



Aging populations are a worldwide phenomenon affecting both developed and developing countries. This issue raises serious concerns for both governments and the general population. Regular participation in physical activity and/or exercise training programs can minimize the physiological alterations that occur during aging and may contribute to improvements in health and well-being. The present review will discuss the role of regular exercise training in preventing age-related physiological decline and, consequently, associated chronic diseases. Compelling evidence that regular exercise and/or physical activity can improve quality of life, prevent or control the development of chronic disease and increase life expectancy is shown. In summary, regular exercise training and/or physical activity has an important influence on aging and may help to prevent age-related disorders.
Aging populations are a worldwide phenomenon affecting both developed and developing countries. According to the Brazilian Geographic and Statistics Institute, there were 15 million elderly people in Brazil in the year 2000, which represented 8.6% of the Brazilian population, and this number is expected to increase to 30 million by the year 2030, which will represent 13% of the population (1). This population aging is a serious concern to both governments and the general population because aging changes the profile of a society and necessitates the adaptation of the entire sociopolitical system to a new reality of an increasing demand for geriatric services. This concern is justifiable because there is structural and functional deterioration of almost all physiological systems during aging, even in the absence of discernible disease, resulting in reduced independence and increased incidence and progression of chronic diseases in older adults (2,3).
However, regular participation in physical activity and/or exercise training programs can minimize the physiological alterations that occur during aging and may contribute to improvements in health and well-being (2,3). Numerous studies have shown that exercise training programs improve the muscle strength (4,5), balance (6,7), cardiorespiratory fitness (4,8), metabolism (9), glucose tolerance (10), daily living activities (11) and psychological health (12) of elderly people, even those in their 80s or 90s (13,14). Accordingly, national and international agencies have recommended regular physical activity or exercise participation to promote older adult health and disease prevention (2,15,16).
The purpose of the present review is to discuss the role of regular exercise training in preventing age-related physiological decline and associated chronic diseases.
Exercise, functional decline and chronic disease riskAlthough aging is a multifactorial process that results from the interaction of the primary aging process with the effects of life style, genetics and chronic diseases, age-related functional and structural decline occurs in most physiological systems (2). Cardiorespiratory and muscular capacity decline are two examples. In addition, cardiorespiratory capacity and muscular capacity are important determinants of exercise tolerance and functional capacity in older adults. The basal levels of these variables during middle age are predictors of future incapacity, chronic disease and mortality risk (2–5).
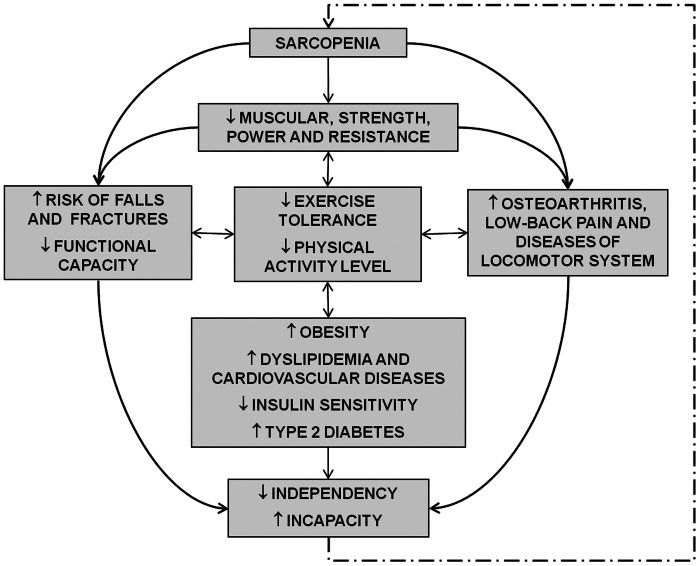
The loss of muscle strength begins around the age of 30. This loss results from a muscle mass reduction that is associated with alterations in the percentage of intramuscular contractile tissue and a reduced capacity for muscular activation (sarcopenia). This issue has received increasing attention from the medical and scientific community in recent decades. It is well documented that the sarcopenia and loss of muscle strength that accompany aging reduce one's ability to perform daily living activities and lower exercise tolerance. In addition, these factors have been implicated in the development of osteopenia and its progression to osteoporosis and are risk factors for knee osteoarthritis (3). Moreover, age-related sarcopenia is also associated with reductions in the basal metabolic rate, fat oxidation, daily living physical activity and energy expenditure, which are associated with visceral and subcutaneous fat accumulation in older adults, resulting in an increased risk for obesity-related locomotor system diseases, as well as cardiovascular disease, dyslipidemia and insulin resistance (2,3,15,17). A schematic representation of the consequences of age-related muscular capacity reduction is shown in Figure 1.

