




Intestinal duplication cysts are rare in adults.1–7 They are usually diagnosed in childhood after causing symptoms in the early years of life.
They can appear throughout the entire digestive tract, although the ileum is the most frequent location. Their malignization is not unusual, but there are few reports in the literature.1,2
We present the case of a patient treated surgically for an intra-abdominal mass of uncertain origin that ultimately turned out to be an advanced adenocarcinoma on an intestinal duplication cyst in the jejunum.
The patient is a 59-year-old male patient with a recent hypertensive crisis who presented a non-painful, immobile, indurated mass in the left hemiabdomen on examination.
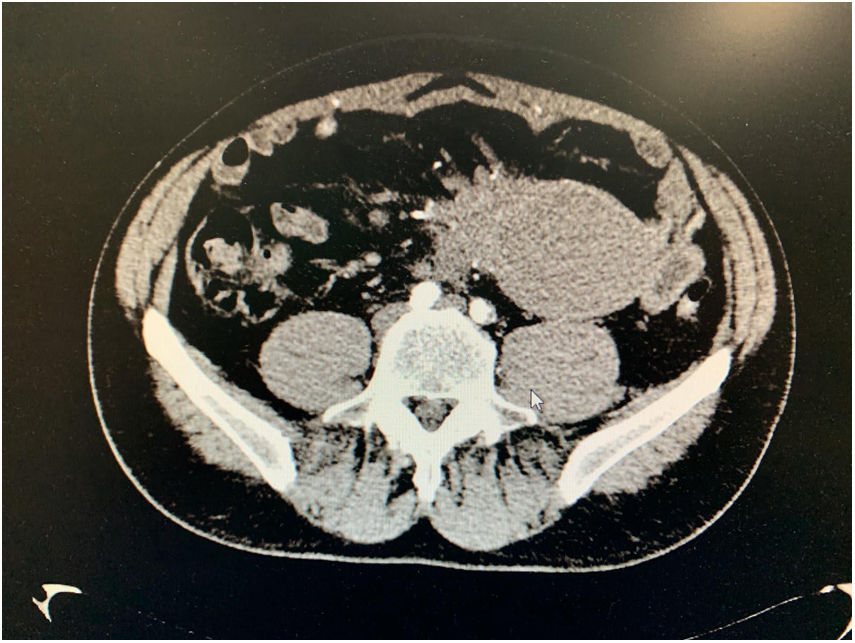
A computed tomography (CT) scan detected a solid cystic mass that depended on the mesentery and seemed to trap the right ureter, causing ipsilateral hydronephrosis (Fig. 1).

Lab work showed a creatinine level of 1.61 mg/dL, and renogram found a right renal function of only 10.2%, possibly due to extrinsic compression. Therefore, we performed right double J catheter placement.
Colonoscopy detected an area of suspected submucosal infiltration, which was not confirmed by biopsy.
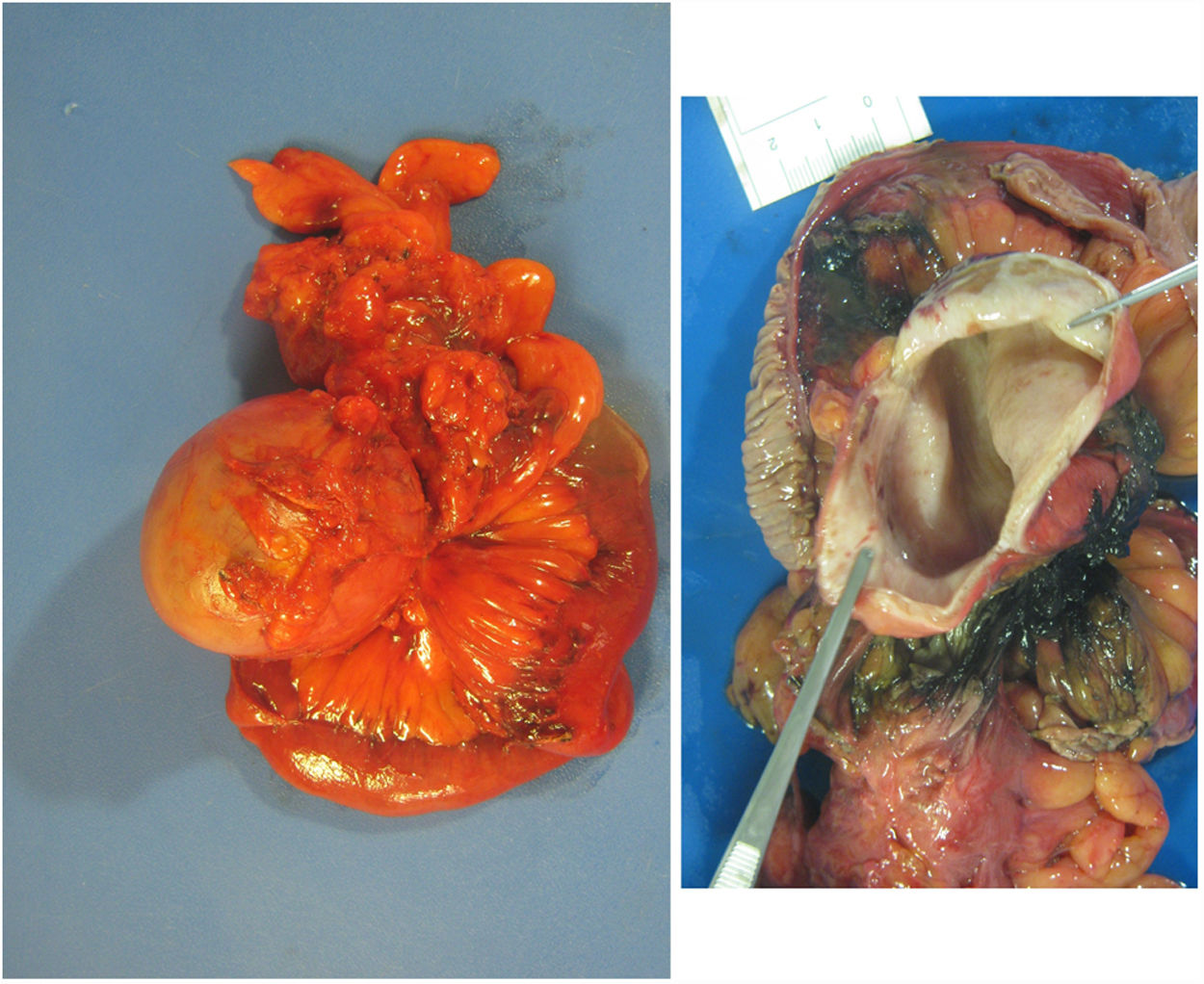
Given these findings, we decided to perform exploratory laparotomy. An intestinal mass of about 8 cm was observed near the angle of Treitz, which affected the root of the mesentery, encompassed the sigmoid colon and respected the superior mesenteric artery and vein, as well as the right ureter.
En bloc excision of the mass was performed, including the affected proximal jejunum and sigmoid colon (Fig. 2).

During the postoperative period, the patient presented dehiscence of the jejunal anastomosis 48 h after surgery, requiring urgent laparotomy. We performed Kocher’s maneuver and complete mobilization of the angle of Treitz. The duodenum distal to the papilla was dissected after direct visualization, and the jejunum was moved to the retromesenteric space, creating a side-to-side duodenum-jejunal anastomosis on the free side of the second portion.
