





Iatrogenic perforation during a diagnostic or therapeutic colonoscopy is one of the complications that is most feared by endoscopists; it occurs in 0.1% to 0.3% of cases.1,2 These perforations usually take place in the rectum and sigmoid colon at the start of the examination, and their management is controversial and entails high morbidity and mortality. We present a case treated with the Ovesco® clip system.
The patient is a 74-year-old woman with a history of diabetes, hysterectomy and sigmoid adenocarcinoma surgery 9 years before. Scheduled colonoscopy was done under light sedation as part of the follow-up of the colonic neoplasm. The patient was well prepared and asymptomatic before the study. During the manoeuvres at the start of the examination and after having advanced some 30cm over normal mucosa, a perforation occurred when the end of the colonoscope clearly entered into the peritoneal cavity and was immediately withdrawn.
At that time, we decided to mount the Ovesco® system (Ovesco Endoscopy GmbH, Tübingen, Germany) on another colonoscope and the clip was placed with endoscopic guidance. The perforation was considered to be sealed. Afterwards, we assessed the possibility of ordering a CT scan with oral and rectal contrast in order to rule out any possible leaks, but the patient presented signs of progressive peritoneal irritation and growing abdominal distension, so a joint decision was made with the General Surgery Unit to proceed with urgent laparotomy. During the exploratory procedure, we verified that the point of perforation in the sigmoid colon, which was approximately 1cm in diameter, was correctly sealed and there were no signs of peritonitis (Fig. 1). A few days later, the patient was asymptomatic and tolerated oral intake, enabling her to be discharged.

When faced with a colonic perforation during a diagnostic or therapeutic procedure of up to 2cm, endoscopic closure by means of clips like the Ovesco® is an option to consider in order to avoid the leakage of intraluminal content to the peritoneal cavity and to limit the consequences of the injury. This system has been used in gastrointestinal bleeding haemostasis, the closure of fistulas and gastrointestinal perforations,3–6 and also for sealing the digestive tube wall after submucosal endoscopic dissection procedures for tumour lesions or after NOTES surgery7,8 (Fig. 2).
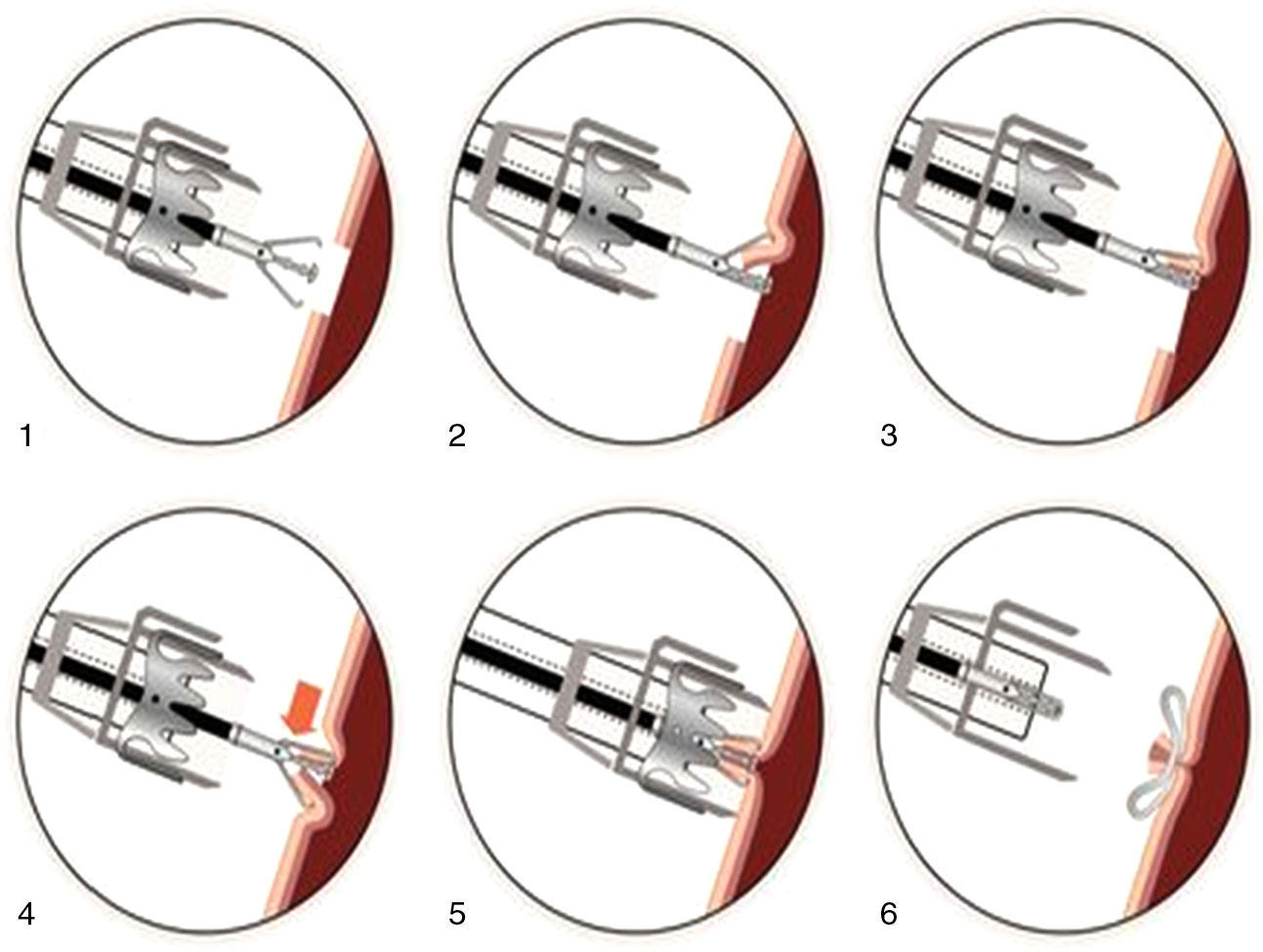
 or bear claw; it is assembled open at the end of the endoscope and, after its release, by a system similar to that used with elastic bands, it traps and seals the edges of the laceration in the digestive tube wall. Image reproduced with permission.")