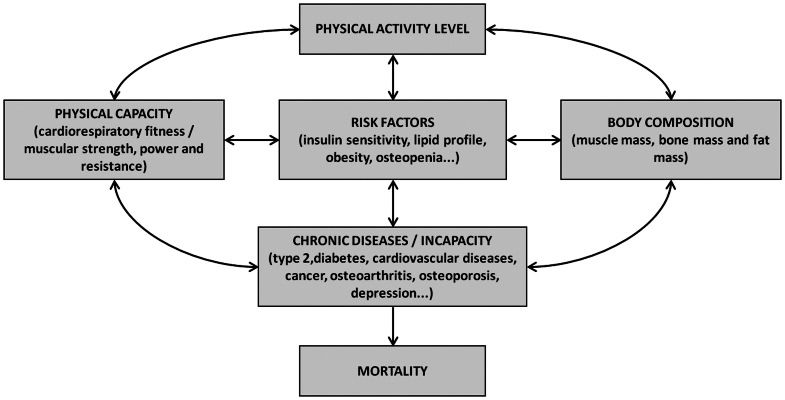
Older people are also less active than young people. Even if they have the same daily physical activity volume, the physical activity intensity performed by the elderly is always lower than is the activity performed by younger adults (2,3). This fact has important implications for the aging process and its consequences because the decline of many physiological variables with advancing age and the incidence of innumerous chronic diseases are increased with lower levels of physical activity. For example, the risk of developing and, consequently, dying from several chronic diseases (i.e., cardiovascular disease, type 2 diabetes, obesity and colon cancer), as well as developing musculoskeletal disorders (i.e., osteoporosis, osteoarthritis and sarcopenia) is lower in individuals with a higher physical fitness or greater daily physical activity levels (Figure 2) (2,15,17).

Schematic representation of the manner in which exercise and/or physical activity may influence disease incidence and, consequently, mortality during aging. Observe that most influences are bi-directional, indicating that the presence of a risk factor or chronic diseases may alter the exercise/physical activity level, increasing the effects of sedentary behavior on disease and mortality.
It is important to note that currently, no lifestyle intervention (including physical activity) has been shown to affect the primary aging process (the aging process independent of behavioral factors). However, participation in regular physical exercise has been shown to increase life expectancy via its influence on the development of chronic diseases and the restoration, at least in part, of the functional capacity and physiological systems of previously sedentary older adults (2–5,15),.
In this context, avoiding a sedentary life style by performing any type or level of daily exercise is a prudent recommendation to follow as it will reduce the impact of aging on some physiological functions, reduce the risk of developing chronic disease and prevent premature mortality, regardless of age.
Aerobic exercise, cardiorespiratory fitness and agingCardiorespiratory fitness, also known as cardiopulmonary capacity, is an important factor influencing risk for cardiovascular and all-cause mortality in men and women (2,18). For example, it was shown that the risk of mortality for men with a cardiorespiratory fitness greater than or equal to 10 metabolic equivalents (METs) is 3 times lower than in men with a cardiorespiratory fitness of less than or equal to 4 METs, independent of any other risk factor (19). The same has been observed in women with a cardiorespiratory fitness of greater than or equal to 9 METs compared to women who have a cardiorespiratory fitness of less than or equal to 6 METs (20).
Moreover, changes in cardiorespiratory fitness throughout life also alter the rate of mortality, even in individuals older than 70 (18). Two studies have analyzed the relative risk for cardiovascular and all-cause mortality in 9777 men aged 20 to 82 years. Two cardiopulmonary exercise tests, separated by a mean interval of 5 years, indicated a lower relative risk for mortality (cardiovascular and all-cause) in men with a high cardiorespiratory fitness in both tests than men with low cardiorespiratory fitness in both tests, whereas individuals who changed their cardiorespiratory fitness by the second test from low to high levels and vice-versa displayed an intermediate relative risk for mortality (21,22). Similar results were found in a study that performed two cardiopulmonary exercise tests, with a mean interval of 8 years, in 867 older men who were 70 years old (23). A clinically important finding of these three studies was that the older men aged 70 to 82 years who improved their cardiorespiratory fitness from low to high levels reduced their mortality risk by approximately 50%, whereas the men who presented reduced cardiorespiratory fitness from high to low levels also had increased mortality risk by approximately 50% (18).
