





Chronic low back pain is a major cause of disability. The most effective intervention is exercise, with higher benefits in terms of pain and function.
ObjectiveKnowing the level of adherence to therapeutic exercise is essential to assess the effectiveness of health services, for planning strategies, optimising resources, and promoting the full recovery of patients in less time.
Material and methodsA prospective, observational study with 6 months follow-up was performed on 31 patients with chronic low back pain who underwent a lumbar stability programme. Rating scales for pain, function, anxiety, depression and fear of avoidance were applied. Adherence was recorded using daily therapy diary. Parametric tests were performed to determine correlations of interest, and to evaluate the changes presented over time.
ResultsThe percentage of adherence was 82–84% during the 3 trimesters. There were no correlations between adherence and socio-demographic variables, depression, anxiety, or fear of avoidance. Patients categorised as adherent showed faster and more significant improvements in pain and function (p>0.05).
ConclusionsAt the end of the study all patients had a significant improvement in pain and function. Depressed patients showed higher scores on scales of pain and disability at the beginning and end of the study. However, neither depression, anxiety, nor fear of running activity were predictors of non-adherence to the therapy.
El dolor crónico de espalda baja es una de las principales causas de discapacidad. La intervención más eficaz es el ejercicio, con un beneficio superior en términos de dolor y funcionalidad.
ObjetivoConocer el grado de adherencia a los programas de ejercicio terapéutico es indispensable para evaluar la eficacia como servicios de salud, planificar estrategias, optimizar recursos, y favorecer la plena recuperación de los pacientes en un menor tiempo.
Material y métodosSe realizó un estudio prospectivo, observacional con seguimiento a 6 meses de 31 pacientes con dolor crónico de espalda baja, incluidos en el programa de estabilidad lumbar. Se aplicaron escalas de valoración para dolor, funcionalidad, ansiedad, depresión y miedo a la actividad física. Se registró la adherencia mediante un diario de terapia. Se realizaron pruebas paramétricas para correlaciones de interés, así como para determinar los cambios presentados en el tiempo de seguimiento.
ResultadosEl porcentaje de adherencia fue de 82-84% en cada trimestre. La adherencia no mostró correlaciones con variables sociodemográficas, depresión, ansiedad ni miedo. Los pacientes categorizados como adherentes mostraron una mejoría más rápida y evidente en cuanto al dolor y funcionalidad (p>0.05).
ConclusiónAl término del seguimiento todos los pacientes presentaron mejoría significativa en cuanto a dolor y funcionalidad. Los pacientes con depresión mostraron puntajes más altos en las escalas de dolor, funcionalidad al inicio y término del estudio. Sin embargo, ni la depresión, la ansiedad, ni el miedo a ejecutar actividad fueron factores pronóstico de no adherencia terapéutica.
Effective intervention for the treatment of chronic back pain is exercise, with higher benefits in terms of pain and function, compared with any other type of intervention.1
The advocacy of exercise programmes as “routines for doing at home” enables health care systems to manage a large volume of the population and respond to the growing demands for care, especially regarding chronic pains such as lower back pain, but it depends on the therapeutic adherence of patients to the indications given.
Despite the health service's efforts to obtain optimum management, it has been estimated that up to 45% of patients do not meet with therapeutic recommendations, and all the more so when the regimes consist of changes in habits or lifestyle (which include exercise), resulting in poorer treatment efficacy.2,3
Many factors are associated with poor therapy adherence, and they vary according to the population under study. Of these, personal factors stand out such as: lack of education, sedentarism, perception of physical fragility, fear or belief that physical activity could be harmful, associated depression or anxiety. Intrinsic characteristics to the treatment regime, the doctor–patient relationship and even socio-economic and environmental factors which facilitate or hinder fulfilment of a programme are also of influence.4
Despite the above, little has been reported regarding adherence to exercise and the factors which influence this in patients with chronic lower back pain.
ObjectiveTo assess the main factors related to the level of therapeutic adherence to the exercise programme for lower back pain stabilisation, in patients who are diagnosed with chronic lower back pain.
Material and methodsA prospective, observational study was conducted with a 6 month follow-up, in patients with a diagnosis of chronic lower back pain who presented at the external services of the Rehabilitation de Columna del Instituto Nacional de Rehabilitación centre and who agreed to participate subsequent to giving their informed consent. The protocol was approved by the Research Committee of the institution.
Older patients were included, regardless of gender, with a presence of mechanic type chronic lower back pain.
Patients who were illiterate were excluded as were those with a history of lumbar surgery, systemic rheumatic disease (rheumatoid arthrosis, systemic eritematous lupus, inflammatory spondiloarhtoropaties), polyneuropathy of any type, mainly diabetic, or neuromuscular diseases. Those who did not complete the assessments and 6 month follow-up were eliminated.
