-emitting diode Fluorescent Microscopy (LED-FM) in Khyber Pakhtunkhwa, Pakistan. A total of 737 EPTB samples were collected from tuberculosis (TB) suspected patients. Out of these samples, male to female ratio was 53% (n=390) to 47% (n=347) respectively. The sensitivity and specificity was 73% and 100% for GeneXpert, while 40% and 100% for LED-FM microscopy. This shows that the sensitivity of GeneXpert is 40–50%, higher than LED-FM microscopy. GeneXpert also detected low number of bacilli as compared to LED-FM microscopy.
Mycobacterium tuberculosis complex (MTBC) is the causative agent of tuberculosis (TB). TB is the second leading cause of death after HIV worldwide. It is estimated that 9 million people develop TB and among them 1.5 million die each year out of which 360,000 people are HIV positive.1 In Pakistan 350 cases of TB per 100,000 population are reported. Pakistan is ranked 5th among 22 high burden TB countries.2 MTBC mainly infect lungs (pulmonary) and seldomly affects other parts of the body known as extra pulmonary tuberculosis (EPTB).3,4 Worldwide, 10% of extrapulmonary cases are reported every year.5 More than 50% of TB cases are reported with HIV co-infection.6 The reason for increased EPTB incidences in Pakistan is still vague due to lack of proper diagnosis. Microscopic observation of M. tuberculosis in sputum smears still remains the pillar of tuberculosis (TB) diagnosis in developing countries, despite its poor sensitivity.7 Fluorescence microscopy (FM) of smears have been studied as an alternative to conventional light microscopy with Ziehl Neelsen staining (ZN).8 On the basis of these findings, World Health Organization in 2011 replaced conventional FM by LED-FM and phase in LED-FM as an alternative to ZN microscopy.9
There are a number of tests available for the diagnosis of tuberculosis each having their own limitations. Conventional microscopy has low sensitivity and culture requires longer time for positivity. The commercially available automated, liquid MGIT (Mycobacterium Growth Indicator tube) culture system is time-consuming and requires specialized laboratories. On the other side, nucleic acid amplification techniques not only provide the advantage of rapidity of diagnosis but also detect even low genomic copies in various specimens and curtail the transmission of the disease.10
The World Health Organization (WHO) has endorsed the implementation of GeneXpert MTB/RIF assay for national tuberculosis programs in developing countries.11 The Xpert MTB/RIF (Cepheid Inc.) is an automated, user friendly and rapid test based on nested real-time PCR assay and molecular beacon technology for MTB detection and RIF resistance.12 The results are obtained within a short period of time (2h). Moreover this technique is not prone to cross-contamination, requires minimal Biosafety facilities and has a high sensitivity in smear-negative pulmonary TB.13 The diagnosis of EPTB is often difficult to establish, considering that number of bacteria in specimens is often very low, a collection often requires invasive procedures, and it is not easy to obtain multiple samples. In this scenario GeneXpert is a potentially useful tool for extrapulmonary specimens.14
The current study aims to investigate the diagnostic accuracy of GeneXpert for EPTB specimens and compared with LED-FM microscopy. The percentage of enhanced case detection rate in EPTB samples was also studied.
Materials and methodsThis study was conducted in Provincial TB Reference Laboratory Peshawar Khyber Pakhtunkhwa, from January 2013 to January 2015 in which two different techniques that is GeneXpert MTB/RIF assay and LED-FM microscopy were compared. The result of both tests was evaluated against reference standard culture method.
Area/patients selectionA total of 737 samples of EPTB on the basis of clinical presentation, radiological finding and histopathological evidence were collected from TB suspects from three tertiary care hospital, 332 samples from Lady Reading Hospital (LRH), 149 and 256 samples from Khyber Teaching Hospital (KTH) and Hayatabad Medical Complex (HMC) respectively. Samples were aspirated from different body parts i.e., n=259 Pleural fluids, n=25 biological alveolar lavage (BAL), n=59 cerebrospinal fluid (CSF), n=82 pus, n=125 ascetic fluid, n=13 synovial fluid, n=47 urine, n=56 pericardial fluids, n=36 bone marrow, n=35 soft tissues.
