




Cheyne-Stokes respiration is a form of periodic breathing in which central apneas and hypopneas alternate with periods of hyperventilation, producing a waxing and waning pattern of tidal volume. This review focuses on the causes and consequences of Cheyne-Stokes respiration in patients with congestive heart failure, in whom the prevalence is strikingly high and ranges from 30% to 50%. Several factors have been implicated in the genesis of Cheyne-Stokes respiration, including low cardiac output and recurrent hypoxia. The key pathophysiological mechanism triggering Cheyne-Stokes respiration is hyperventilation and low arterial CO2 (PaCO2) that when below the apneic threshold triggers a central apnea. Hyperventilation is associated with pulmonary congestion, and Cheyne-Stokes respiration is more prone to occur during sleep, when the respiratory system is mainly dependent on chemical control. It is associated with recurrent dips in oxygen saturation and arousals from sleep, with oscillations in blood pressure and heart rate, sympathetic activation and increased risk of ventricular tachycardia. Cheyne-Stokes respiration is an independent marker of poor prognosis and may participate in a vicious cycle, further stressing the failing heart.
A respiração de Cheyne-Stokes é uma forma de respiração periódica na qual apnéias e hipopnéias se alternam com períodos de hiperpnéias que apresentam um padrão crescendo e decrescendo de volume corrente. Esta revisão enfoca as causa e conseqüências da respiração de Cheyne-Stokes em pacientes com insuficiência cardíaca congestiva na qual a prevalência é extremamente alta e varia entre 30 a 50%. Vários fatores foram implicados na gênese da respiração de Cheyne-Stokes, incluindo baixo debito cardíaco e hipoxia recorrente. Hiperventilacão e baixos níveis de CO2 arterial (PaCO2), que quando abaixo do limiar de apnéia desencadeiam apnéia central são os mecanismos fisiopatológicos chave na gênese da respiração de Cheyne-Stokes. Hiperventilação está associada com congestão pulmonar, e a respiração de Cheyne-Stokes tem uma tendência maior de ocorrer durante o sono, quando o centro respiratório é dependente principalmente do controle químico. A respiração de Cheyne-Stokes está associada a quedas recorrentes da saturação de oxigênio e ao despertar do sono, com oscilações recorrentes na freqüência cardíaca, pressão arterial, aumento da atividade simpática e risco aumentado de taquicardia ventricular. A respiração de Cheyne-Stokes é um marcador independente de mau prognostico e provavelmente participa de um ciclo vicioso que contribui para a deterioração cardíaca.
Clinicians generally pay little attention to a patient's pattern of breathing.1 This is partly the result of the limitations of physical examination, which is notoriously unreliable in assessing changes in tidal volume.2 Therefore, detection of abnormal patterns requires either an unusually practiced eye or, preferably, an objective method of recording the breathing pattern. Moreover, subtle alterations in the breathing pattern may manifest themselves only during exercise3 or sleep.4 Cheyne-Stokes respiration (CSR) is the best-known disturbance of the breathing pattern.1 The periodic irregularity of respiration, characterized by a period of apnea followed by breathing that begins almost imperceptibly, waxes until it becomes dyspneic then wanes until apnea follows the last shallow breath, was first described by Cheyne, in 1818.5 This particular pattern of breathing was later recognized as a complication associated with heart failure by Stokes, in 1854.6 The patient in the original description suffered from both congestive heart failure (CHF) and neurologic disease.5 Therefore, the term Cheyne-Stokes respiration has been used to describe this abnormal pattern of breathing but not to denote any specific underlying etiology. It is also not clear from the original descriptions whether the apneas were central or obstructive in nature (ie, absence or presence of respiratory effort during apnea, respectively). Patients with CHF may present both central and obstructive sleep apnea,7–15 may convert obstructive to central sleep apnea during a single night,16 and may present obstructive apneas with a prolonged ventilatory pattern that mimics Cheyne-Stokes respiration.17 In this text for the sake of simplicity, unless otherwise stated, Cheyne-Stokes respiration will imply that it is associated with central apnea (Fig. 1).