A calculation was made for the sample size, with the consideration of detecting a correlation coefficient when there was below 0.50 between the main variables, with an error index of under 0.05 (α) and a Statistical rate of 80%: the minimum requisite was 29 patients.
The Mc Gill Pain short-form Spanish version Questionnaire (SF-MPQ), was used for pain assessment. This questionnaire consists of 15 descriptors (11 sensory and 4 affective) where the patients gave a score of 0–3 depending on the intensity of their pain: none, mild, moderate or severe. A present pain intensity index was included, with response from “no pain” to “unbearable plain” and a Visual Analogue Scale (VAS). The outcome obtained was: assessment of pain applying the VAS with a score of 0–100. The number of pain descriptors chosen by the patient. The pain intensity index is the chosen response to the item which explores this aspect.5
Function was assessed using the Roland-Morris scale, which reflects limitations in daily activities related to chronic lumbalgia. This tool has proven to be reliable and with appropriate reproductibility for measuring incapacity.6
The level of therapeutic adherence is measured using the Sluijs scale which is a questionnaire which assesses the frequency and duration of exercise the patients with chronic lower back pain do at home, for a week.7
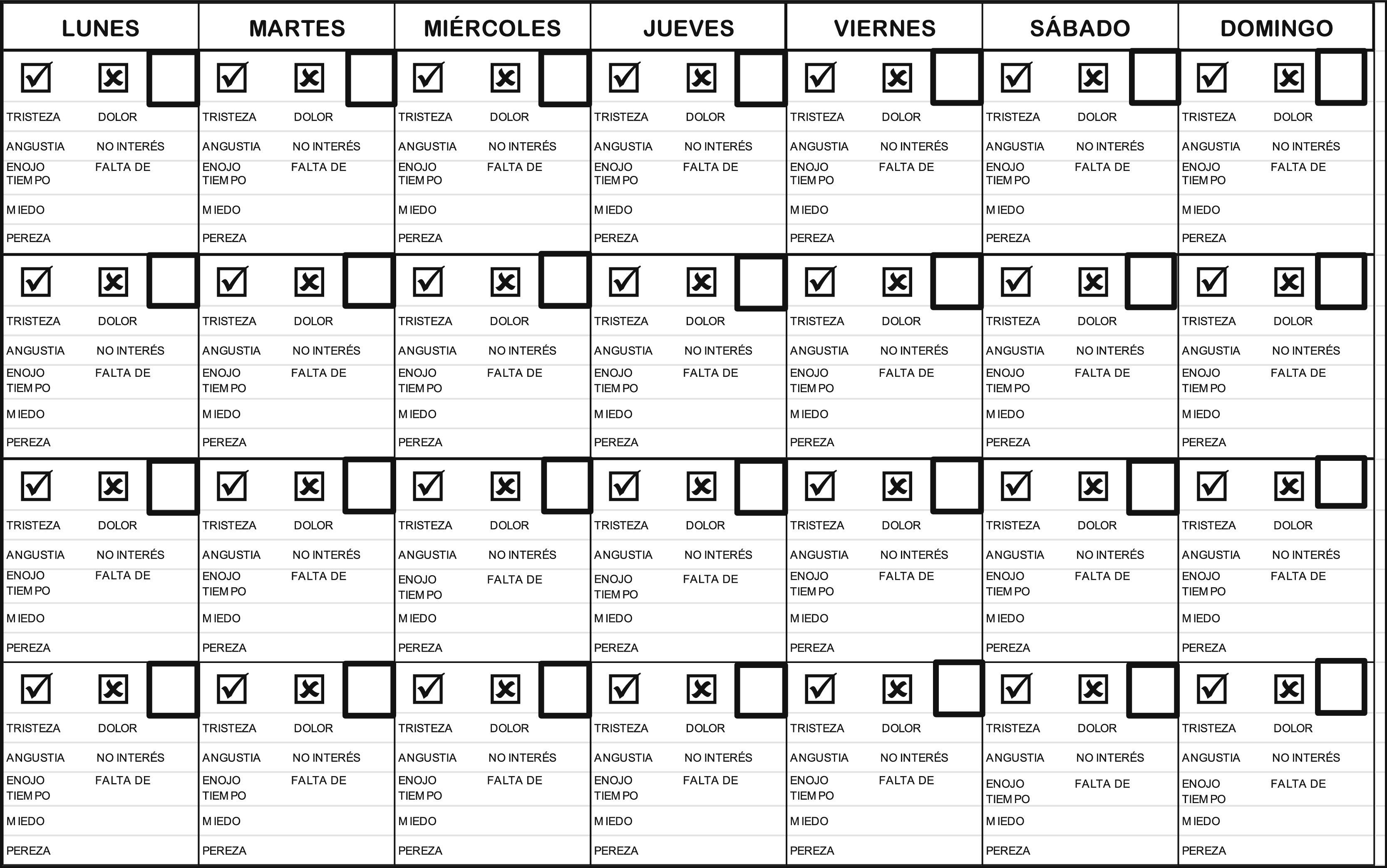
Quantitative measurements of adherence are made by the percentage of exercise adherence. This was measured by applying a therapy diary at home, designed for this study and driven by recommendations in the literature.8 Each follow-up month all patients were given the diary. If the patient did not do the exercise one day, they were given the possibility of selecting the reason why this task had not been completed (Fig. 1).