Sample processingCulture processing procedureAll samples were subjected to decontamination process according to standard protocol except bone marrow and CSF.15,16 Some specimens should not be decontaminated, because either they are sterile source i.e. CSF or decontamination process is a rough method and there is a risk of killing TB bacilli.17 After digestion and decontamination, samples were diluted with 50mL sterile phosphate buffer, pH 6.8, to minimize the continuing action of NaOH and to lower the pH and specific gravity of the specimen before centrifugation. Following refrigerated centrifugation, the falcon tubes were kept for 5min to allow aerosols settle down. Once the supernatant was decanted, 1mL of buffer was added and vortexed to homogenized the pallets. 200ul of the sample was added to 7mL MGIT tube supplemented already with PANTA. All the tubes were incubated in MGIT (Bactec 960, BD, USA) semi-automated liquid culture system machine for 42 days at 35–38°C.
Post MGIT identificationThe identification of MTBC was done by two different methods, including Ziehl Nelson staining (ZN) Microscopy and TBC (Becton, Dickinson and Company) device method. Staining using ZN was carried out according to standard published procedure, and slides were examined with bright-field microscopy (Olympus CX21) at 1000× magnification. TBc is a rapid immuno-chromatographic device which was used to determine clinical isolates to the species level.
GeneXpert MTB/RIF assay and LED-FM microscopySmear for LED fluorescent microscopy were prepared according to standard procedures.11 Smears for FM were stained using auramin O. Briefly, smears were flooded with Auramin O for 10min, destained with acid alcohol for 2min, and then counterstained with methylene blue for one minute. With auramine O staining, Mycobacteria appear as bright yellow fluorescent rods on a dark background. The slides were examined with ZEISS EXTARO 300 at 20× magnification. The presence or absence of AFB was reported using WHO/IUATLD guideline.18
The sediment samples by cytocentrifugation were processed for Xpert MTB/RIF assay. Using a fresh transfer pipette, 2mL of the processed sample was transferred to the Xpert MTB/RIF cartridge 10. Load the cartridge into the GeneXpert instrument as per manufacturer's instructions according to standard protocol.14,19 The MTB/RIF assay interpretation is software based and not user dependent.20 The sensitivity and specificity of each sample were calculated according to the following formula
Sensitivity:

Specificity:
Results
Our study was the first to show the successful implementation of LED-FM staining and Xpert MTB/RIF services in routine programmatic conditions in Khyber Pakhtunkhwa, Pakistan. A total of 737 samples were processed, 53% (n=390) were male and 47% (n=347) were female.