The patient required admission to the resuscitation unit (grade IVa Clavien-Dindo classification) and was discharged 13 days after admission.
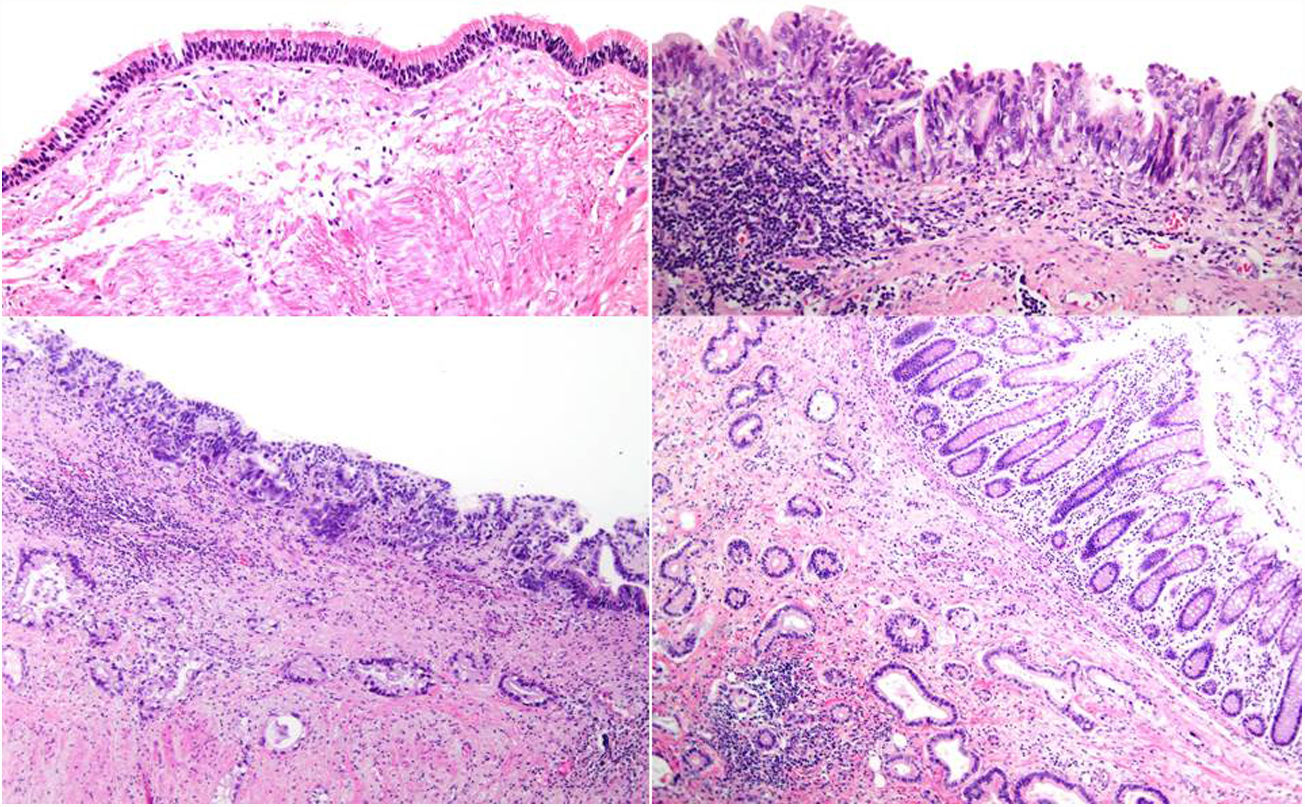
The final results of the pathology study identified a small bowel adenocarcinoma that invaded the mesentery and a colon segment (pT4), with affected radial margin and presence of lymph node infiltration (pN2), vascular and perineural invasion, and continued expression of repair proteins (Fig. 3).
.")
Intestinal duplication cyst with no relationship with the lumen of the small intestine, covered by dysplastic intestinal-type epithelium, extensive areas of carcinoma in situ, and bare areas. The cyst shows 2 developed muscle layers in the entire extension, with the presence of Auerbach’s plexus and lymph node cells. An invasive component of adenocarcinoma is identified, invading lymph nodes, nerves structures and vein structures (intra-/extramural).
With a diagnosis of stage IIIC, adjuvant chemotherapy was initiated with capecitabine and oxaliplatin. The planned treatment was completed for 24 weeks, with a subsequent 14-month follow-up.
Intestinal duplication cysts are a congenital disease that can occur at any level of the digestive tract.1–7 Their diagnosis can be complicated by their low incidence and because they are observed in childhood in most cases, within the first 2 years of life (70%).2 The origin of these duplications is still controversial, although a multifactorial cause has been proposed, including theories such as twin gestation, persistent embryonic diverticulum, or aberrant luminal recanalization. Currently, one of the most widely accepted theories is the explanation through intrauterine