Assessment of psychological components relating to chronic lower back pain was applied with the Hospital Anxiety and Depression Scale (HADS) scale. This filter is used to detect symptoms of anxiety and depression.9
Assessment of fear and beliefs held with regard to physical activity in the case of chronic lower back pain was made with the Fear Avoidance Beliefs Questionnaire (FABQ) questionnaire, which consists of 16 items which are graded from 0: totally disagree, to 6: totally agree. The higher scores indicate a higher degree of fear and avoidance belief, divided into a subscale of physical activity and other work activities. Scoring is done by adding up the points obtained as results: 7 of the 11 items relating to work (FABQ-W) within the range of 0–42 points and 4 out of 5 items relating to physical activity (FABQ-PA), within the range of 0–24 points; a high score is considered in FABQ-PA when the score is over 14.10–12
All the tools used were previously translated and validated for use in our sample.
ProcedureIn the first assessment the data collection format was completed: socio-demographic, relevant clinical, filtering for depression, fear and anxiety, and also the application of the initial FAB, Roland Morris and Mc Gill scales. Furthermore a diary for recording therapy was explained and distributed together with the Sluijs scale, which was filled in weekly.
After the initial assessment the patients were seen monthly to exchange the therapy diary and the Sluijs scale. At the end of the third and sixth month they re-applied the pain and function scores.
All the patients did the same activities, which began with the application of a hot, wet compress, followed by a routine of muscular stretches and lumbar stabilisation exercise for the management of patients with chronic lower back pain.13
Statistical analysis was carried out with version 20.0 (SPSS) of the Statistical Package for Social Sciences. Descriptive statistics were conducted to synthetisize data. Sample behaviour was determined using the Kolmogorov–Smirnov test and distribution was found to be normal. Parametric tests (Pearson and Student's t-test) were chosen to study the relationship between the primary variables such as pain, function and percentage of therapeutic adherence and the remaining variables of interest.
One-way Anova analysis of variance was used with covariance adjustment to determine the changes between initial scores and follow-up after 6 months. General lineal models were also made for repeated measurements to determine the changes over time for pain, function and therapeutic adherence. The level of significance was established at 0.05.
ResultsInitially 39 patients were assessed. After 6 months only 31 patients completed the follow-up. Of the 8 patients who were eliminated, 6 only completed the first month of follow-up and did not attend a re-assessment (one due to the illness of a close family member and the others for unknown reasons). Two patients completed 3 months of follow-up and did not attend the final assessment (one due to heart problems and the other for unknown reasons).
Of the final sample (31 cases), 21 were female (67.74%) and 10 male (32.2%) with an average age of 48±11.32 years. Body mass index was 27.6±4.1. Average time for the development of chronic lower back pain was 4.5±4.32 years.
Regarding socio-demographic data, 40.7% of patients were married, followed by singles (37%), divorcees (18.5%) and those living with partners (3.7%). Education levels were mainly upper middle (secondary and baccalaureate/university preparation with 37% for each level), followed by primary (18.5%) and further education (7.4%).
The majority of patients who went to the service came from the Federal District with a total of 19 patients (61%) and the others from the State of Mexico (12 patients, 39% of the sample).
The patients’ occupation was classed as high or low risk for chronic lower back pain, 81% of whom had activities which were high risk.
Only 8 patients (29.6%) reported being unemployed as a result of the chronic lower back pain, whilst the great majority (66.7%) referred to themselves as active in their job and financially independent.
78% (24 cases) of patients did not practise any regular physical activity prior to the assessment.
The instructed exercises were in 3 modalities: 6 patients went to 10 sessions to learn the programme, 7 went to 5 sessions, and 18 received one session to then continue doing the exercises at home. The distribution in these modalities was determined by patient preference (i.e. whether they wanted one session or several to learn the programme), without modifying the routine of the exercise which they later continued to do at home.