. Observe the typical crescendo-decrescendo tidal volume interposed with central apneas")
Polysomnographic recordings of a congestive heart failure presenting Cheyne-Stokes respiration during sleep. The top channels are related to sleep recordings. The bottom channels trac respiration by monitoring motion of the thorax, abdomen and respiratory flow (nasal canula). Observe the typical crescendo-decrescendo tidal volume interposed with central apneas
Cheyne-Stokes respiration has for too long been considered as a physiologic curiosity and not a clinical problem worthy of diagnosis and specific therapy,4,7 and only in the last few years has it attracted more clinical attention, since it has been recognized to be very common among patients with severe but stable CHF, and it can cause symptoms of a sleep apnea syndrome.4,7–13 In patients with severe but stable CHF, Cheyne-Stokes respiration is present in 30% to 50% of the patients.13,14 It is present in CHF of all origins, including Chagas disease.14,15 There is increasing evidence to suggest that Cheyne-Stokes respiration in patients with CHF participates a vicious cycle that further stresses the failing heart. In line with this hypothesis, we have shown that periodic oscillations of ventilation in normal subjects promoted profound oscillations in blood pressure and heart rate;18 similar cardiovascular effects were present in CHF patients during Cheyne-Stokes respiration19; and periodic ventricular premature beats were found to be higher during periods of this respiration than during periods of regular breathing in CHF patients.20 We have also recently reported that a mild form of Cheyne-Stokes respiration, characterized by periodic and cyclic oscillations of minute ventilation (also known as periodic breathing) was present in 30% of a population of CHF patients evaluated for heart transplant and was a powerful predictor of mortality.3 These findings may help to explain the increased mortality observed in CHF patients presenting Cheyne-Stokes respiration observed in some studies.21–23 This review will focus on the causes and consequences of Cheyne-Stokes respiration in patients with CHF. We will also briefly review concepts concerning the control of breathing. More extensive reviews on this topic have been recently published.4,24–27
CONTROL OF BREATHINGThe respiratory and the cardiovascular systems act in concert to transfer oxygen (O2) and carbon dioxide (CO2) between the atmosphere and the cells. Their control systems must be integrated to ensure that the metabolic needs of the tissues are met under varying conditions according to demands.28 Under normal conditions, ventilation is stable and maintains arterial blood gas tensions within narrow limits through a negative feedback circuit. This negative feedback system consists of a central controller sensitive to fluctuations in PaO2 and PaCO2 at the peripheral and central chemoreceptors and a mechanism (the lungs, chest wall, and respiratory muscles) that generates ventilation.29,30 The controlled variables are PaO2, PaCO2, and pH, which act as negative feedback signals to the central controller. In turn, the central controller maintains blood gas homeostasis by altering its neural output to the respiratory muscles in order to move the chest wall to achieve the appropriate level of ventilation. PaO2 and PaCO2 are altered accordingly. The system is stable, and the responses are linear over a wide range of PaCO2. However, apnea may prevail when the PaCO2 is driven below the apneic threshold.29 On the other hand, blood gas homeostasis is maintained through certain stabilizing influences inherent in the system. These include the maintenance of PaCO2 well above the threshold for apnea, a relatively low gain of the chemoreceptors, a short delay in the transmission of the effects of ventilation on PaO2 and PaCO2 to the chemoreceptors, the rapid correction of deviations in blood gas tensions toward the desired level, and a high functional residual capacity acting as a large reservoir of O2 and CO2 within the body to damp oscillations in PaO2 and PaCO2 during apneas.24,25,29,30
