




Ectopic decidua or deciduosis is the presence of decidual cells outside the endometrium. This condition can affect the ovaries, uterine serosa, fallopian tubes or cervix. Less frequently, it can affect the appendix, diaphragm, liver, spleen, retroperitoneal lymphatic tissue or renal pelvis.1 The ectopic decidual cells located in the subceloma stroma may represent a physiological reaction secondary to the stimulation of progestogens.2 Usually, the condition is asymptomatic and regresses during the weeks after childbirth, but may reappear in later pregnancies. Occasionally, it may appear in the form of abdominal pain during pregnancy or as appendicitis in 0.05%–0.13% of cases.3–6 In the international literature, only 10 cases of deciduosis of the appendix during pregnancy have been described7–9 (Table 1), so we therefore present our case.
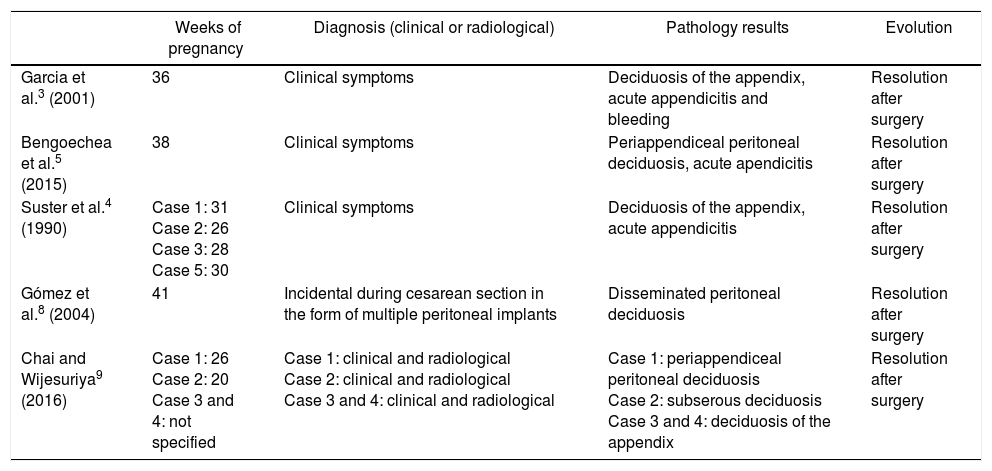
Internationally Published Cases of Deciduosis of the Appendix.
| Weeks of pregnancy | Diagnosis (clinical or radiological) | Pathology results | Evolution | |
|---|---|---|---|---|
| Garcia et al.3 (2001) | 36 | Clinical symptoms | Deciduosis of the appendix, acute appendicitis and bleeding | Resolution after surgery |
| Bengoechea et al.5 (2015) | 38 | Clinical symptoms | Periappendiceal peritoneal deciduosis, acute apendicitis | Resolution after surgery |
| Suster et al.4 (1990) | Case 1: 31 Case 2: 26 Case 3: 28 Case 5: 30 | Clinical symptoms | Deciduosis of the appendix, acute appendicitis | Resolution after surgery |
| Gómez et al.8 (2004) | 41 | Incidental during cesarean section in the form of multiple peritoneal implants | Disseminated peritoneal deciduosis | Resolution after surgery |
| Chai and Wijesuriya9 (2016) | Case 1: 26 Case 2: 20 Case 3 and 4: not specified | Case 1: clinical and radiological Case 2: clinical and radiological Case 3 and 4: clinical and radiological | Case 1: periappendiceal peritoneal deciduosis Case 2: subserous deciduosis Case 3 and 4: deciduosis of the appendix | Resolution after surgery |
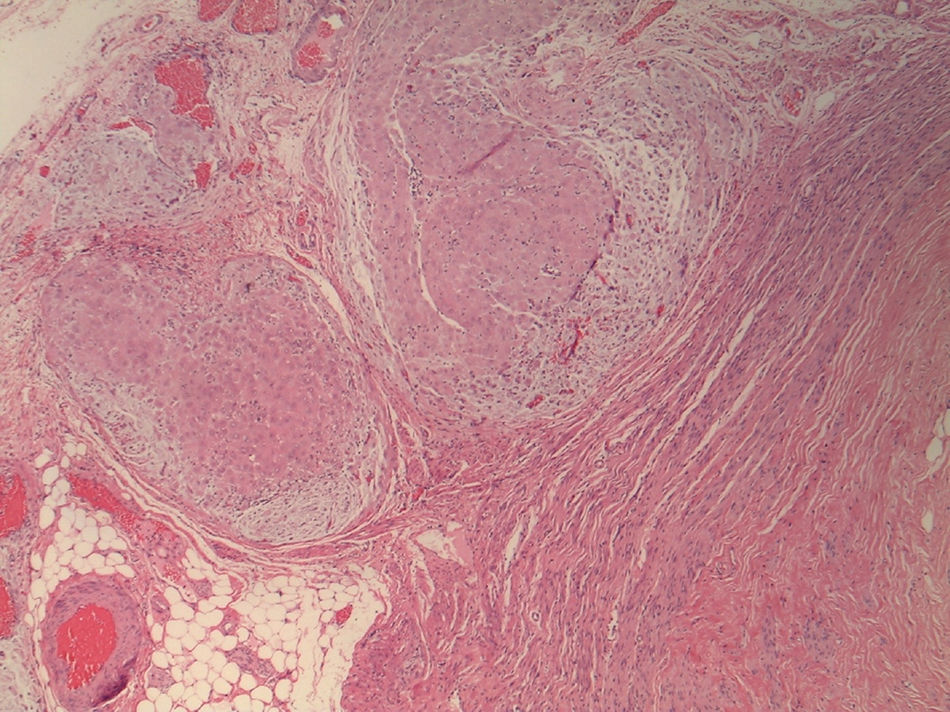