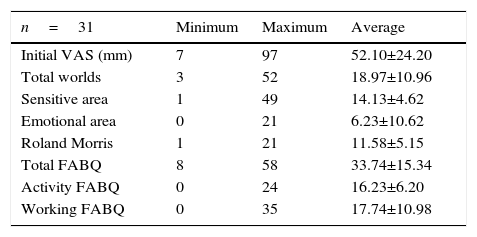
The baseline results on the assessment scales for pain, function and application of the FABQ scale for fear and physical activity beliefs are shown in Table 1.
Baseline results of the scales applied to assess pain (Mc Gill questionnaire), function, and avoidance and fear of physical activity.
| n=31 | Minimum | Maximum | Average |
|---|---|---|---|
| Initial VAS (mm) | 7 | 97 | 52.10±24.20 |
| Total worlds | 3 | 52 | 18.97±10.96 |
| Sensitive area | 1 | 49 | 14.13±4.62 |
| Emotional area | 0 | 21 | 6.23±10.62 |
| Roland Morris | 1 | 21 | 11.58±5.15 |
| Total FABQ | 8 | 58 | 33.74±15.34 |
| Activity FABQ | 0 | 24 | 16.23±6.20 |
| Working FABQ | 0 | 35 | 17.74±10.98 |
VAS: Visual Analogue Scale; FABQ: Fear Avoidance Beliefs Questionnaire.
The results of the HADS scale for depression: 15 patients negative (48.3%), 13 borderline (41.9%) and 3 positive (9.6%); for anxiety: 17 patients negative (54.8%), 6 borderline (19.3%) and 8 positive (25.8%).
No significant differences were found regarding gender, with regards to the initial pain assessment (VAS and Mc Gill), function (Roland Morris) and the FABQ fear scale (p≥0.05 in all tests).
Equally, the influence of depression or anxiety was studied on pain variables, higher scores being found in initial and final scales for patients with depression (p=0.015 the first month; p=0.048 the third month; p=0.03 the sixth month), but no influence being found for those patients with anxiety (p≥0.05 in all tests).
Correlations between scores on the initial FAB scales and the pain and function scales were researched, with only correlation being found between the total score on the FAB scale regarding initial function (p≥0.045), but which this was not maintained at 6 months.
Time of development, age, weight, or size had no effect on pain and function scores.
Regarding the effect of depression or anxiety on function variables, we observed higher scores in the Roland Morris questionnaire (greater dysfunction), for both the initial assessment and in the sixth month in those patients with depression compared with those who scored negatively or with borderline (p=0.015 scores in the first month; p=0.048 the third month; p=0.03 the sixth month). These results are shown in Tables 2 and 3.
Correlation of pain with depression at the beginning and end of the study.
| Diagnosis of depression according to the HADS scale | Initial average VAS (mm) | Final average VAS (mm) |
|---|---|---|
| Negative (n=15) | 43.40 | 30.20 |
| Borderline (n=13) | 57.46 | 46.62 |
| Depression (n=3) | 72.33 | 71.67 |
| p=0.093 | p=0.007 |
VAS: Visual Analogue Scale; HADS: Hospital Anxiety and Depression Scale.
Correlation of pain with incapacity at the beginning and end of the study.
| Diagnosis of depression according to the HADS scale | RM initial average (score) | RM final average (score) |
|---|---|---|
| Negative (n=15) | 10.67 | 7.20 |
| Borderline (n=13) | 11.00 | 8.92 |
| Depression (n=3) | 18.67 | 17.67 |
| p=0.036 | p=0.013 |
HADS: Hospital Anxiety and Depression Scale; RM: Roland Morris Questionnaire.
The therapeutic adherence averages measured in days and the number of patients adhering to treatment according to the Sluijs scale at the first, third and sixth month of development is shown in Table 4.
Adherence to therapy in the sample studied.
| n=31 | % of execution per month (total days) | Average in days | Adherent patients according to the Sluijs scale |
|---|---|---|---|
| Adherence to therapy the first month | 82.39 | 23.07±7.01 | 24 |
| Adherence to therapy the third month | 85.85 | 24.04±5.37 | 20 |
| Adherence to therapy the sixth month | 82.14 | 23.00±8.61 | 22 |
Adherence was not influenced by the number of sessions provided for the learning of the exercise routine. In addition to this, the possible correlations between these socio-demographic variables and therapeutic adherence were analysed, with no significant results.
Patients were asked to state the most frequent reasons why they did not do the exercises, and the main reasons stated was “lack of time” (37% the first month, 40.7% the third month and 33.3% the sixth month), followed by “pain” in the first and the third month (14.8% in both months) and “fatigue” as the second cause in the sixth month.