During sleep, the respiratory system is particularly prone to instability. As one passes from wakefulness to nonrapid eye movement (NREM) sleep, the waking neural drive to breathe is abolished, and the behavioral control system becomes quiescent. Therefore, the nonchemical drive to breathe associated with wakefulness, which tends to maintain ventilation even when PaCO2 is driven below the apnea threshold, is lost during sleep and breathing becomes critically dependent on the metabolic control system.29–32 In addition, during NREM sleep the threshold for a ventilatory response to CO2 is increased, so that a higher PaCO2 is necessary to stimulate breathing as compared to the awake state.28,29 If the PaCO2 during wakefulness is below this new threshold level during sleep, there will be a loss of respiratory drive resulting in a central apnea in the transition awake-sleep. During apnea, PaCO2 rises (at a rate proportional to metabolic CO2 production) until it reaches the critical threshold value, and breathing resumes. If sleep becomes firmly established at this point, regular breathing follows.29 However, should the central nervous system state shift back momentarily to the awake state, as occurs during arousals from sleep, the increased PaCO2 level that was present during sleep now represents a state of relative hypercapnia for wakefulness. Accordingly, a period of hyperpnea follows, in accordance with the awake ventilatory response to CO2, resulting in the hyperpneic phase of periodic breathing. As long as the central nervous system state continues to fluctuate between wakefulness and sleep, waxing and waning of the waking neural drive results in alternating periods of hyperpnea and apnea until sleep becomes firmly established. Hence, transitions in sleep-wakefulness states are an ideal setting for the generation of respiratory instability and periodic breathing even in normal humans.33 Similarly, sleep-awake transitions may produce respiratory control instability by a different mechanism: upper airway instability. Sleep is associated with loss of muscle tone, rendering the upper airway prone to collapse. In patients with partial or complete airway collapse at sleep, a central neural output to the respiratory muscles will not be rapidly translated into airflow. As a consequence, ventilation may be not sufficient during periods of upper airway collapse and, a moment later, will overshoot during brief arousals (when upper airway patency is reestablished). This mechanism may also lead to fluctuations of PaCO2 above and below the apneic threshold.30
CAUSES OF CHEYNE-STOKES RESPIRATIONThe key pathophysiologic mechanism leading to Cheyne-Stokes respiration is a fluctuation of PaCO2 above and below the apneic threshold.4,7,24,25 In patients with CHF, a number of destabilizing factors contribute to fluctuation in PaCO2. First, a low PaCO2 close to apneic predisposes to the development of central apneas. Under this condition, a relatively small increase in ventilation would drive PaCO2 below threshold and trigger a central apnea.4,7,24,25,34 Naughton et al.35 and Hanly et al.36 have shown that CHF patients with Cheyne-Stokes respiration have lower PaCO2 both while awake and asleep than those without Cheyne-Stokes. In patients with CHF, an association between Cheyne-Stokes and low PaCO2 both during wakefulness and NREM sleep has been demonstrated in several reports.35–40 Naughton et al.35 found that CHF patients with Cheyne-Stokes respiration had lower PaCO2 during wakefulness and NREM sleep than patients without it, who had comparable age, LVEF, PaO2, and lung-to-chemoreceptor circulatory delay. All episodes of Cheyne-Stokes respiration starting during stage 2 sleep were almost always, precipitated by hyperventilation in association with arousals from sleep. Furthermore, during Cheyne-Stokes episodes in stage 2 sleep, PaCO2 fell on average by 1.5 mm Hg, which mirrored a 23% rise in minute ventilation.35
Patients with CHF and Cheyne-Stokes respiration have an unusual response to the sleeping state, in that their PaCO2 levels do not increase as they go from wakefulness to sleep,38,39 and as a consequence PaCO2, is closer to their apneic threshold during sleep.39 Lorenzi-Filho et al.40 were able to abolish Cheyne-Stokes in CHF patients by inhalation of small concentrations of CO2 delivered by a mask. Stabilization of breathing was achieved by a small (~2 mm Hg) but significant increase in transcutaneous PCO2. In contrast, supplemental oxygen was not able to raise transcutaneous PCO2 and had no significant impact on the frequency of Cheyne-Stokes.40 This study reveals the critical importance of small variations in PaCO2, which when it falls below the apneic threshold triggers central apneas and Cheyne-Stokes respiration. Arousals, through promotion of hyperventilation, appear to facilitate rather than to provoke periodic breathing directly.