The patient is a 32-year-old woman with a history of endometriosis. At 23 weeks of pregnancy, she came to the emergency room with acute abdomen that had been progressing over the previous 12h. Examination of the abdomen showed a palpable uterus in the umbilical area and pain predominantly in the right flank. Gynecological examination, ultrasound and amniocentesis detected no alterations. Blood work demonstrated leukocytosis. The appendix could not be visualized on ultrasound or MRI, although free fluid was observed between the bowel loops. Given the suspicion of acute appendicitis, exploratory laparoscopy was performed, which revealed suppurative appendicitis, and appendectomy was conducted. The pain subsided after the appendectomy, and the postoperative period was uneventful. The histological study observed solid nests of decidual cells in the appendicular wall, at the levels of the muscularis propria, subserosa and serosa, compatible with deciduosis of the appendix. Neutrophil polymorphonuclear leukocytes were not identified in the total inclusion of the surgical piece (Fig. 1).

Deciduosis is an asymptomatic process associated with pregnancy, although in some cases it may present with symptoms of acute abdomen and should be included in the differential diagnosis as a possible cause in pregnant patients. The clinical presentation in the form of acute appendicitis could be attributed to peritoneal irritation due to mechanical factors associated with the response of the ectopic decidua to the estrogenic stimulus, or humoral factors since the decidua contains large concentrations of prostaglandins that act as a powerful muscle stimulant. Excessive secretion of microsomal acid phosphatase by decidual cells may increase the synthesis of prostaglandins, causing contraction of the appendix muscle wall.4 The case we present corresponds with appendicular deciduosis with acute abdominal symptoms during the second trimester of pregnancy whose symptoms completely subsided after appendectomy.
Please cite this article as: Luna Aufroy A, Orellana Fernández R, Novell Grau M, Ferreres Piñas JC, Navarro Soto S. Deciduosis apendicular como causa de abdomen agudo. Cir Esp. 2018;96:383–384.
