




Cerebrotendinous xanthomatosis is a rare autosomal recessive hereditary disease that is caused by a mutation in the gene encoding the mitochondrial enzyme sterol 27-hydroxylase (CYP27). The CYP27 gene is located on chromosome 2q35-qter and is responsible for the conversion of cholesterol into cholic and chenodeoxycholic acid. Cerebrotendinous xanthomatosis results in increased levels of serum cholestanol, a cholesterol precursor, and increased deposition of cholestanol and cholesterol in various tissues, especially the lenses, tendons, and the central nervous system. The principal manifestations of Cerebrotendinous xanthomatosis include juvenile cataracts, tendon xanthomas, and progressive neurological symptoms.1
Early recognition of this condition is essential because cholic and chenodeoxycholic acid replacement therapy can prevent Cerebrotendinous xanthomatosis -induced brain damage, which leads to severe neurological dysfunction and death. We present the case of a patient with clinical, radiological, and biochemical evidence of Cerebrotendinous xanthomatosis and his response to cholic and chenodeoxycholic acid treatment.
CASE REPORTThis report describes a 30-year-old male who displayed normal psychomotor development until 10 years of age when, according to his mother, he began presenting learning difficulties and showed progressive cognitive decline. At 15 years of age, the patient presented progressive gait instability and enlargement of the Achilles tendons. At age 17, he suffered his first convulsive episode. The patient has suffered a total of four seizures since that time, and his seizure condition is adequately controlled with the use of anticonvulsants. A family history revealed that the patient's parents were cousins. Physical examination revealed bilateral Achilles tendon enlargement and bilateral cataracts. A neurological examination identified spastic paraparesis, brisk deep tendon reflexes and extensor plantar responses, upper limb symmetrical dysmetria and dysdiadochokinesia, and ataxic-paraparetic gait. The remainder of the patient's physical examination was normal.
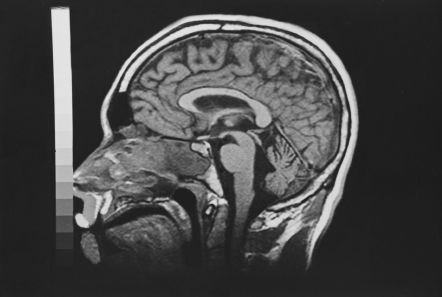
Magnetic resonance imaging (MRI) of the patient's skull revealed mild cerebellar atrophy (Figure 1). MRI of the left ankle showed fusiform thickening of the Achilles tendon with heterogeneous signals on all sequences, T2-hyperintense foci due to the presence of fat, and a slight increase in the uptake of paramagnetic contrast. These results were suggestive of a xanthoma of the Achilles tendon (Figure 2). Laboratory tests (complete blood count, biochemistry, liver and kidney function, lipid panel, and coagulation tests) were normal. The patient's serum cholestanol level was high (28.3 µg/mL, normal value <6 µg/mL).


Based on these findings, the patient was diagnosed with CTX, and treatment with CDCA (750 mg/day) was immediately initiated. The drug was imported from Germany. A significant improvement in neurological symptoms was observed after one year of follow-up, especially with respect to ataxia and coordination. The patient retains a slightly ataxic gait but presents normal finger-to-nose and fast finger movements, and his serum cholestanol level has been reduced to 4.1 µg/mL. In addition, the patient has undergone eye surgery to treat his cataracts. The patient authorized the publication of this case report by signing a consent form.
DISCUSSIONVan Bogaert et al. described the first CTX phenotype in 1937.2 Subsequent work established several additional symptoms of CTX, including cholestanol accumulation in several tissues and the absence of CDCA in the bile. These symptoms were determined to be the result of a disorder of hepatic conversion of cholesterol to cholic acid and CDCA.3 In 1975, Salen et al. reported that administration of CDCA dramatically reduced cholestanol synthesis in CTX patients.4 In 1984, Berginer et al. demonstrated that one year of CDCA oral supplementation treatment at 750 mg/day was sufficient to produce a significant improvement in neurological symptoms, normalization of EEG readings, and a reduction in serum cholestanol in CTX patients.5 In 1991, Cali et al. identified a defect in the gene encoding the 27-hydroxylase enzyme in CTX patients.6 More than fifty different mutations of this gene have since been reported worldwide, and molecular analysis has enabled diagnosis during the pre-symptomatic period.7
The unexplained presence of bilateral cataracts and chronic diarrhea in children suggests a diagnosis of CTX. Tendon xanthomas usually appear in the second or third decade of life, especially in the Achilles tendons. Neurological symptoms usually begin in the second decade of life and include ataxia, pyramidal and extrapyramidal signs, peripheral sensory-motor neuropathy, epilepsy, and dementia.7,8 Psychiatric manifestations such as depression, suicidal thoughts, catatonia, and psychotic symptoms may also present with CTX and usually appear at early stages.9 Other clinical manifestations include osteoporosis, bone fractures, premature arteriosclerosis, and coronary and lung disease.1,8
The mechanism underlying the progressive neurological dysfunction in CTX remains unknown. Some authors support the hypothesis that increased concentrations of apolipoprotein B in the cerebrospinal fluid (CSF) of CTX patients facilitates cholestanol and cholesterol transport across the blood-brain barrier. Presumably, this accumulation of cholestanol activates apoptotic pathways, resulting in neuronal death. However, CDCA treatment restores the selective permeability of the blood-brain barrier, normalizing the concentration of sterols and lipoproteins in the CSF and promoting reversal of the neurological symptoms.1,10
In a recent study, Berginer et al. demonstrated that early diagnosis and initiation of CDCA treatment during the pre-clinical and initial phases of CTX may prevent the development of clinical manifestations of CTX. These authors suggest that the following three steps are fundamental to prevent irreversible damage in patients with CTX: 1) recognition of early symptoms, including chronic diarrhea and juvenile cataracts, by pediatricians, 2) confirmation of the diagnosis through biochemical and genetic analysis, and 3) immediate CDCA treatment to prevent the CTX phenotype.7
This report describes the case of a patient with clinical, biochemical, and radiological characteristics indicative of CTX. In support of this diagnosis, biochemical analysis demonstrated elevated cholestanol levels. Tendon xanthomas can occur in other lipidoses, such as familial hypercholesterolemia and sitosterolemia, but juvenile cataracts and progressive neurological symptoms are only seen in CTX.1 We were unable to perform molecular genetic analysis in our patient, but MRI analysis of the skull revealed cerebellar atrophy. A similar finding has been reported by other authors, as have bilateral and symmetric hyperintense lesions surrounding the white matter of the dentate nuclei, cerebral atrophy, and demyelinating lesions.11 These changes were not demonstrated in our case due to technological limitations. CDCA treatment was immediately initiated in our patient, and a significant improvement in neurological symptoms was observed after one year of treatment. Furthermore, the clinical improvement correlated with a reduction in cholestanol serum levels. Unfortunately, because treatment was initiated at a late stage in this case, it did not result in a functional cure of CTX. However, the treatment did promote a significant improvement in quality of life and, more importantly, prevented progression of the disease.