



To analyze the frequency of the delta F508 (ΔF508) deletion mutation in 108 unrelated cystic fibrosis patients and compare the results with the previously reported data for Brazilian patients. Cystic fibrosis is the leading cause of genetic disease in Caucasians, and the ΔF508 deletion is the most common mutation associated with the disease.
METHODThe frequency of the ΔF508 mutation was assessed by means of a polymerase chain reaction (PCR) followed by detection in 8% silver-stained polyacrylamide gels.
RESULTSTwenty-three of 108 patients (21.3%) were homozygous for the ΔF508 deletion, 50 were heterozygous (46.3%), and the remaining 35 (32.4%) were non-carriers. In terms of alleles, there were 96 mutated (96/216 or 44.45%) and 120 wild-type ones (120/216 or 55.5%).
CONCLUSIONThe 44.45% of affected alleles that were found is higher than the 33% first described in 1993, but slightly lower than the 48% recently reported. Moreover, our data corroborated the idea that the frequency of the ΔF508 mutation is lower in Brazil in comparison to that found in studies carried out in Europe and North American (circa 70.0%), probably due to increased racial miscegenation. These findings must be taken into account before any genetic screening of the population is proposed in Brazil.
Analisar a freqüência da mutação delta F508 (ΔF508) em 108 pacientes não aparentados, com fibrose cística e comparou os resultados com os dados de outros estudos brasileiros. A fibrose cística (CF) constitui a doença genética mais comum em populações caucasianas, sendo a ΔF508 a mais freqüente dentre as mutações relacionadas à doença.
MÉTODOA freqüência da ΔF508 foi analisada por meio da Reação em Cadeia da Polimerase (PCR) seguida de detecção em géis de poliacrilamida a 8%.
RESULTADOSVinte e três dos 108 pacientes foram homozigotos para a mutação (21,3%), 50 foram heterozigotos (46,3%) e os 35 restantes não eram portadores da ΔF508 (32,4%). Em termos de alelos, foram observados 96 mutados (44,45%) e 120 do tipo selvagem (55,55%), ou seja, não portadores da mutação.
CONCLUSÃOA freqüência de 44,45% de alelos mutados encontrada no estudo é mais elevada que os 33,0% descritos em pesquisa realizada em São Paulo em 1993, e ligeiramente mais baixa que os 48,0% encontrados em relatos mais recentes. Além disso, nossos resultados corroboraram a idéia de que a freqüência da mutação ΔF508 é mais baixa no Brasil em comparação a países europeus e nos Estados Unidos da América (cerca de 70,0%), provavelmente devido a maior miscigenação racial. Estas observações terão que ser consideradas antes da implementação de testes genéticos de triagem no Brasil.
Cystic fibrosis (CF) is the most common potentially lethal autosomal recessive disease of Caucasians. The affected gene, CFTR (cystic fibrosis transmembrane conductance receptor), has been determined to code for a chloride channel. Laboratory diagnosis is based on the finding of abnormally high concentrations of chloride in sweat.1 The clinical features of CF are dominated by involvement of the respiratory tract, where obstruction of the airways by thick, sticky mucus and subsequent infection, especially with Pseudomonas species, predominate. In most patients, there is also involvement of the intestinal tract leading to pancreatic insufficiency as a result of obstruction of the pancreatic ducts and subsequent scarring and destruction of exocrine function.2
The CFTR gene is composed of 250,000 base pairs and 27 exons and encodes a protein of 1,480 amino acids. The finding that one particular mutation, the delta F508 (ΔF508), which is a 3 base-pair deletion in exon 10 of the CFTR gene corresponding to codon 508 (phenylalanine) of the protein, is responsible for up to 70.0% of all mutations found in CF patients tested so far has made its molecular detection a very attractive diagnostic tool.3 However, it has been shown that the frequency of this mutation varies significantly among ethnic groups, ranging from 26.0% in Turkey to 88.0% in Denmark.4
A few Brazilian studies carried out in the south and southeast regions of Brazil found differences with respect to the frequency of the ΔF508 mutation among CF patients and also in comparison to those reported in European countries and in the USA.5 In 24 patients in São Paulo, 33.0% of alleles were affected;6 In 17 patients in Rio de Janeiro, a frequency of 35.0% of affected alleles was found.7 In 190 patients from São Paulo, Paraná, and Rio Grande do Sul, 47.0% had the ΔF508 mutation.8 In another study of 120 chromosomes of 60 patients in São Paulo, a frequency of 31.7% of alleles with the ΔF508 mutation was found.9 In 61 patients from the South of Brazil, 50.8 % of the alleles had the mutation.10 Of 44 patients from Rio de Janeiro, 47.7% were affected, with a frequency of 30.7% affected alleles11 More recently, among 160 Brazilian patients in a study conducted in São Paulo, 48.4% of alleles were affected,12 and in 77 patients from the south of Brazil, 48.7% of alleles had the ΔF508 mutation.13 Raskin et al. (2004) concluded that the frequency of the ΔF508 mutation varies remarkably according to geographic and ethnic origin of patients (Euro-Brazilians or Afro-Brazilians).14
PATIENTS AND METHODSThis study was approved by the Ethics Committee of the Faculty of Medicine, University of São Paulo, Brazil.