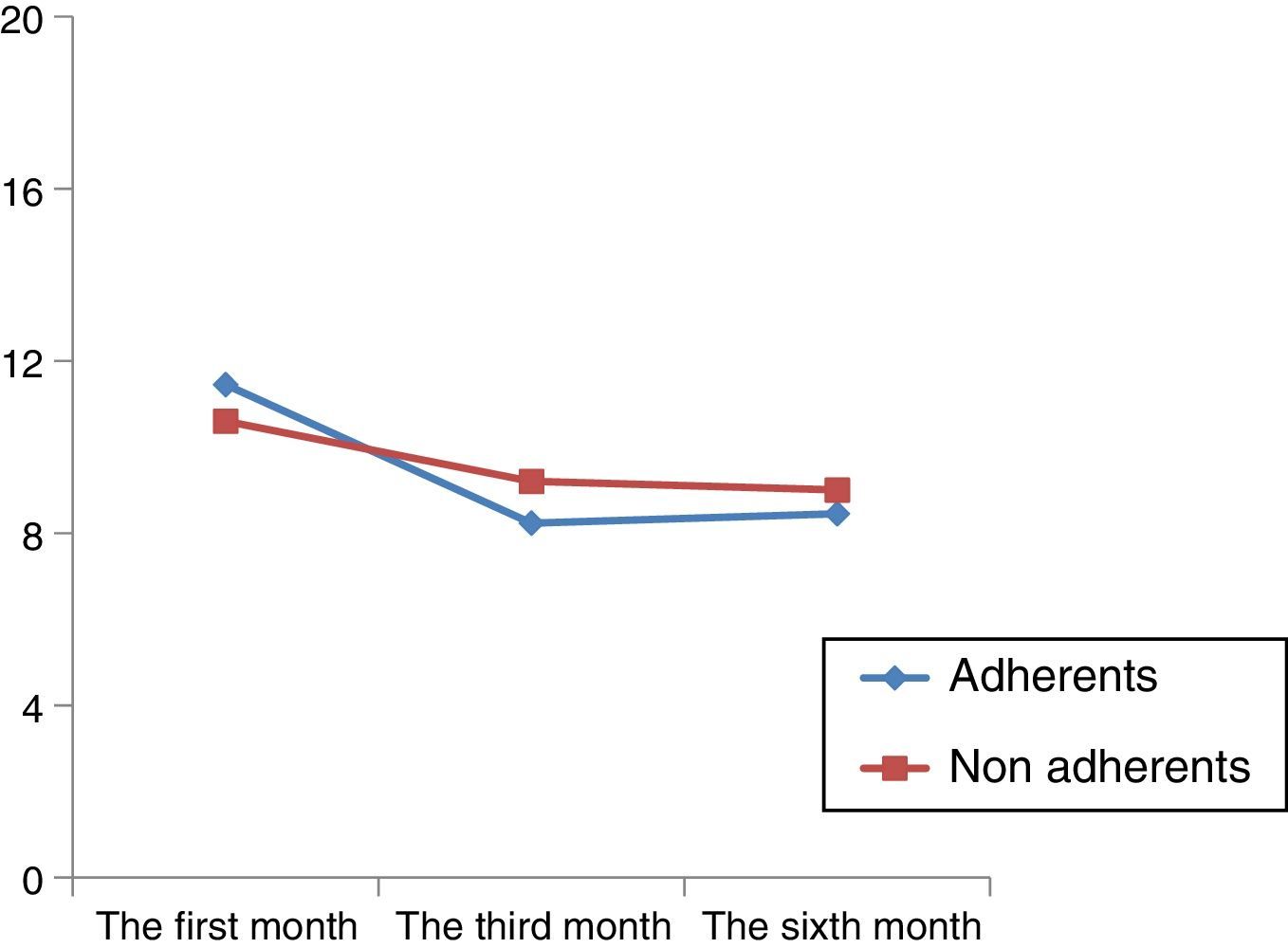
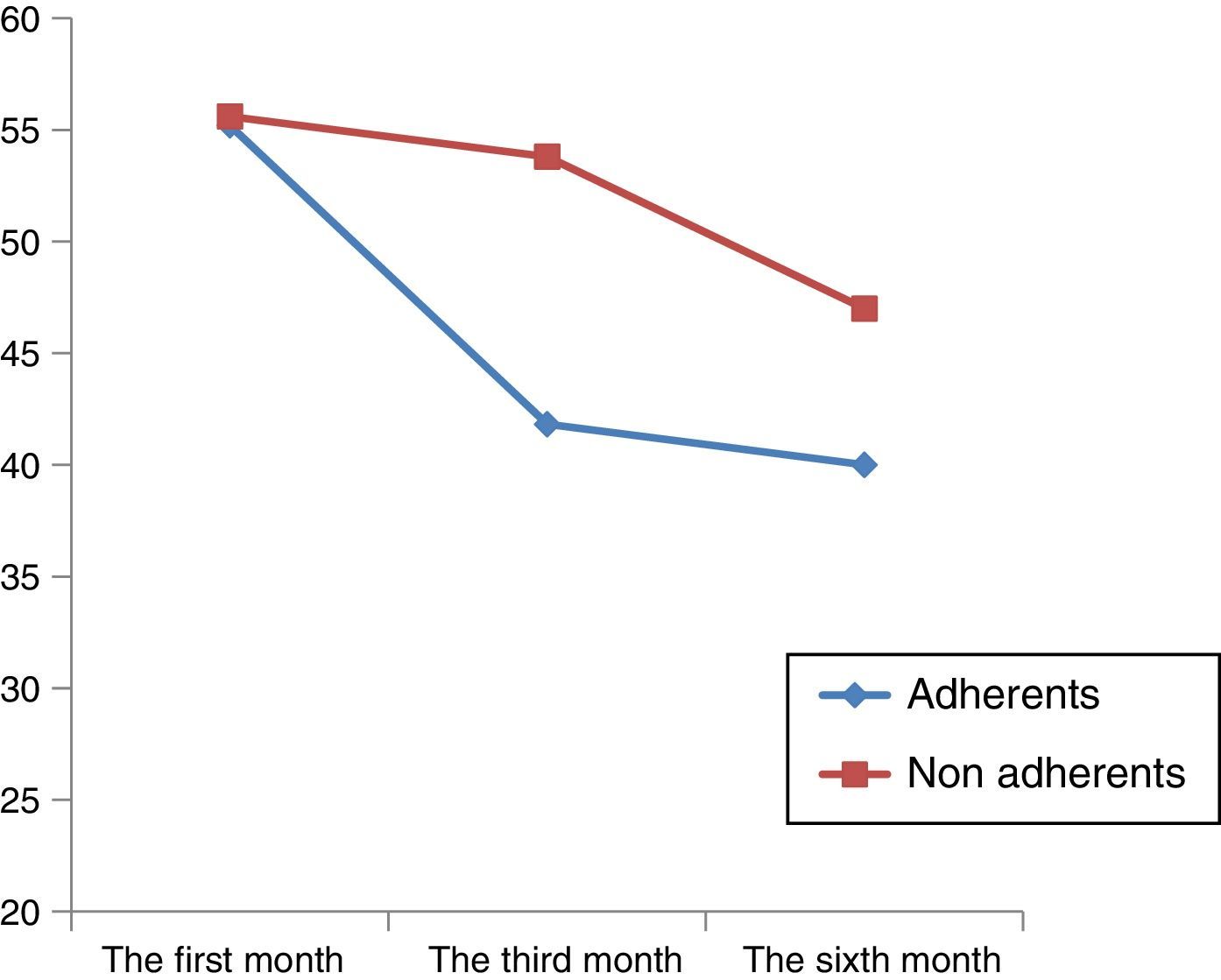
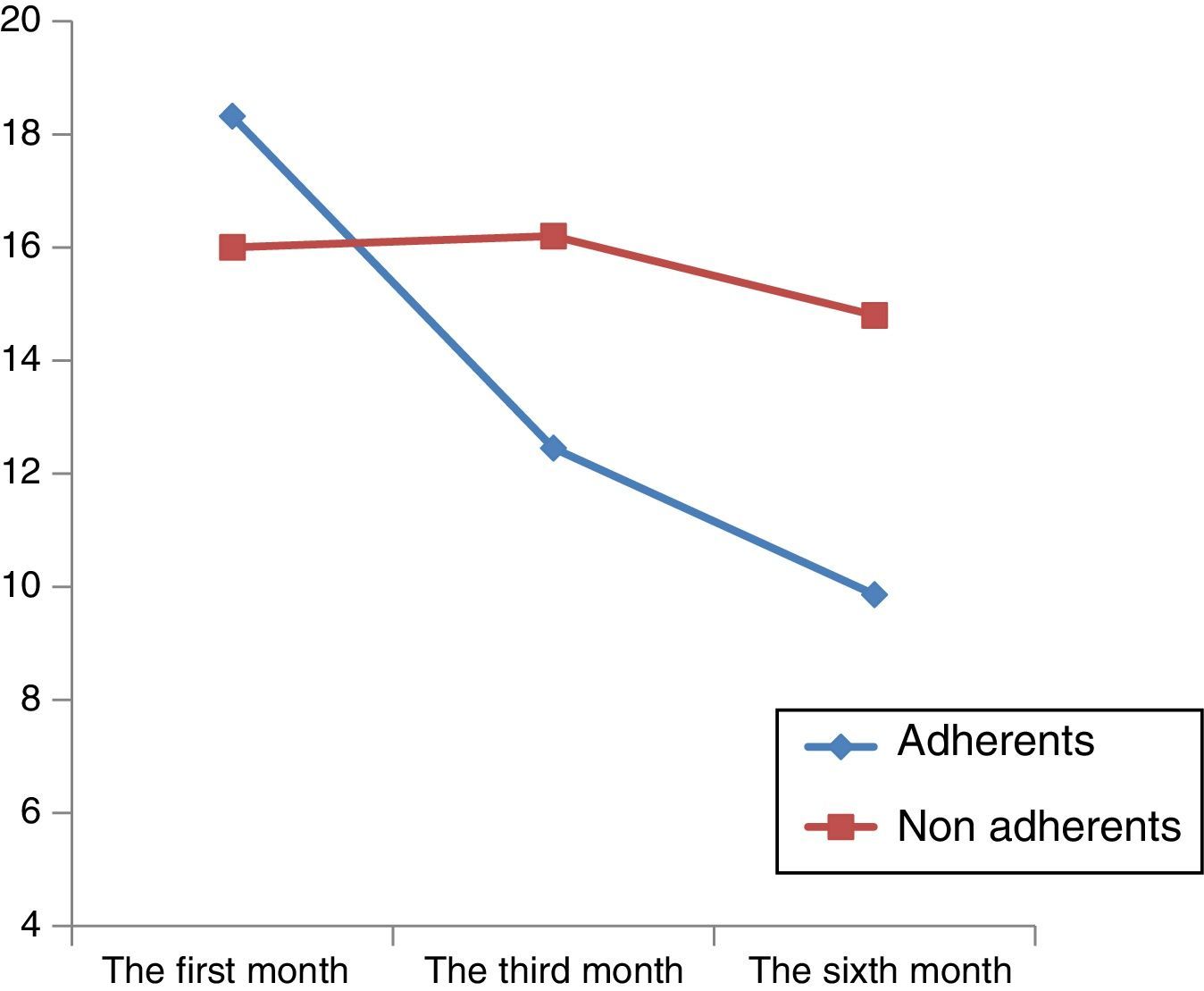
Patients were classified as adherent or non adherent using the Sluijs scale and observing the difference in scores obtained for pain control and function, according to the application of a linear model of repeated measures and it was found that both groups (adherent and non adherent) presented improvements in the measures of the evaluated outcome, the fastest being in the group of patients who were adherents, which was also related to a significant tendency regarding time (Figs. 2–4).

Graph showing the pattern of function between groups over time according to the classification of adherence using the Sluijs scale. The “X” axis represents review after one month, 3 months and 6 months of assessment and the “Y” axis represents the average functional incapacity score when applying the Roland Morris questionnaire.