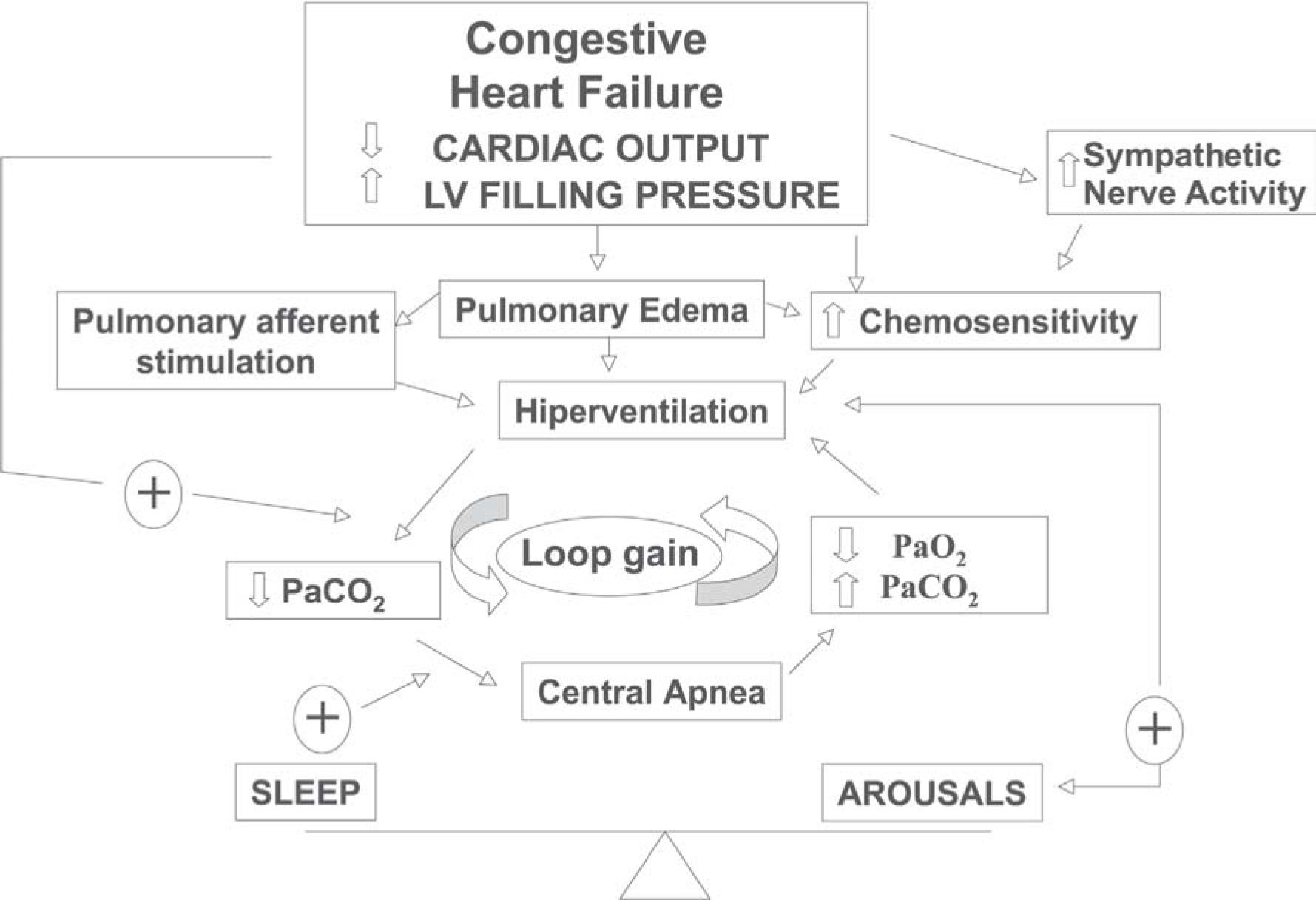
The second question is: why do patients with CHF hyperventilate? Several possible mechanisms, listed in Table 1 and summarized in Figure 2, may participate. The most important mechanisms will be discussed below.
Mechanisms responsible for respiratory stability (STABLE) and instability (UNSTABLE) in congestive heart failure patients
| Variable | VENTILATION STABLE | UNSTABLE |
|---|---|---|
| CHEMICAL FACTORS | ||
| PaCO2(apneic threshold) | Above | Close |
| Chemoreflex response | Rapid Adequate | Delayed Increased |
| O2 and CO2 reservoir | Large | Low Functional Residual Capacity |
| SLEEP FACTORS | ||
| Awake drive to breathe | Present | Absent during sleep |
| Continuity of sleep | Present | Arousals |

There is a considerable body of evidence showing that pulmonary congestion is associated with reduced PaCO2. Tkacova et al.38 examined a population of patients with CHF due to nonischemic dilated cardiomyopathy and showed that, in spite of similar left ventricular ejection fractions, the left ventricular (LV) end diastolic and systolic volumes were twice as high in patients with Cheyne-Stokes respiration as compared to those without it. In addition, Cheyne-Stokes patients had a significantly lower PaCO2 while awake, and a lower mean transcutaneous CO2 (PtcCO2) during stage 2 sleep. Furthermore, the greater the LV end-diastolic volume, the less the rise in PaCO2 from wakefulness to stage 2 sleep. This relationship suggests that marked LV dilatation in patients with nonischemic dilated cardiomyopathy is associated with a nonchemical respiratory drive that prevents the normal rise in PaCO2 during the transition from wakefulness to sleep. The most likely explanation for this relationship is that high LV volumes are associated with elevated LV filling pressures. These results are in line with the observation that pulmonary capillary wedge pressure was significantly greater in patients with CHF and Cheyne-Stokes respiration, as compared to CHF patients with no sleep apnea or obstructive sleep apnea.12 We have also studied CHF patients undergoing diagnostic cardiac catheterization, in which hemodynamic variables and arterial blood gases were measured simultaneously. PaCO2 correlated inversely with capillary wedge pressure (r = –0.80, P = .003). In addition, in 3 patients in whom multiple measurements were made, acute alterations in capillary wedge pressure caused inversely proportional changes in PaCO2.41 Therefore, hypocapnia in CHF patients is a respiratory manifestation of elevated LV filling pressures.