During the primary aging process, there appears to be an inevitable cardiorespiratory fitness decline (after 25 years of age), which can be observed by the parallel decline in the maximum oxygen uptake (VO2MAX) in lifelong trained or untrained individuals. However, a mean difference of approximately 25–30 ml·kg⋅min−1 in the VO2MAX between lifelong aerobically trained and untrained individuals (25 to 65 years of age) is observed, which is maintained as long as the physical training continues (18).
In contrast, the secondary cardiorespiratory fitness aging process (caused by diseases and behavioral factors) appears to be reduced or accelerated following the adoption of a physically active or sedentary lifestyle, respectively. For example, young and middle-aged individuals who trained aerobically to maintain high levels of cardiorespiratory fitness or to participate in competitions demonstrated a lower VO2MAX decline compared to their untrained peers during a 20-year follow-up (24). Similar results were observed in a study indicating reduced VO2MAX decline in high– and moderate–intensity trained individuals (aerobic exercise) at a 20-year follow-up, whereas individuals who only participated in low–intensity physical training displayed an accelerated VO2MAX decline in the same period (25).
Although a higher mortality rate is the most notable clinical consequence of low cardiorespiratory fitness and sedentary living, the lower cardiorespiratory fitness decline resulting from regular aerobic exercise throughout life has other important clinical implications that include the following:
- –
A delay in the onset of physical frailty associated with low cardiorespiratory fitness – Subjects aged 60 to 70 years who have participated in lifelong aerobic exercise usually have a VO2MAX that is similar to 30-year-old sedentary subjects (18). In this context, sedentary subjects may present cardiorespiratory frailty (VO2MAX<18 ml⋅kg⋅min−1) before the subjects who have participated in lifelong aerobic exercise, which results in earlier physical dependency and fewer years with a good quality of life (26).
- –
The maintenance of the functional capacity at adequate levels to maintain homeostasis in situations of physiological stress – Physiological stress situations that promote a marked increase in oxygen consumption, such as major surgeries, may not be tolerated by older subjects with poor cardiorespiratory fitness and may lead to otherwise avoidable morbidity and mortality (27).
- –
Reduced risk of developing chronic diseases – Regular aerobic exercise/physical activity and high cardiorespiratory fitness are associated with a reduced incidence of several chronic diseases (i.e., cardiovascular diseases, type 2 diabetes and some types of cancer) (2,15), which may increase life expectancy (18).
In this context, lifelong participation in aerobic exercise programs is an important strategy not only to increase life expectancy but also to extend the independent life span, improve the quality of the years lived, reduce the risk of developing chronic diseases and reduce the morbidity and mortality risk in situations that promote marked physiological stress (i.e., major surgeries).
Resistance exercise, muscular capacity and agingMuscular strength (the ability of a muscle group to generate force against a resistance) and power (the ability of a muscle group to generate force quickly or work per unit of time) are also important markers of morbidity and mortality. For example, a prospective study followed 8,762 men aged 20 to 80 years for approximately 18.9 years and revealed that there was an inverse association between muscular strength (measured by the supine and leg press exercise 1–repetition maximum [1–RM]) and cancer mortality, independent of any other risk factor, such as age, physical activity level, obesity, smoking, alcohol consumption, clinical conditions prior to follow-up, family history of cardiovascular disease or cardiorespiratory fitness (28). Confirming these data, a meta-analysis including more than 50,000 individuals indicated that the risk of death increased by 67% in subjects within the lower handgrip strength quartile, independent of age, gender and body mass index (29).
Sarcopenia, the loss of muscle mass that accompanies aging, is associated with daily energy expenditure and bone mineral density reductions, which may have implications for the incidence of obesity, cardiovascular disease and osteoporosis (3). In addition to the greater susceptibility to disease, the muscular strength and power loss that results from sarcopenia may reduce exercise tolerance and the capacity to perform daily living activities. For example, a large number of subjects aged 55 years and older have difficulty walking 400 m or carrying 11 kg, and 57% of men and 70% of women in their 80s are unable to perform heavy housework (30), although simple activities may be performed (i.e., moderate walking, stair climbing and carrying objects). In addition, a higher heart rate, blood pressure and respiratory rate response, as well as early and general fatigue are observed (31). The reduced exercise tolerance leads older subjects to avoid these activities, resulting in a further reduction in the muscular capacity, which establishes a vicious cycle, thereby exacerbating the aging process. It is important to emphasize that women are more susceptible to the above mentioned consequences of sarcopenia because of their reduced muscle reserve due to differences in the production of anabolic hormones, which causes the muscular capacity threshold necessary to affect the functional capacity to be crossed at least 10 years earlier than in men (31).