Graph showing the pattern of pain between groups over time according to the classification of adherence using the Sluijs scale. The “X” axis represents review after one month, 3 months and 6 months of assessment and the “Y” axis represents the average pain score when applying the Visual Analogue Scale.

Graph showing the pattern of pain between groups over time according to the classification of adherence using the Sluijs scale. The “X” axis represents review after one month, 3 months and 6 months of assessment and the “Y” axis represents the average score of the total descriptors selected for pain when applying the McGill Pain Scale.
The measurements made in our study (first, third and sixth month) show that therapeutic adherence did not change with fear, beliefs in physical activity, the presence of depression or anxiety, age, time of development, function (Roland Morris) nor pain (initial, intermediate and final Mc Gill scale) with a value of p≥0.05 for all tests.
The patient characteristics of those patients who withdrew from the study prior to the 6-month follow-up were also analysed, to compare potential differences between patients who continued adhering to the programme. Here we found that their average pain score (VAS and Mc Gill) and the score for incapacity was lower in its initial evaluation, compared with those patients who continued with the programme, with this difference being significant.
DiscussionChronic lower back pain is a major public health problem in our country and this is due to poor treatment programme adherence, which requires active participation of the patient doing regular exercise and leading a healthy lifestyle.1 It has been found that withdrawal from therapy is higher than 40%; however, in our study adherence to the exercise programme was higher (none was under 20% during the whole follow-up) and these differences are possibly related to the monthly review, the use of a therapy diary and patient motivation through reduction of symptoms. These factors were previously reported as positive for therapeutic adherence by Bentsen et al.,14 who carried out follow-up for 3 years on 74 patients who were diagnosed with chronic lower back pain.