Pulmonary congestion stimulate ventilation and reduce PaCO2 by mechanisms that are not completely understood. Experiments in animals suggest that pulmonary venous congestion and elevation of interstitial pressure cause increased pulmonary vagal afferent nerve stimulation, which precipitates central apnea followed by rapid shallow ventilation with increased minute ventilation.42 These observations are limited, however, and Cheyne-Stokes was not studied. Congestive heart failure patients with Cheyne-Stokes respiration have high central and peripheral chemoresponsiviness.43,46,47 Elevated chemoreceptor responsiveness (gain) could destabilize the respiratory control system by increasing the tendency to hyperventilate, promoting both a background hypocapnia and also triggering a ventilatory overshoot. Augmented gain of the chemoreceptors, which could be primary or, more likely, secondary to pulmonary edema, destabilizes the respiratory control system by making it prone to ventilatory overshoot30,45 (Figure 2).
Prolonged circulatory timeProlonged circulation time leading to delays in transmitting changes of arterial blood gas tensions within the lungs to the chemoreceptors could theoretically destabilize the respiratory control system. It could do so by changing a negative feedback into a positive feedback system such that “the right response occurs at the wrong moment”.48,49 In support of this theory, Guyton et al.48 induced Cheyne-Stokes respiration in sedated dogs by inserting a length of tubing between the heart and brain to prolong the transit time from the lungs to the chemoreceptors. However, Cheyne-Stokes was achieved only when the circulatory delay was a few minutes in duration, far exceeding anything seen in patients with CHF. There is now a body of evidence indicating that prolonged circulatory delay is not the critical factor predisposing to Cheyne-Stokes respiration. In humans, the circulatory delay for a given chemical stimulus to reach the carotid body from the lungs can be estimated by determining the time from the end of an apnea until the maximum dip in SaO2 detected by an oximeter on the ear (which is in close proximity to the carotid body). This lung-to-ear circulation time (LECT) is inversely proportional to the stroke volume and cardiac output in both patients with normal and with abnormal heart function.50 In this study, patients with idiopathic central sleep apnea (ICSA), whose cardiac function and LECT were normal, were compared to CHF patients with Cheyne-Stokes. The results showed that despite having higher stroke volumes and shorter LECT than the CHF patients with Cheyne-Stokes, those with ICSA had the same low and fluctuating PaCO2 and similar high frequencies of central apnea during sleep. These data indicate that central apneas in patients with ICSA and Cheyne-Stokes are due to hypocapnia and fluctuations in PaCO2 below and above the apnea threshold, but are not related to the degree of circulatory delay. A number of investigators have also found no significant differences in LECT or LVEF between CHF patients with and without Cheyne-Stokes respiration-.21,22,35,36 In the same study, Hall et al. observed that the longer periodic breathing cycle length in the CHF patients with Cheyne-Stokes respiration was related to a longer LECT than in the patients with idiopathic central sleep apnea. The relationship between LECT and cycle length was found to be due to the correlation of LECT and hyperpnea length, whereas LECT did not correlate with apnea length. However, the characteristic “sculpting” and prolongation of the hyperpnea in CHF patients was related to their lower cardiac output. Therefore, rather than initiating periodic breathing and central apnea, circulatory delay appears to determine hyperpnea length and, secondarily, cycle length once periodic breathing with central apnea has been established. However, it does not affect apnea length, which is influenced by the degree of preceding hyperventilation and hypocapnia.51
