





The aim of this study was to review original scientific articles describing the relationship between atmospheric pollution and damage to human health. We also aimed to determine which of these studies mentioned public policy issues.
Original articles relating to atmospheric pollution and human health published between 1995 and 2009 were retrieved from the PubMed database and analyzed. This study included only articles dealing with atmospheric pollutants resulting primarily from vehicle emissions. Three researchers were involved in the final selection of the studies, and the chosen articles were approved by at least two of the three researchers.
Of the 84 non-Brazilian studies analyzed, 80 showed an association between atmospheric pollution and adverse effects on human health. Moreover, 66 showed evidence of adverse effects on human health, even at levels below the permitted emission standards. Three studies mentioned public policies aimed at changing emission standards. Similarly, the 29 selected Brazilian studies reported adverse associations with human health, and 27 showed evidence of adverse effects even at levels below the legally permitted emission standards. Of these studies, 16 mentioned public policies aimed at changing emission standards.
Based on the Brazilian and non-Brazilian scientific studies that have been conducted, it can be concluded that, even under conditions that are compliant with Brazilian air quality standards, the concentration of atmospheric pollutants in Brazil can negatively affect human health. However, as little discussion of this topic has been generated, this finding demonstrates the need to incorporate epidemiological evidence into decisions regarding legal regulations and to discuss the public policy implications in epidemiological studies.
Motor vehicle emissions have been increasing over time, and more efficient measures are required for their effective reduction. Among the anthropogenic sources of emissions, the present work focuses on pollution from mobile sources, primarily motor vehicles.
It is predicted that vehicle emissions in 2030 will be worse than they are now. The harmful effects of vehicle pollutants (hydrocarbons, nitrogen oxide, carbon monoxide and particulates) on human health and the environment have been scientifically proven, and the body of evidence detailing these effects continues to grow.1
Solid or suspended liquid particles, such as those present in aerosol sprays, are classified according to their aerodynamic properties (which are the determinants of particle transportation, penetration and deposition in the respiratory airway) as follows: coarse (2.5 to 10 μm aerodynamic diameter), fine (less than 2.5 μm in diameter) and ultrafine (less than 0.1 μm in diameter).11
In large urban centers, people die from causes related to air pollution each year. In addition to causing deaths, air pollution is also the cause of a number of immediate, medium-term and long-term human health problems.11
Fine particles can reach the alveoli and enter the blood stream, and heart and lung disease,100 diabetes,102 premature birth,35 low birth weight,34 cancer,28 sudden death37 and cognitive alterations41 are some of the comorbidities that have been associated with the effects of or damage caused by air pollution in large urban centers.2
According to Damasceno-Rodrigues et al. (2009), the mechanisms by which air pollution negatively influences these comorbidities are not well understood. Possible mechanisms, such as increased calcium influx upon contact with macrophages, upregulation of proinflammatory mediators, increased blood viscosity, increased fibrinogen and C-reactive protein levels and alterations in blood rheology favoring coagulation, have been suggested. The oxidative stress generated by air pollution has also been proposed as a major mechanism of tissue injury leading to pulmonary and systemic inflammation.124
The World Health Organization (WHO) recommends PM2.5 (particulate matter less than 2.5 μm in diameter) rather than PM10 (particulate matter less than 10 μm in diameter) as an indicator of risk to human health.4 In 1997, the American Environmental Agency (US EPA) established the initial parameters for PM2.5.
Several episodes of excessive pollution have been correlated with increased numbers of deaths in some cities in Europe and the United States.5,6. The Clean Air Act of 1956 and 1968 expanded the oversight of polluting emissions. In 1976 in Europe, the Commission of the European Communities (CEC) established standards for air quality, which were further revised and used as the basis for European legislation.7 In the 1950s, California implemented pioneering legal regulations controlling vehicle emissions. In 2005, the WHO also established standard values for this parameter.