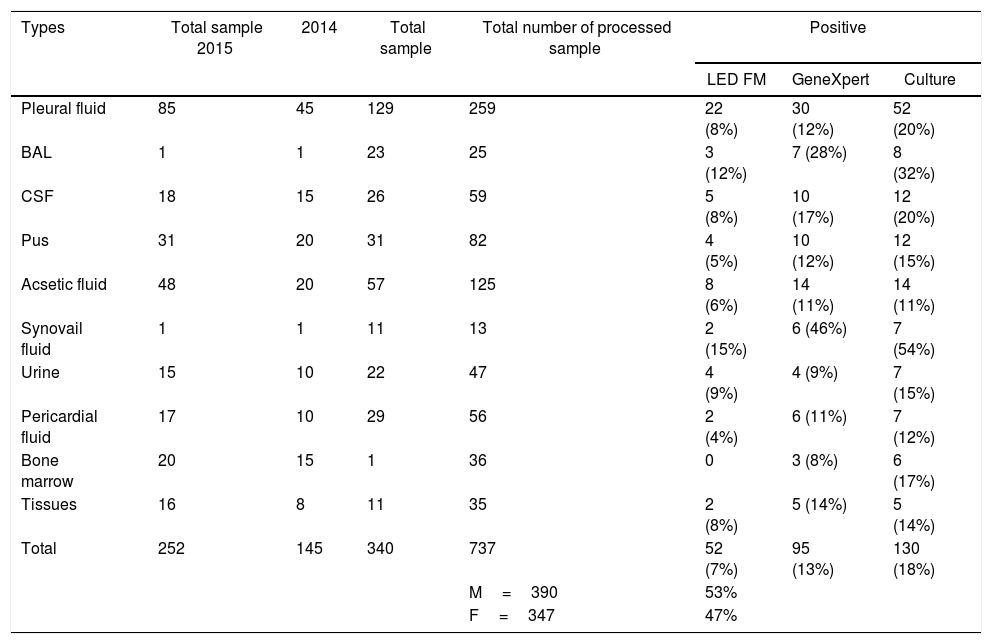
Detection of M. tuberculosis by Xpert MTB/RIF assayTotal positive on Xpert MTB/RIF assay declared 13% (n=95). Table 1 shows results of EPTB for GeneXpert technique. The sensitivity values obtained through GeneXpert ranges from 50 to 100% while Specificity remains high (100%) as shown in Table 2.
Sample wise comparison of LED-FM, GeneXpert and culture.
| Types | Total sample 2015 | 2014 | Total sample | Total number of processed sample | Positive | ||
|---|---|---|---|---|---|---|---|
| LED FM | GeneXpert | Culture | |||||
| Pleural fluid | 85 | 45 | 129 | 259 | 22 (8%) | 30 (12%) | 52 (20%) |
| BAL | 1 | 1 | 23 | 25 | 3 (12%) | 7 (28%) | 8 (32%) |
| CSF | 18 | 15 | 26 | 59 | 5 (8%) | 10 (17%) | 12 (20%) |
| Pus | 31 | 20 | 31 | 82 | 4 (5%) | 10 (12%) | 12 (15%) |
| Acsetic fluid | 48 | 20 | 57 | 125 | 8 (6%) | 14 (11%) | 14 (11%) |
| Synovail fluid | 1 | 1 | 11 | 13 | 2 (15%) | 6 (46%) | 7 (54%) |
| Urine | 15 | 10 | 22 | 47 | 4 (9%) | 4 (9%) | 7 (15%) |
| Pericardial fluid | 17 | 10 | 29 | 56 | 2 (4%) | 6 (11%) | 7 (12%) |
| Bone marrow | 20 | 15 | 1 | 36 | 0 | 3 (8%) | 6 (17%) |
| Tissues | 16 | 8 | 11 | 35 | 2 (8%) | 5 (14%) | 5 (14%) |
| Total | 252 | 145 | 340 | 737 | 52 (7%) | 95 (13%) | 130 (18%) |
| M=390 | 53% | ||||||
| F=347 | 47% | ||||||
Comparison between LED-FM, GeneXpert sensitivity and specificity.
| Total | Pleural fluid | BAL | CSF | Pus | Ascetic fluid | Synovail fluid | Urine | Pericardial Fluid | Bone Marrow | Tissues. | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GX | LED-FM | GX | LED-FM | GX | LED-FM | GX | LED-FM | GX | LED-FM | GX | LED-FM | GX | LED-FM | GX | LED-FM | GX | LED-FM | GX | LED-FM | GX | LED-FM | |
| Sensitivity % | 73 | 40 | 58 | 42 | 88 | 38 | 83 | 42 | 83 | 33 | 100 | 57 | 86 | 29 | 57 | 57 | 86 | 29 | 50 | 0 | 100 | 40 |
| Specificity % | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| PPV | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| NPV | 95 | 89 | 90 | 87 | 94 | 77 | 96 | 87 | 98 | 90 | 100 | 95 | 86 | 55 | 93 | 93 | 98 | 91 | 91 | 83 | 100 | 91 |
PPV, positive predictive value; NPV, negative predictive value; GX, GeneXpert; CSF, cerebrospinal fluid; LED-FM, light emitting diode fluorescent microscopy.