The main reasons reported for not doing exercise in our study was lack of time, coinciding with that reported by Slade et al. in 2014.15
Contrary to our expectations, we did not find that beliefs and fear of physical activity, the presence of depression or anxiety, assessment time, functional incapacity or pain were factors which directly affected therapeutic adherence for the 6 months of follow-up. These results are contradictory to those reported by Henchoz et al.,16 who describe that a lower educational level, the presence of depression and greater evolution time, together with functional incapacity are poor adherence factors. However, in their study the mean age was 67 (and in our study it was 48), and it is therefore probable that this included a higher percentage of patients with degenerative processes in their spines, and that the sample differences affect the outcome of motivation to do exercise, as well as comorbitity with other factors such as depression, which in the mentioned study included up to 30% of the sample.
Despite the above, we must be cautious about our results, since 40% of the initial sample did not complete the 6 month follow up and neither do we know what results were obtained, due to difficulties in contacting the patients. In future research, pertinent strategies will be taken, in order to observe whether the reason that the sample under study did not complete the follow up period could have been due to the fact that even initially they were patients who did not adhere to treatment, nor filled in their evaluations and probably did not do the exercises either.
By analysing the patient characteristics of those who did not complete the assessments, we find that on average these patients obtained low scores for incapacity and pain, and these “low scores” are probably the result of them feeling less motivated to continue long term with the treatment, due to the fact that their symptoms were mild and more tolerable in their regular lifestyle. The above coincides with the results reported in 2007 by Kovacs et al.,12 and in 2010 by Henchoz et al.,16 who in the Spanish population highlighted that avoidance beliefs and attitudes towards physical activity on the FAB scale did not appear to influence the perception of pain and function in patients with chronic lower back pain; contrary to our study, where we found there was an association between higher scores on the FAB scale and functional incapacity, which coincides with populations such as England, Switzerland, Germany and France.
Depression is one of the main factors related to incapacity, reporting in this study with higher scores for pain and incapacity in those patients with depression, which coincides with Karp et al.17, who believe that this association may generate a vicious circle of demoralisation, physical disability, psycho-social disability, and medical and psychiatric comorbidity.
One of the key findings from our study was that those patients who formed part of the group with adherence to the routine of exercises for lumbar stabilisation showed a reduction in pain, with functional improvement, and that this improvement presented more quickly than in non patients. Although the non adherent group also improved at the end of the study, the gain was at a lower level. It may therefore be deduced that the strongest predictor of improvement could be therapeutic adherence.18
Another appreciated factor was the number of therapy sessions which were granted within the institution. This variable does not appear to affect adherence to the programme or the functional outcome, coinciding with that reported by Bentsen et al.19
Adherence appears to be more strongly related to several strategies such as: patient information and advice, and reinforcement techniques and that they have proven to be important points of the motivational programme for obtaining positive results.20
In 201415 Slade et al. reported that adherence to treatment increases with: printed supplementary material, supervision, motivation strategies, clinical follow up and positive reinforcement. In addition to these, the suggestion of goals to be aimed at and established contracts between the therapist and participating patient are important.
In our study the patient was able to feel motivated by filling in the therapy diary, and for this to have worked as a facilitator to adherence.
Another aspect which has been described as enhancing adherence is the recognition by the patient or by the doctor of goals achieved. This is referred to as the best predictor of persistent physical activity, together with conviction that exercise will improve health and reduce stress.21
In general, patients feel stimulated to continue exercising when they have regular contact with a health professional and when they have the perception of feeling understood. One must not forget that, in the presence of lower back pain together with depressive symptoms, it is of vital importance to treat both situations simultaneously.
Mention should be made of the main limitation of our study which was the loss of patients with a limited follow up through hindrances in contact, and that several questions remained unanswered. What are the factors limiting their follow up? If we had been aware of these data strategies aimed at this patient group could have been offered.
ConclusionOn termination of follow up, all patients had achieved significant improvement with regards to pain and function. The scores for pain and function were greater in patients with depression at the beginning and end of the study. Socio-demographic factors, beliefs and fear of physical activity, the level of function, pain, depression and anxiety, did not show up as prognostic factors in therapeutic adherence to the lumbar stabilisation programme in our study.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Nava-Bringas TI, Roeniger-Desatnik A, Arellano-Hernández A, Cruz-Medina E. Adherencia al programa de ejercicios de estabilización lumbar en pacientes con dolor crónico de espalda baja. Cir Cir. 2016;84:384–391.