One-hundred and eight unrelated clinically and laboratory diagnosed CF patients were enrolled in this study to determine the frequency of ΔF508-mutated alleles in this population. We aimed at comparing our data with those previously reported with respect to Brazilian CF patients.5–13
Two milliliters of whole blood samples (EDTA, Becton Dickinson) were drawn from patients after informed consent. DNA extraction was performed according to a previously described salting out protocol.15 The presence of the ΔF508 mutation was determined by means of a classical PCR followed by detection of amplification products in silver-stained polyacrylamide gel electrophoresis according to a previously described protocol,16,17 which was modified to fit our laboratory conditions.
DNA samples of non-carrier subjects (having 2 wild-type alleles) yielded a unique 98 bp (base-pair) fragment, whereas samples from heterozygous patients had 2 amplified fragments, 1 of 98 bp and 1 of 95 bp (lacking 3 base-pairs), and finally DNA from homozygous individuals had only 1 amplified fragment of 95 bp. Amplifications were performed as follows: 10 ng of genomic DNA, 0.4 mM of each of the primers “sense” C16B (5’-GTTTTCCTGGATTATGCCTGGGCA-3’ and “anti-sense” C16D (5’- GTTGGCATGCTTTGATGACGTTTC); 1.5 mM of MgCl2, 2.5 U of Taq DNA polymerase (Amersham-Pharmacia Biotech). After an initial denaturation step of 5 min. at 95°C, 40 cycles of amplification were performed in a Minicycler PT-150, (MJ Research). Cycles consisted of 1 min. at 95°C, 1 min. at 55°C and 1 min. at 72°C, and were followed by a final extension step of 5 min. at 72°C.
Ten microliters of amplification products were analyzed by means of vertical electrophoresis in 8% polyacrylamide gels under non-denaturing conditions for 4 h and 30 min. (25 mA, 450 V, 20 W) in a refrigerated electrophoresis apparatus (Höefer SE 660, Amersham-Pharmacia Biotech). Then, gels were silver-stained, washed, and fixed according a previously described protocol18 and afterwards were dried in a gel dryer (BioRad, USA), at 80°C for 2 h and 30 min.
RESULTSAmong the 108 patients studied, we found 23 (21.3%) homozygous for the ΔF508 deletion mutation, 50 heterozygous (46.3%), and 35 (32.4%) non-carriers. In terms of alleles, there were 96 mutated (96/216 or 44.45%) and 120 wild-type ones (120/216 or 55.5%).
Table 1 summarizes the data of 14 Brazilian studies performed in cystic fibrosis patients according to the number of alleles studied, the region of the country, and the frequency of ΔF508-mutated alleles. Briefly, the data show that the totality of reports included south or southeast regions patients, with a great variability of either ΔF508 mutation frequency as well as other CF-associated mutations (21.0 to 81.0%).
Brazilian studies performed in cystic fibrosis patients according to the number of alleles studied, the region of the country, and the frequency of ΔF508-mutated alleles.