HypoxiaOne possible explanation for hyperventilation and low PaCO2 is hypoxia. Normal subjects may present periodic breathing during sleep at high altitude. In periodic breathing at high altitude, hypoxemia causes hyperventilation and lowers PaCO2 below the apnea threshold.52 Under these conditions, administration of O2 removes the hypoxic drive, allowing PaCO2 to rise above the apneic threshold and abolishing central apnea. The critical dependence of periodic breathing at high altitude on fluctuations in PaCO2 is further emphasized by the observation that CO2 inhalation, even in the presence of sustained hypoxia, raises PaCO2 and abolishes central apnea. However, both awake PaO2 and mean nocturnal SaO2 in CHF patients with Cheyne-Stokes respiration are within normal limits and are practically identical to those in CHF patients without Cheyne-Stokes.35,36,37 Thus, the hypoxic dips in Cheyne-Stokes respiration are the result, rather than the cause, of central apnea. Nevertheless, the hypoxic dips during apnea could further the tendency to hyperventilate at the termination of central apnea by amplifying the ventilatory response to CO2 once PaCO2 rises above the ventilatory threshold.30 Ventilatory overshoot with propagation of Cheyne-Stokes respiration would therefore be facilitated by even mild degrees of apnea-related hypoxia. Dips in SaO2 would also facilitate arousal from sleep, which in turn contributes to hyperventilation.
A number of studies have investigated the effects of supplemental oxygen in patients with CHF and Cheyne-Stokes. It must be stressed that most studies were interested in abolishing the dips in SaO2 rather than understanding how such dips contribute to the genesis of Cheyne-Stokes respiration.53–57 All studies were consistent in showing small but significant reductions in the total amount of Cheyne-Stokes respiration. For instance, Hanly showed that low flow O2 administered to patients with CHF reduced the duration of Cheyne-Stokes respiration-CSA mainly during stage 1 sleep, with no significant change during stage 2, slow wave, or rapid eye movement (REM) sleep.55 The administration of O2 was also associated with a more consolidated sleep with a decrease in the number of arousals. Modest reductions in the frequency of central apneas and hypopneas in response to O2 administration have been confirmed by others.54–56 Differences in the effects of O2 in Cheyne-Stokes respiration among patients are most likely related to rising PaCO2 in response to abolition of hypoxic drive. Taken together, these data are consistent with the concept that hypoxia may play a role in aggravating, but is not the major determinant of Cheyne-Stokes in patients with CHF.
Contributing factors to respiratory instabilityTwo additional factors, namely low functional residual capacity and upper airway instability may further contribute to respiratory instability and perpetuation of Cheyne-Stokes respiration. Congestive heart failure patients have a low functional residual capacity that is further reduced by moving from the upright to the supine position. A large functional residual capacity acts as a large reservoir of O2 and CO2 in the body and damps oscillations in PaO2 and PaCO2 that would occur during apnea.45,58 Therefore, reductions in functional residual capacity decrease the lung O2 and CO2 reservoirs and allow greater reductions in PaO2 and greater increases in PaCO2 during apnea.45,58 This could contribute to instability of the respiratory control system. However, Naughton et al.35 have shown that lung volumes in CHF patients with Cheyne-Stokes respiration do not differ from those in patients without it. Thus the role of reduced lung volume in the pathogenesis of Cheyne-Stokes remains uncertain, and if present, will only help to make the respiratory system unstable.