In contrast to what happens with the age-associated cardiorespiratory fitness reduction, the consequences of sarcopenia (loss of muscle, strength, power and endurance) are generally not mitigated by regular aerobic exercise throughout life. However, muscular stress promoted by regular resistance training has been shown to prevent, or at least to reduce, the loss of muscle mass during aging. A pioneering study analyzing knee extensor muscle function and morphology of young and older adults demonstrated that older runners and swimmers (at least 10 years of regular practice in the modality) had a muscle mass (cross-sectional area and fiber type proportion) and strength that was similar to older sedentary adults and lower than in young sedentary adults, whereas subjects practicing resistance training for at least 10 years had levels that were similar to those of sedentary men who were 40 to 50 years younger (32).
It has also been shown that the capacity to improve muscular strength and mass are preserved in previously sedentary older subjects. Elderly individuals practicing resistance training have shown muscle strength improvements of up to 150% (4,5,26). Improvements of 10% to 30% in the muscle fiber cross-sectional area have also been observed in older subjects following 3 to 6 months of resistance training (3,26).
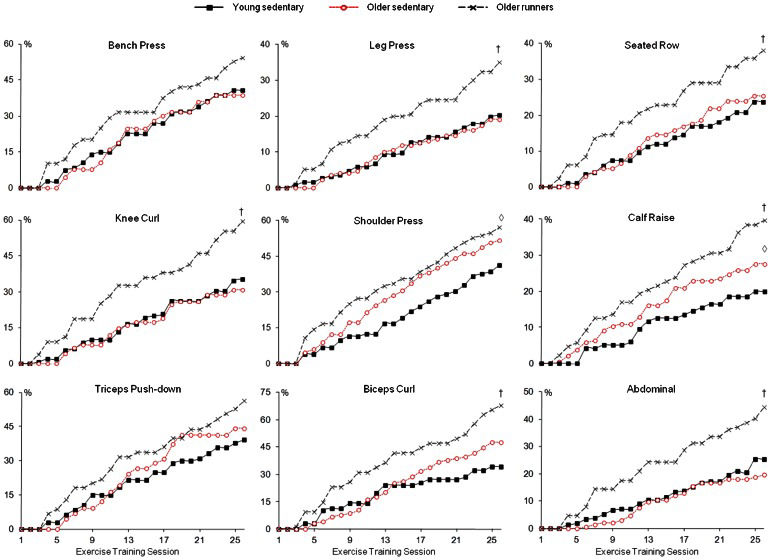
In addition to the preserved capacity to improve muscle mass and strength, older adults appear to be able to similarly adapt to a resistance training workload, even better than do young adults (4,5,33). In studies by our group, sedentary young and older men or women performing the same resistance training program displayed similar increases in muscle strength and resistance training workload progression (4,5), whereas aerobically trained older men (senior runners) displayed greater increases in resistance training workload progression than did sedentary young men (Figure 3) (5).
 men submitted to 13 weeks of resistance training (2 sets of 8 to 12 maximal repetitions in 9 exercises). The training workload was increased by 5% to 10% whenever 2 sets of 12 maximal repetitions with the proper form were achieved, without performing Valsalva maneuver, for two consecutive exercise sessions. Observe that there was no significant difference between sedentary young and sedentary older workload increase for almost all exercises performed (except for the greater increase in the calf raise workload of sedentary older), whereas the older runner workload increase was greater than the sedentary young and sedentary older subjects for most of the exercises performed. †: Difference from the sedentary young and sedentary older group (p<0.05). ◊: Difference from the sedentary young group (p<0.05). Reprinted from (5) Ciolac EG, et al. Resistance exercise intensity progression in older men. Int J Sports Med 2010; 31: 433–8. © Georg Thieme Verlag KG Stuttgart. Used with permission.")