In the 1970s and 1980s, increases in vehicle production led to a larger number of vehicles being used worldwide, a trend that was most noticeable in large urban centers. In Brazil, Resolution 03/1990 from the Environmental National Council (CONAMA), which used data from CONAMA Resolution 05/1989, established standards for air quality consisting of “the concentrations of pollution that, when exceeded, could affect the health, safety and wellbeing of the population, as well as causing damage to flora, fauna and the environment in general....” The resolution described atmospheric pollution as “any form of matter or energy with sufficient quantity, concentration, exposure or characteristics beyond the established levels that could cause the air to be the following: I- inadequate, harmful or damaging to health; II- inappropriate for public wellbeing; III- damaging to materials, fauna and flora; and IV- damaging to the safety, use and enjoyment of property and to the normal activities of the community.”8
In 1998, increased emissions of pollutants in São Paulo led to the implementation of the Program for Control of Air Pollution by Motor Vehicles, PROCONVE (originally created in 1986). This program declared that new vehicles should conform to the maximum emission limits under standard tests using a reference fuel. It also required certification for prototypes and production line vehicles, a special license from the federal environmental authority for the use of alternative fuels, withdrawal and repair of vehicles that did not conform to the production or project specifications and prohibition of the sales of non-homologated vehicles. This program led to the removal of lead from gas in 1989, set 22% as the proportion of anhydrous alcohol to be added to gas across the entire country in 1993 and gradually reduced the sulfur content in diesel fuel used inside cities.9
However, vehicle emissions are still the main source of atmospheric pollution, and the Brazilian standards have not changed since the 1990s, when the CONAMA Resolution was published as Resolution 03/1990. A number of studies have shown a clear association between atmospheric pollution and negative effects on human health, thus demonstrating the concern of the scientific community on this topic. However, despite the weight of scientific evidence, air quality standards in Brazil have remained the same over the last 20 years, indicating a significant imbalance between the science and public policy.
Seeking a balance between individual rights (the exposure of each citizen to pollutants) and collective rights (those of society as a whole), the present study aimed to review original Brazilian and non-Brazilian studies carried out between 1995 and 2009. By means of a systematic review, the cause-effect relationship between pollution from motor vehicles and adverse events on human health was examined, both for pollution levels at legally permitted standards and those below the standards. Additionally, this review was conducted to identify whether these studies dealt with aspects of public policy involving measures to mitigate the adverse effects of pollution on human health. This outcome would suggest an interplay between the science and the adoption of public policies, thus expressing intersectoral attempts to protect our greatest asset, human health.
Consequently, the hypothesis investigated in this review is that the interface between law and epidemiology is necessary for and capable of protecting human health from the effects of pollution. From this starting point, our work aimed to assist decision makers in discussing more restrictive proposals for air quality standards, following international trends. Furthermore, the present study not only reviewed data from epidemiological studies but also investigated which studies specifically assessed the data with respect to concerns for developing efficient public policy.
METHODSPubMed was used for this review because it includes over 19 million papers from health-related fields that were published in over 3,800 scientific journals. Furthermore, papers in the PubMed database include studies from other primary sources, such as Medline, meaning that PubMed includes a large number of both Brazilian and non-Brazilian reports published in internationally renowned scientific journals. PubMed was developed by the National Center for Biotechnology Information, and it is maintained by the National Library of Medicine.
The following terms were used for searching the PubMed database:
- •
air pollution, health, Brazil, epidemiologic;
- •
air pollution, health, Brazil;
- •
air pollution, health, Brazil, epidemiologic study;
- •
air pollution, health, epidemiologic cohort;
- •
air pollution, health, epidemiologic case control;
- •
air pollution, health, epidemiologic time series study;
- •
traffic, air pollution, epidemiologic panel;
- •
traffic, air pollution, epidemiologic review.
Original studies were initially selected for our analysis after excluding those in which the objectives did not include vehicle atmospheric pollution (for example, papers on pollution due to sugar cane burning or papers regarding internal pollutants).