Total positive on culture was 18% (n=130) (Table 1). Further, there were no samples found that have culture positive results and GeneXpert and LED-FM negative.
Detection of M. tuberculosis by LED fluorescence microscopyTotal positive on LED-FM microscopic technique declared 7% (n=52) (Table 1). The lowest sensitivity recorded by LED-FM is 0 for bone marrow while the highest is 57% for ascetic fluid and urine samples. Specificity for LED fluorescence microscopy remains high (100%) as shown in Table 2.
DiscussionIn the current investigation, the diagnostic performance for EPTB cases of two different techniques were evaluated. The results were compared with reference standard culture technique. A total of 737 EPTB samples were analyzed with the detection rate of LED-FM, 7% (n=52), GeneXpert MTB/RIF assay 13% (n=95), while for reference standard culture technique 18% (n=130). The sensitivity and specificity for GeneXpert MTB/RIF assay was 73% and 100%, while that of LED-FM microscopy was 40% and 100% respectively. A better detection rate of GeneXpert was reported in a study when compared to smear microscopy and culture.21
The results revealed that the detection rate (specificity and sensitivity) of the tested samples for GeneXpert MTB/RIF assay was almost twofold to that of LED-FM microscopy (Table 2). Previous investigations showed that the specificity and sensitivity of GeneXpert MTB/RIF was 79.0% and 97.3% respectively.22 Some other studies showed specificity and sensitivity of 95% and 100% respectively in 340 positive samples.23 This higher ratio in term of sensitivity in comparison to our results may be due to sample size.
The current conventional techniques, i.e. LED-FM and culture system not only requires the Biosafety Level III (BSLIII) and trained personnel but also take several weeks to yield results. The GeneXpert MTB/RIF is a proven technology in TB diagnosis. The GeneXpert MTB/RIF assay is independent of the user's skills and routine staff with minimal training can use the test. The efficacy of GeneXpert MTB/RIF was proved to be much higher than conventional LED-FM and comparable to that of culture. We observed a sensitivity of 73% and specificity of 100%, which was comparatively higher than the sensitivity observed in a study which consisted 52% of EPTB samples.24 In another published work carried out in EPTB cases, Tortoli et al., 2012.22 reported 86.9% sensitivity and 99.7% specificity by GeneXpert, slightly higher than our results.
The sensitivity of GeneXpert was 40–50% higher than the LED-FM technique while in a previous study carried by,25 the sensitivity of GeneXpert MTB/RIF assay was 45% higher than microscopy technique. If we compare our study with previous study it depicts same results regarding sensitivity and specificity (Table 2). Armand et al., reported the same results for both the techniques regarding specificity.26 The positivity of EPTB increased from LED-FM to GeneXpert followed by culture gold standard. We found that the implementation of GeneXpert services in TB Diagnostic centers enhance the yield of EPTB patients. It has a shorter turnaround time and simultaneously detects refamicin (RIF) resistance in less than 3h. GeneXpert is preferred over the conventional techniques because of its high specificity, sensitivity and with minimal technical expertise required. Although, conventional laboratory techniques as LED-FM smear microscopy for diagnosis of tuberculosis are cost effective but less sensitive as compared to the GeneXpert because the large bacillary load (105/mL) will be required for a smear to become positive.
In conclusion, specificity of GeneXpert is high in majority of EPTB cases with smear-positive non-respiratory samples. In addition, it has a high sensitivity for detecting EPTB samples like ascetic fluid and tissues. These findings support recent WHO guidelines regarding the use of GeneXpert for TB diagnosis from EPTB specimens.
Conflicts of interestThe authors declare no conflicts of interest.