Relative resistance training workload increase curves of young sedentary, older sedentary and older runner (more than 10 years of practice) men submitted to 13 weeks of resistance training (2 sets of 8 to 12 maximal repetitions in 9 exercises). The training workload was increased by 5% to 10% whenever 2 sets of 12 maximal repetitions with the proper form were achieved, without performing Valsalva maneuver, for two consecutive exercise sessions. Observe that there was no significant difference between sedentary young and sedentary older workload increase for almost all exercises performed (except for the greater increase in the calf raise workload of sedentary older), whereas the older runner workload increase was greater than the sedentary young and sedentary older subjects for most of the exercises performed. †: Difference from the sedentary young and sedentary older group (p<0.05). ◊: Difference from the sedentary young group (p<0.05). Reprinted from (5) Ciolac EG, et al. Resistance exercise intensity progression in older men. Int J Sports Med 2010; 31: 433–8. © Georg Thieme Verlag KG Stuttgart. Used with permission.
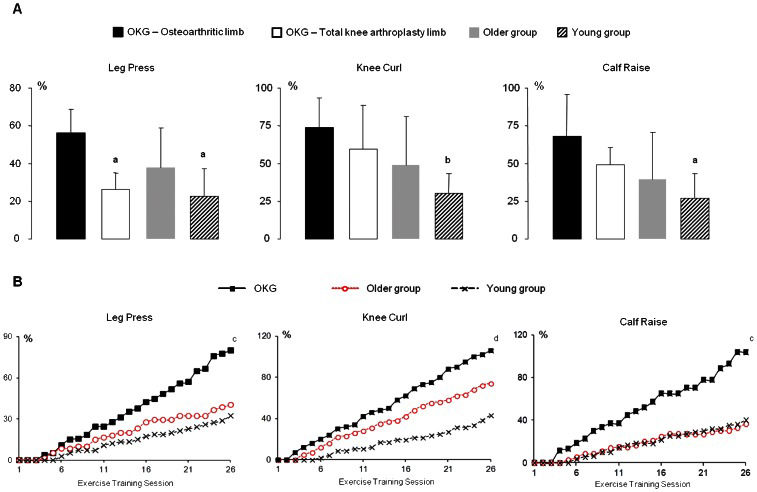
The preserved capacity to improve muscle strength and to adapt to a resistance training workload has been demonstrated even in older subjects with musculoskeletal limitations. A recent study by our group compared muscle strength improvements and resistance training workload adaptation among older women with total knee arthroplasty (TKA) and knee osteoarthritis (KOA) in the contralateral limb, older women without musculoskeletal limitations and healthy young women performing the same resistance training program. The study demonstrated greater relative increases in the muscle strength and resistance training workload intensity in older women with TKA and KOA in the contralateral limb than in older and young women without musculoskeletal limitations over 3 months (Figure 4) (33). It is important to emphasize that there was no injury or major muscle or joint pain in the participants of the three above-mentioned studies. Therefore, resistance training has been demonstrated to be an effective and safe tool to counteract the age-related loss of muscle strength and mass, even in elderly subjects with major musculoskeletal limitations.
 and relative resistance training workload increase curves (B) for older women with total knee arthroplasty and knee osteoarthritis in the contralateral limb (OKG), older women without musculoskeletal limitations (older group) and young women without musculoskeletal limitations (young group) submitted to 13 weeks of resistance training (2 sets of 8 to 12 repetitions of 9 exercises). The training workload was increased by 5% to 10% whenever 2 sets of 12 repetitions with the proper form and avoidance of the Valsalva maneuver were performed for two consecutive exercise sessions. Observe that there was no significant difference between the older group and the young group in terms of the muscle strength or workload increase, whereas the OKG had a greater muscle strength and workload increase for all exercises. adenotes a significant difference from the total knee arthroplasty limb muscle strength (p<0.05). bdenotes a significant difference from the total knee arthroplasty and osteoarthritic limb muscle strength (p<0.05). cdenotes a significant difference from the older group and the young group (p<0.05). ddenotes a significant difference from the young group (p<0.05). Adapted from (33) Ciolac EG, et al. Muscle strength and exercise intensity adaptation to resistance training in older women with knee osteoarthritis and total knee arthroplasty. Clinics 2011; 66: 2079–84. © Clinics. Used with permission.")