At the next stage, three researchers were invited to choose epidemiological studies using their own judgment, based on experience, with the aim of addressing the study hypothesis presented above. The researchers separately made decisions regarding the inclusion of the studies to avoid bias in the inclusion criteria. The researchers were epidemiologists and experts on atmospheric pollution, and the studies were selected based on their epidemiological quality. Each of the reviewers received a file containing full reprints of the epidemiological studies, as well as a list of all study titles divided according to study type. After making their selections through an analysis of the basis and methodological quality of the studies, the researchers returned the file and titles.
The studies selected were those that received at least two votes for inclusion in the systematic review and that referred to outdoor air pollution, particularly the ones related to atmospheric emission of pollutants from motor vehicles. Only national and international studies related to air pollution in peer-reviewed journals, epidemiological studies, original articles and studies examining automotive sources of outdoor pollution with well-explained statistical positive or negative associations were included.
The final selection was made by the study supervisor, who reviewed all of the articles according to the inclusion criteria.
Two tables containing the following data were prepared: type of study, study design, outcome, study population, statistical analysis applied, pollutants investigated, estimates, covariables and whether the effects on health were assessed, including cases where the levels were below the legally permitted standards. One table included Brazilian papers, whereas the other included non-Brazilian studies.
The data from these initial tables were used to produce two additional tables that are presented in this paper. These tables include only the type of study, study population, outcome, association, discussion of public policies for decreasing pollution levels, effects on health if emissions remain below the Brazilian standards and the appropriate citation(s) for each study.
The scientific papers selected for this work were original, but any review articles and systematic review papers found were used for data comparison and discussion.
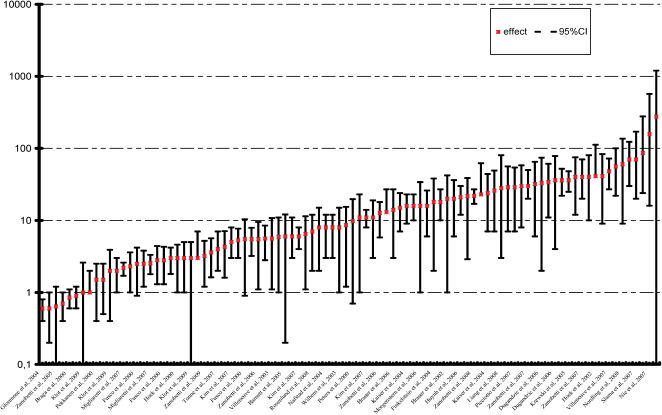
In addition, two figures showing the percentage increase in pollution, including cases where it was below the limits imposed by air quality standards, were designed. These figures present the percentage increases and their confidence intervals.
RESULTSInitially, 2,530 Brazilian and non-Brazilian articles were collected, and after preliminary selection, 249 articles exclusively referring to outdoor pollution were chosen.
After the subsequent analysis conducted by the three researchers participating in the study group, 143 reports were finally selected according the inclusion criteria described in the Methods section.
Only 113 of these articles were used in our final analysis because reviews and systematic reviews were excluded. Figure 1 shows the selection steps in the review process.

The non-Brazilian studies selected included 1 clinical trial, 9 case crossover studies, 13 case-control studies, 15 time series, 28 cohorts, 10 panels, 22 reviews, 6 systematic reviews and 8 cross-sectional studies. Therefore, a total of 112 non-Brazilian studies were included. Excluding reviews and systematic reviews, 84 non-Brazilian studies remained for our final analysis (Table 1).