Upper airway instability may play a role in the pathogenesis of Cheyne-Stokes. Alex et al.59 described upper airway occlusion at the onset and at the end of central apnea in patients with CHF. Instability of upper airway resistance could promote the development of respiratory instability. If upper airway resistance increases as ventilation decreases during the decrescendo phase of the hyperpneic portion of Cheyne-Stokes respiration, there will be a tendency to cause an undershoot of ventilation.60 The occasional occluded breath at the onset of central apnea during Cheyne-Stokes59 is compatible with this possibility. On the other hand, decreasing resistance as ventilation increases during the crescendo phase will facilitate overshoot, rapidly driving PaCO2 down and setting up conditions for posthyperventilation apnea. In addition, it is possible that upper airway collapse itself can reflexly precipitate central apnea.62 This suggests an important interaction between upper airway and central controller instability in the pathogenesis of some cases of Cheyne-Stokes respiration. Consistent with this hypothesis, Sahlin et al.,63 studying the overnight polysomnography of 20 patients presenting Cheyne-Stokes, observed that the frequency of apneas and hypopneas in patients with this respiration was significantly higher when patients were in the supine position. It is noteworthy in this context that continuous positive airway pressure (CPAP), which dilates and stabilizes the upper airway,64,65 has been shown to alleviate Cheyne-Stokes.66,67,68 These data must be interpreted with caution because CPAP has many other effects that could damp periodic breathing by a indirect mechanism other than stabilization of the upper airway. Continuous positive airway pressure is an effective treatment for the failing heart, not only because it inflates the lungs but also because it augments cardiac performance by decreasing pre and after load.69,70 On the other hand, the recent observation that Cheyne-Stokes respiration is more frequent in the supine position is compelling evidence that upper airway instability does play a role in the aggravation of the respiration, at least in some patients.
CONSEQUENCES OF CHEYNE-STOKES RESPIRATIONCheyne-Stokes respiration is the consequence of a failing heart. Accordingly, Cheyne-Stokes is ameliorated by therapies that improve myocardial function, such as cardiac resynchronization in patients with CHF associated with conduction disturbances,71 and goes away after heart transplant.72 One important question raised is: once established, does Cheyne-Stokes respiration constitute an additional burden to the patient? It is now recognized that it gives rise to clinical problems largely through its effects during sleep, in agreement with the observations of Harrison et al.73 These effects are similar to those associated with sleep apnea syndromes and lead to disrupted sleep and its consequences. Hanly et al.74 showed that patients with CHF and Cheyne-Stokes had a sleep latency that was significantly shorter than CHF patients without this breathing disorder, suggesting that they suffered from hypersomnolence. In addition, they demonstrated that patients with CHF and Cheyne-Stokes had more stage 1 and 2 nonREM sleep, less REM sleep, and a higher frequency of arousals from sleep than CHF patients without the breathing disorder.72 Interestingly enough, CHF patients with Cheyne-Stokes respiration14 and obstructive sleep apnea75 do not complain of significant subjective sleepiness. The symptoms may overlap with the fatigue that is characteristic in patients with severe CHF.
There is some evidence suggesting that Cheyne-Stokes respiration is a marker of poor prognosis in patients with CHF, but the data is conflicting. Findley et al. reported in an uncontrolled retrospective study that patients with CHF who also suffered from Cheyne-Stokes during sleep had a higher mortality rate than patients without it. Hanly et al.22 prospectively followed a group of 16 patients with stable CHF, 9 of whom had Cheyne-Stokes respiration and 7 of whom did not. Despite comparable LVEF, the combined rate of mortality and heart transplantation was significantly higher in the Cheyne-Stokes group. Similarly, Sin et al.23 observed an increased mortality in CHF patients presenting Cheyne-Stokes respiration. These data suggest that Cheyne-Stokes itself may accelerate disease progression in patients with heart failure.