vascular accidents.2–5 These are frequently located on the mesenteric side of the intestine, as in the case of our patient, and in order of appearance they are located in the ileum, esophagus, rectum and colon.2 The presence of ectopic tissue (gastric, pancreatic) can cause symptoms of hemorrhage, ulceration and even perforation, so it is not surprising that they end up being diagnosed and operated on urgently.2,5
Imaging tests such as ultrasound, computed tomography or magnetic resonance imaging are recommended for diagnosis. Once the diagnosis is made, the treatment of choice is complete surgical resection.
In adults, the diagnosis of these duplications can occur as complications (occlusion, bleeding, pain) and surgical resection is also indicated by the risk of malignancy.
The diagnosis of malignancy on these lesions is rare, with a small number of published case reports. It occurs more frequently in the colon, with a percentage of malignancy for this type of cysts of up to 68% in some published series,8 and 23% in ileal cysts.9 The most common histological type is adenocarcinoma, followed by squamous carcinoma and carcinoid tumor.10 The diagnosis is also usually made in advanced stages, as in the case of our patient, frequently with the presence of lymph node involvement.
Surgery must be radical, with a curative intent from the outset.1,2
Although rare, intestinal duplication cysts can be diagnosed in adults, and this diagnosis must be contemplated in cases of abdominal mass of unknown origin. Knowing that malignization is possible, surgery should be the initial therapeutic option, and radical resection should always be carried out with curative intent.
Juan José Segura-Sampedro and Rafael Morales-Soriano
Please cite this article as: Craus-Miguel A, Bianchi A, Pagan-Pomar A, Torralba Cloquell I, González-Argenté XF. Adenocarcinoma sobre quiste de duplicaciόn yeyunal. Cir Esp. 2021;99:66–68.