The Ovesco clip, also called OTSC (over-the-scope clip) or bear claw; it is assembled open at the end of the endoscope and, after its release, by a system similar to that used with elastic bands, it traps and seals the edges of the laceration in the digestive tube wall. Image reproduced with permission.
After an evident iatrogenic perforation of the colon treated with an Ovesco® clip, there is dilemma about the need for subsequent exploratory laparoscopy or laparotomy due to the difficulty involved in the endoscopic evaluation of the laceration as well as correct clip placement and, furthermore, the possible leakage of a significant amount of contaminating material to the peritoneal cavity. Therefore, in certain situations that meet the factors for a good prognosis, including proper previous colonic preparation, perforation less than 2cm, lesions in the rectum (given its extraperitoneal location) and absence of alarming clinical data, conservative management could be indicated with clips, hospital observation and CT with oral and rectal contrast in order to rule out any leaks. In the presence of symptoms or signs that may indicate progressing complications, emergency surgery is the treatment of choice. In the case that we present, in hindsight we admit that conservative endoscopic treatment would have been sufficient and the surgical intervention could have been avoided, but the limited experience with the technique and the clinical evolution of the patient led us to decide otherwise.
Published experiences using Ovesco® clips are limited to case reports or retrospective studies of small series. Furthermore, the reports include not only perforations occurring during diagnostic colonoscopy, as in our case, but also haemorrhages, ulcer perforations, anastomotic fistulas and perforations after polypectomy.7,9 In any event, the results are promising and surgery can be avoided in most cases. In the series by Nishiyama, in 23 patients there were no complications with the use of Ovesco® clips, and the success rate was above 80%.7 In a recent review of 79 patients in whom this procedure was used, 22 cases were perforations and in 21 the results were satisfactory.10
Please cite this article as: Pérez-Cuadrado-Robles E, Flores-Pastor B, Bebia P, Pérez-Cuadrado-Martínez E, Aguayo-Albasini JL. Manejo endoscópico mediante sobreclip ovesco de una perforación colonoscópica durante procedimiento un dia. Cir Esp. 2016;94:e25–e27.