Non-Brazilian studies of air pollution, categorized by type of study, study population, outcomes and effects found.
| Type of study (n) | Study population (n) | Outcome (n) | Association (n) | Effect below the Brazilian limit (n) | Discussion on public policies for decreasing emissions | References |
|---|---|---|---|---|---|---|
| Clinical trial (1) | Adults (1) | Atherosclerosis | Yes | Yes (1) | No (1) | 16 |
| Case crossover (9) | Adults (5) Children (1) | Respiratory diseases (4) | Yes (8) | Yes (8) | No (9) | 17 - 25 |
| Elderly (2) | Cardiovascular diseases (5) | No (1) | No (1) | |||
| All (1) | ||||||
| Case control (13) | Adult (5) | Respiratory diseases (4) | Yes (11) | Yes (7) | No (13) | 26 - 38 |
| Children (7) | Pregnancy-related outcomes (3) | No (2) | No (6) | |||
| Elderly (1) | Cardiovascular diseases (3) | |||||
| Cancer (3) | ||||||
| Cohort (28) | Adults (12) | Respiratory diseases (8) | Yes (28) | Yes (22) | No (28) | 39 - 66 |
| Children (13) | Mortality (3) | No (6) | ||||
| Elderly (3) | Pregnancy-related outcomes (3) | |||||
| Cognitive deficit (1) | ||||||
| Cancer (1) | ||||||
| Otitis (1) | ||||||
| Cardiovascular diseases (11) | ||||||
| Panel (10) | Adults (5) | Respiratory diseases (5) | Yes (9) | Yes (9) | Yes (2) | 67 - 76 |
| Children (3) | Cardiovascular diseases (5) | No(1) | No (1) | No (8) | ||
| Elderly (2) | ||||||
| Time series (15) | Adults (13) | Respiratory diseases (1) | Yes (15) | Yes (15) | Yes (1) | 77 - 91 |
| Elderly (1) | Cardiovascular diseases (3) | No (14) | ||||
| All (1) | Mortality (11) | |||||
| Cross-sectional (8) | Adults (5) | Respiratory diseases (6) | Yes (8) | Yes (4) | No (8) | 92 - 99 |
| Children (2) | Cardiovascular diseases (1) | No (4) | ||||
| Elderly (1) | Diabetes (1) |
n = quantity.
The Brazilian studies selected included 1 case control, 2 panels, 2 reviews, 20 time series and 6 cross-sectional studies. Therefore, a total of 31 Brazilian studies were included, and excluding reviews and systematic reviews, 29 Brazilian studies remained for our final analysis (Table 2).
Brazilian studies of air pollution, categorized by type of study, study population, outcomes and effects found.
| Type of study (n) | Study population (n) | Outcome (n) | Association (n) | Effects below the Brazilian limit (n) | Discussion on public policies for decreasing emissions | References |
|---|---|---|---|---|---|---|
| Case control (1) | Children (1) | Perinatal death | Yes | Not informed | Not informed | 100 |
| Panel (2) | Adults (1) | Blood pressure; carboxyhemoglobin | Yes for both | Yes (2) | Yes (1) | 101 – 102 |
| Children (1) | No (1) | |||||
| Time series (20) | Adults (7) | Respiratory diseases (14); | Yes (19) | Yes (18) | Yes (12) | 103 - 123 |
| Children (11) | Pregnancy-related outcomes (2); | No (1) | No (2) | No (8) | ||
| Elderly (2) | Cardiovascular diseases (4) | |||||
| Cross-sectional (6) | Children (5) | Respiratory diseases (4) | Yes (5) | Yes (6) | Yes (3) | 124 - 129 |
| All (1) | Child mortality (1) | No (1) | No (3) | |||
| Pregnancy-related outcomes (1) |
n = quantity.
Of the 84 non-Brazilian studies selected for our analysis (excluding reviews and systematic reviews), 66 demonstrated effects on health, even when emissions were below the permitted levels (these studies are marked “yes” in the corresponding column in Table 1). These 66 non-Brazilian studies demonstrated that, even when emissions of atmospheric pollutants were below the levels permitted by Brazilian legislation, they were capable of negatively affecting the health of the urban population.
Among the 30 Brazilian studies selected for the present work (excluding reviews), 27 showed that there were risks to health, even if the population was exposed to pollution levels below those permitted by Brazilian legislation.
The reviewed studies showed that some age groups, particularly the elderly and children, are more susceptible to air pollution emissions. Some diseases were frequently associated with exposure to air pollution; for example, respiratory and cardiovascular outcomes were described in several studies (Tables 1 and 2).