Conversely, Andreas et al.73 did not observe increased mortality in patients presenting Cheyne-Stokes respiration during the night, but only in patients presenting it while awake. Rebuck et al. followed 78 patients, of whom 42% had Cheyne-Stokes, over a median period of 52 months. The authors were able to confirm an increased mortality in patients presenting sleep disorder breathing (including obstructive sleep apnea, present in 28%) at 500 days, but contrary to their initial hypothesis, the effect was lost at long-term follow-up (52 months).77 Therefore, the effects of Cheyne-Stokes respiration during sleep in patients with CHF remain to be established. It is possible that respiratory instability while awake is more meaningful for mortality than while asleep. Supporting this hypothesis, we have observed that periodic breathing during exercise (a mild form of Cheyne-Stokes) was a powerful predictor of mortality in CHF patients waiting for heart transplant.3
Regardless of the exact impact of Cheyne-Stokes on mortality, there is evidence that it may be detrimental to the failing heart. Blood pressure (BP) and heart rate (HR) oscillate in concert with Cheyne-Stokes cycles, very much as they do during obstructive sleep apnea; that is, peaks occur during the hypernea and troughs during apnea.56,78 These oscillations could be related to the same mechanisms that have been implicated in obstructive sleep apnea, including hypoxia and arousals from sleep, both of which can stimulate sympathetic nerve activity. However, Franklin et al. and Leung et al. 20 found that O2 administration at a sufficient flow rate to abolish dips in SaO2 did not significantly influence BP or HR oscillations during Cheyne-Stokes respiration. These data indicate that mechanisms other than hypoxic dips are involved in precipitating these surges in BP and HR during Cheyne-Stokes. The best explanation for the oscillations in BP and HR during Cheyne-Stokes is related to the intrinsic link between ventilation and the cardiovascular system, which, for instance, also produces oscillations in BP and HR on a breath-to-breath basis. Normal subjects voluntarily reproducing a Cheyne-Stokes respiratory pattern of breathing (in the absence of hypoxia or arousals from sleep) presented profound oscillations in BP and HR in a pattern that was similar to what is seen in CHF patients during Cheyne-Stokes respiration.18 Trinder et al.75 also found that BP oscillations during Cheyne-Stokes in CHF were related to oscillations in ventilation and not to the level of hypoxia. Moreover, when Cheyne-Stokes was abolished by the inhalation of small concentrations of CO2, oscillations in BP and HR were also abolished.20 Regardless of the exact mechanisms, once established, Cheyne-Stokes promotes cyclic increases in BP and HR in concert with the ventilatory cycle,20,56,78 which may contribute to a poor prognosis for CHF patients with Cheyne-Stokes.
Hypoxia and arousals from sleep present during Cheyne-Stokes may also be associated with stimulation of the sympathetic nervous system. Overnight urinary norepinephrine concentrations and daytime plasma norepinephrine concentrations are markedly higher in CHF patients with Cheyne-Stokes than in those without it, and they are directly related to the frequency of arousals from sleep and to the degree of apnea-related hypoxia, but not to left ventricular ejection fraction.79 These data suggest that Cheyne-Stokes can trigger sympathetic activation in patients with CHF. These higher nocturnal and daytime catecholamine concentrations might aggravate myocardial dysfunction. On the other hand, Mansfield et al.80 studied 55 CHF patients and showed that Cheyne-Stokes breathing was associated with worse cardiac function (higher mean pulmonary artery pressure) and higher total body plasma and cardiac norepinephrine. The differences in norepinephrine were due to heart failure and not to apnea severity. Cheyne-Stokes respiration could therefore be a marker of poor prognosis rather than a causative factor. This hypothesis fits with the observation that CHF patients with this breathing disorder have larger left ventricles than those without it.81 Javaheri et al. also observed that Cheyne-Stokes is associated with a lower PaCO2 and a higher rate of ventricular tachycardia.37 These associations do not clarify whether there is any relationship of causality between Cheyne-Stokes and poor prognosis, and further studies are needed.
The discussion of the treatment of Cheyne-Stokes respiration in patients with CHF is beyond the scope of this review. Readers wishing an in depth discussion of this subject are referred to a recent review.82 Briefly, since Cheyne-Stokes respiration probably arises from CHF, the first approach to therapy is to optimize the medical therapy of CHF.83 Failing that, there are a number of other therapeutic options. The most extensively tested intervention is CPAP. When used overnight for 1 to 3 months, CPAP has been shown to alleviate Cheyne-Stokes; to increase LVEF; reduce mitral regurgitation, atrial natriuretic peptide and both urinary and plasma norepinephrine levels. It also improved quality of life and survival.23,67,68,79,84,85 Oxygen administration has been shown to cause a modest reduction in the severity of Cheyne-Stokes respiration, to reduce overnight urinary norepinephrine levels, and cause an increase in peak O2 consumption during graded exercise over periods of 1 to 4 weeks.53–57 Finally, theophylline has been shown to reduce the severity of Cheyne-Stokes over 5 days, but has not been shown to improve cardiac function, neurohumoral activity, or quality of life.86 Pepperell et al. have recently shown in a prospective randomized trial that 1 month of nocturnal-assist servoventilation was able to reduce daytime sleepiness in conjunction with improvements in plasma brain natriuretic peptide and urinary metadrenaline excretion in patients with CHF and Cheyne-Stokes.87 Larger, longer-term randomized trials will be required to determine which, if any, of these interventions are effective for the management of CHF patients with Cheyne-Stokes respiration.88