Muscle strength (A) and relative resistance training workload increase curves (B) for older women with total knee arthroplasty and knee osteoarthritis in the contralateral limb (OKG), older women without musculoskeletal limitations (older group) and young women without musculoskeletal limitations (young group) submitted to 13 weeks of resistance training (2 sets of 8 to 12 repetitions of 9 exercises). The training workload was increased by 5% to 10% whenever 2 sets of 12 repetitions with the proper form and avoidance of the Valsalva maneuver were performed for two consecutive exercise sessions. Observe that there was no significant difference between the older group and the young group in terms of the muscle strength or workload increase, whereas the OKG had a greater muscle strength and workload increase for all exercises. adenotes a significant difference from the total knee arthroplasty limb muscle strength (p<0.05). bdenotes a significant difference from the total knee arthroplasty and osteoarthritic limb muscle strength (p<0.05). cdenotes a significant difference from the older group and the young group (p<0.05). ddenotes a significant difference from the young group (p<0.05). Adapted from (33) Ciolac EG, et al. Muscle strength and exercise intensity adaptation to resistance training in older women with knee osteoarthritis and total knee arthroplasty. Clinics 2011; 66: 2079–84. © Clinics. Used with permission.
Another benefit of resistance training during aging is the reduction of functional capacity decline or the improvement of the functional capacity of previously sedentary older subjects. The capacity to perform these daily living activities, which have their maximal values in the third decade of life and then begin to decline, is associated with muscle strength and power (3,11,26). For example, greater muscle strength (upper limbs, lower limbs and trunk) displayed an independent and inverse association with functional incapacity incidence in 3,658 men and women during 5 years of follow-up, reducing the risk for incapacity by almost 50%, whereas cardiorespiratory fitness reduced this risk by only 10% (34).
Studies have also demonstrated the improvement of daily activity performance in previously sedentary elderly subjects following resistance training programs (3,11,26,35). For example, our group displays an improvement in several daily activity tasks in older women with TKA and KOA in the contralateral limb following 3 months of resistance training, including sitting-to-standing (∼13%), rising from the floor (∼13%), stair-climbing (∼16%) and 6-minute walking distance (∼23%) (35). In addition, these resistance training-induced improvements were sufficient to restore functional performance, at least in part, to levels similar to those observed in older or even young women (sedentary) without physical limitations (35).
Finally, resistance training has also been shown to reduce the impact of aging on body composition and associated chronic diseases. Older subjects who perform resistance training throughout life display increased bone mass and improved body composition compared to sedentary older subjects or even to those who are engaged in aerobic exercises (2,3). This greater resistance training-related bone mass may have important implications for the prevention of osteoporosis and fractures (3,26). The improved body composition (increase of muscle mass and reduction of fat mass) associated with resistance training may also have health-related benefits, including the prevention of type 2 diabetes, cardiovascular disease, cancer (colon, breast and endometrium), osteoarthritis and falls (3,26,36). With regard to older subjects who were previously sedentary, the benefits of participating in resistance training programs include improvement of body composition, maintenance or even increase of bone mineral density, improvement of insulin sensitivity, reduction of glycated hemoglobin and other benefits (2,3,7,10,26). Moreover, the resistance training-induced reduction of fat mass and increase of muscle mass may have important implications in the treatment of chronic diseases and incapacities associated with disuse. For example, in several diseases, such as type 2 diabetes, there are potential advantages in both reducing the body fat and increasing the muscle mass because these two compartments (fat and muscle) have opposite and independent effects on the insulin sensitivity of older individuals (3,26,31).
Balance, flexibility and agingAlthough the number of studies examining balance exercises is very small as compared to the number of studies analyzing the effects of aerobic and resistance training, the regular practice of balance exercises appears to have health benefits during the aging process. Balance training has been shown to improve balance and stability and thus has been recommended as part of programs to prevent falls (2,37). Moreover, older adults at risk for falls (i.e., women with osteoporosis, frail older individuals and individuals with a history of previous falls) can benefit from prevention programs, including exercise, whereas programs including balance activities, lower-limb resistance training, walking (mainly on irregular surfaces) and flexibility can reduce the number of falls (with or without injury) (2,15,37). Participation in Tai Chi Chuan programs also appears to prevent falls in older people (38,39). Although official statements about exercise prescription for fall prevention do not specify an initial age to begin the practice of specific exercises, there are a few studies demonstrating the benefits of exercise for preventing falls in older adults under the age of 65 years (37).