Only 3 of the non-Brazilian studies and 16 of the Brazilian studies specifically mentioned public policy.
Finally, Figures 2 and 3 show the percentage increase of some of the endpoints of the selected studies and their relative risks.
 from selected non- Brazilian studies of air pollution and adverse human health outcomes.")
 from Brazilian studies of air pollution and adverse human health outcomes.")
Although the papers selected for review in this study have associated atmospheric pollutants with damage to human health, including comorbidities such as respiratory diseases, cardiovascular diseases, pregnancy outcomes, cancer and death, most of these papers failed to mention public policy. Therefore, while science is making great strides in demonstrating the harmful effects of atmospheric pollution on human health, public authorities are not using these data to make decisions concerning the reduction of emissions or the adoption of measures that might indirectly affect the comfort of the population and, therefore, might not be politically acceptable. Nonetheless, such measures should be adopted, together with an awareness campaign, so that a change of habits and attitudes occurs in everyday lives.
Epidemiological evidence produced using several different study models has demonstrated that atmospheric pollution negatively affects human health, even if the pollutants are below the levels established by Brazilian legislation (CONAMA National Council of the Environment Resolution 03/1990). However, despite the available scientific evidence, there has still not been any appropriate reaction in terms of the adoption of public policies in Brazil that are aimed at improving the air quality of large urban centers.
Measures such as vehicle inspections, efficient public transport, traffic management, bus lanes, bicycle lane systems and urban tolls are all consistent with proposals for creating a healthy environment. However, the use of cleaner fuel must also be pursued because sustained sulfur emissions will lead to more deaths and hospitalizations.
Studies carried out at the University of São Paulo have confirmed that living in a city with polluted air leads to a 75% increase in the risk of a heart attack compared to living in a city with clean air. Additionally, the possibility of dying in a traffic jam is two and a half times greater in a polluted city. For every 10 μg/m3 of PM10 removed from the air, there is an increase in life expectancy of eight to twelve months. If an economic model was applied to Brazilian public health, and the well-being of the population and quality of life were considered, it would reveal how much Brazil is losing, even though a few companies and decision makers may still be turning profits.
According to Dockery and Pope, 10 the establishment of emission standards implies the existence of a limit below which there would be no harm to health. However, in reality, the response is linear, and there is no safe lower limit of these pollutants in terms of human health.
Despite ample scientific evidence, no strong concern has been shown for human health and its sensitivity to pollution. In Brazil, we have been using outdated standards that do not follow the international trend. Moreover, we have adopted policies that encourage the purchase of vehicles and, thus, are inadequate to solve transportation problems. At the same time, the use of diesel fuel, which causes less pollution, has been postponed. In conclusion, Brazil needs to change its emission standards and adopt policies that address the awareness, expansion and improvement of public transportation.
The present review highlights the inappropriate nature of decisions made by public institutions regarding the establishment of public policies related to pollution, which are dissociated from the reality demonstrated by scientific evidence. Therefore, the authors of this report seek to draw the attention of Brazilian decision makers toward implementing changes in the public and political measures adopted on this topic. Epidemiological studies need to be understood and used as the basis for defining these public policies with the aim of improving the quality of life among the target population. Education, awareness and concern are allies in the adoption of appropriate public policies.
Of the 113 Brazilian and non-Brazilian articles that were analyzed in the present review, only 4 papers did not find an association between pollution and health. This suggests that there may be a publication bias. Such a bias would consist of a tendency for researchers, reviewers and editors to only submit or accept papers that follow the direction of the hypothesis that they wish to prove. It is important and necessary to avoid publication biases, both from the point of view of the universal nature of scientific knowledge and of meta-analysis studies. Decisions regarding treatments, medications placed on the market and many medical situations and public health decisions are based on research.14 However, there is strong evidence supporting the association between atmospheric pollution by vehicles and adverse effects on human health.