The number of studies analyzing the effects of flexibility exercises in older adults is even lower than the number of studies of balance exercises, although it is well documented that the range of motion decreases with age. These few studies demonstrate significant flexibility improvements (some joints show range of motion improvements of greater than 40%) with supervised exercise programs, including static stretching or a combination of stretching and rhythmical movements through a full range of motion (yoga or Tai Chi Chuan) (2,40). Therefore, despite the evidence of health benefits not being as clear as the evidence for aerobic and resistance training, flexibility exercises are recommended for maintaining the range of motion necessary for daily activities and physical activities (2,15).
Exercise prescriptionBecause there many studies demonstrating the role of regular exercise training and/or physical activity practice for disease prevention and life expectancy improvement, several medical or health promotion associations have published official scientific statements with minimal exercise and/or physical activity recommendations for disease prevention and health promotion, including specific recommendations for older adults (2),. For example, in 2007, the American College of Sports Medicine and the American Heart Association published a joint position statement on physical activity and public health for older adults (15) and established a minimal exercise/physical activity level (type, quantity and quality) necessary for health maintenance and disease/incapacity prevention in this population. In 2009, the American College of Sports Medicine also published their updated position statement on exercise and physical activity for older adults and emphasized not only the benefits of regular exercise/physical activity engagement for older adults but also the importance of exercising throughout life (2). In these statements, the practice of regular aerobic, resistance, balance and stretching exercises/activities are always recommended (2,15,16). The exercise recommendations for healthy aging and disease prevention in older adults are described in Table 1.
Exercise recommendations for health promotion and chronic disease prevention in older adults.
| Modality | Resistance | Aerobic | Balance | Flexibility |
|---|---|---|---|---|
| Frequency | 2–3 days per week | 3–7 days per week | 2–7 days per week | 2–7 days per week |
| Volume | 1–3 sets of 8–12 repetitions 1 exercise per major muscle group (8–10 exercises) | 20–60 minutes per day (may be divided into sessions of at least 10 min) | No specific recommendation | All major muscle groups should be stressed |
| Intensity | 70 to 80% of 1-maximum repetition (15 to 17 in the 6 to 20 rate of perceived exertion [RPE] scale) (42), ∼1 min recovery between sets | 40–80% of reserve heart rate or VO2MAX (12–15 in the 6–20 RPE scale) (42) | No specific recommendation | 12–13 in the 6–20 RPE scale (42) |
| Observations | Emphasize the use of correct technique. Perform controlled movements and avoid the Valsalva maneuver. Increase workload progressively to maintain relative intensity. Ensure there is at least one day of rest between sessions. If there is equipment available, periodic power training sessions (moderate-intensity, high-velocity movements) will generate muscular power increase. | Moderate-intensity sessions of 30-60 min performed 5 days per week (12-13 in the 6-20 RPE scale) (42) or high-intensity sessions of 20-30 min performed 3 times per week (14-15 in the 6-20 RPE scale) (42) are recommended. Avoid high-impact activities. Walking is the most frequently recommended exercise; however, cycle-ergometer or water-based exercises can be more beneficial for those who do not support weight-bearing activities. | There is no evidence regarding specific frequency, intensity or type of exercise; however, the use of exercises that progressively achieve the following is recommended: 1) reduce the base of support, 2) perturb the center of gravity, 3) stress postural muscle groups and/or 4) reduce sensory input. | Perform sustained stretches rather than ballistic movements. |
Recommendations based on references 2, 4, 5, 15, 31 and 33.
It is important to note that in older adults with one or more chronic diseases, exercise training may be considered a therapy, and such adults should begin an exercise program designed to safely and efficiently treat their disease. However, they should also perform the exercise recommended for disease prevention to prevent the development of an additional chronic condition (15). Moreover, when chronic diseases or even a lack of time prevent older adults from achieving the minimal exercise/physical activity recommendation, they should still engage in exercise (type, quantity, intensity and frequency) accord to their capacity and clinical condition, always trying to avoid sedentary lifestyle (15) because even exercise levels below (mainly in quantity) the minimum recommendation have demonstrated health-related benefits (41).
Although the aging process (and consequently death) is inevitable, a sedentary lifestyle can accelerate its progression by decreasing physical (cardiorespiratory and muscular) fitness and increasing sarcopenia and the incidence of chronic diseases. Moreover, regular exercise and/or physical activity practice may improve the quality of the years lived, in addition to increasing life expectancy. The data presented in this review provide convincing evidence about the importance of engaging in regular exercise and/or physical activity programs throughout life to improve health and the quality of life and to prevent chronic disease during aging.
This work was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP # 2013/00753-9).
No potential conflict of interest was reported.