The tables presenting the summarized data from the papers selected not only show the cause-effect relationship between atmospheric pollution and harm to human health but also indicate which of the selected studies effectively led to attitudes being adopted in terms of public policy. From the perspective of proposals for public policy, there is a gap between the science and the policy makers because even the studies that mention public policy do not actually suggest proposals for reducing atmospheric pollution.
By bringing together studies from several parts of the world, including Brazil, it can be seen that their results trend in the same direction. The studies were able to answer the essential questions proposed in the present study, namely:
Is there any epidemiological evidence for adverse effects of atmospheric pollution on human health? Do these effects occur even at concentrations that are lower than the maximum permitted levels? Was there any concern in these reports about outlining public policy measures that would restrict emissions?
The present work produced clear answers to these questions. There is epidemiological evidence for the negative effects of atmospheric pollution on human health, and these effects can be observed even after exposure to emission levels that are below the established legal levels in Brazil. The most-affected population comprises so-called susceptible individuals (children, the elderly and individuals with heart disease or asthma). Few reports specifically mentioned public health policy, but it seems that mentioning such policies is more frequent in Brazilian studies than in non-Brazilian ones.
The Brazilian model for individual transportation is failing, and there is a need to prioritize and modernize the public transportation system. Even if public health were not an issue, the time wasted in traffic jams should be a motivating factor for adopting new public policies and changing the habits of the population. Thus, the immobilization of urban centers will force decision makers and people living in the city to become aware of these issues.
The adoption of more efficient public policies is essential for the reduction of current emission standards for air pollutants. These measures cannot continue to accommodate an increasing number of vehicles. Instead, epidemiology should be seen as a science advocating the adoption of stricter standards for air emissions as well as education of the population involved, thereby giving legitimacy to its decisions. Thus, policies on education, awareness and mandatory investments in the automotive sector and in public transportation are of paramount importance to accomplish this goal. Internationally, priority is given to scientific information and to active public participation, not only as consumers but also as an essential part of the quality of life, both present and future. Such participation requires the adoption of integrated measures based on the population and the government.
Therefore, we hope that this work can serve as the basis for a dynamic and responsible decision-making process. We also hope that it can be used to establish public policies that are not only theoretically ideal but also equally efficient regarding human health.
CONCLUSIONThis review made it possible to extrapolate conclusions from the individual and independent results of each study analyzed, identifying coherent data that can be used for developing public guidelines and for future planning. The present study used scientific data based on epidemiological studies that were produced both within the Brazilian sphere and in other countries. It showed that, even when atmospheric pollutants are within legally established limits, they can be harmful to health. This harm leads to additional expenses for public health services and, ultimately, for the government, which is responsible for ensuring the quality of life of the population and assuring the right to healthcare.
The concept of co-benefits of pollution control is becoming increasingly relevant and is taking on the role of a guiding principle because there must be synergy between the measures aimed at the mitigation of emissions and those aimed at improving public health. These concepts are constantly interlinking the fields of healthcare and law and can lead to public policies based upon scientifically verified results. Such policies always aim toward a better quality of life and increased well-being of the population.
The aim of this study was not to explain the pathophysiology of the comorbidities caused by exposure to air pollutants. However, considering the harmful effects that have already been reported in epidemiological studies (such as those that were part of this systematic review, listed in Tables 1 and 2), we discussed the need for the application of these data by decision makers to allow for the proper adjustment of legislation in support of human health. Thus, epidemiological studies were used as a tool to demonstrate the objective of this paper, namely the need for an interrelationship between health and epidemiology in the shaping of Brazilian public policy.
Finally, we suggest an interface between science and Brazilian public policy involving intersectoral attempts to protect our most important asset, human health.
This study was supported by the Laboratory of Medical Investigations (LIM05-FMUSP) and FAPESP (Research Support Foundation of the State of São Paulo).
We are grateful to the LIM05-FMUSP (Laboratory for Medical Investigations of the University of São Paulo) for its unwavering support and to the Research Support Foundation of the State of São Paulo (FAPESP) for the study bursary that made this work possible.