| No. chromosomes | Region of Brazil/State | Frequency | Reference |
|---|---|---|---|
| 48 | Southeast | 33.0 | 6 |
| (São Paulo) | |||
| 34 | Southeast | 35.0 | 7 |
| (Rio de Janeiro) | |||
| 120 | South | 49.0 | 8 |
| (Rio Grande do Sul) | |||
| 48 | South | 27.0 | 8 |
| (Santa Catarina) | |||
| 34 | South | 44.0 | 8 |
| (Paraná) | |||
| 116 | Southeast | 52.0 | 8 |
| (São Paulo) | |||
| 62 | Southeast | 53.0 | 8 |
| (Minas Gerais) | |||
| 120 | Southeast | 31.7 | 9 |
| (São Paulo) | |||
| 122 | South | 50.8 | 10 |
| (Rio Grande do Sul) | |||
| 88 | Southeast | 30.7 | 11 |
| (Rio de Janeiro) | |||
| 320 | Southeast | 48.4 | 12 |
| State ? | |||
| 154 | South | 48.7 | 13 |
| (Rio Grande do Sul) | |||
| 310 | South/Southeast | 81.0* | 14 |
| (Euro-Brazilians) | |||
| 76 | South/Southeast | 21.0* | 14 |
| (Afro-Brazilians) |
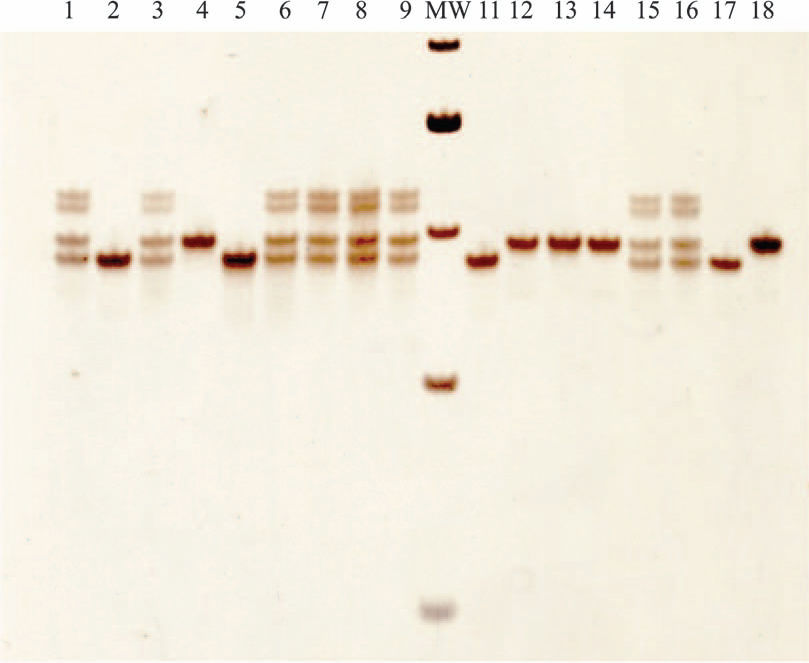
Figure 1 shows the detection of PCR products in 8% polyacrylamide gels. Homozygous patients (ho) have two 95 bp products, indicating 2 alleles with the ΔF508 mutation; heterozygous ones (he) have one 95 bp product one 98 bp product, indicating one ΔF508-mutated allele and one non-carrier (wild type) allele; and finally non-affected individuals or non-carriers (nc) have two 98 bp products, indicating 2 non-mutated alleles. The molecular weight marker used is the 25 bp marker from Invitrogen (USA).
. Lanes 2, 5 and 11 are homozygous patients (two 95 bp fragments), and lanes 4, 12, 13 and 14 are non-carrier patients (two 98 bp fragments). Lane 16 presents the heterozygous control, lane 17 the homozygous control and lane 18 the non-carrier control. Molecular weight (MW) is the 25 bp molecular weight marker (Invitrogen, USA). The 5 MW fragments are (from top to bottom): 150 bp, 125 bp, 100 bp, 75 bp and 50 bp.")
Detection of ΔF508 mutation by PCR in 8% polyacrylamide gels. Lanes 1, 3, 6, 7, 8, 9 and 15 are heterozygous patients (one 98 bp fragment and one 95 bp one). Lanes 2, 5 and 11 are homozygous patients (two 95 bp fragments), and lanes 4, 12, 13 and 14 are non-carrier patients (two 98 bp fragments). Lane 16 presents the heterozygous control, lane 17 the homozygous control and lane 18 the non-carrier control. Molecular weight (MW) is the 25 bp molecular weight marker (Invitrogen, USA). The 5 MW fragments are (from top to bottom): 150 bp, 125 bp, 100 bp, 75 bp and 50 bp.
The frequency of ΔF508-mutated alleles in the present study was 44.5%. This frequency is higher than the 33.0% and the 35.0% described by Martins et al. (1993)6 and De Miranda et al. (1993)7, respectively, but it is noteworthy that they studied a limited number of patients (24 in São Paulo and 17 in Rio de Janeiro). However, Parizotto et al. (1997)9 studied 120 chromosomes from 60 CF patients of the State of São Paulo and reported that only 31.7% of them had ΔF508-mutated alleles. Similarly, Cabello et al. (1999) described a frequency of 30.68% of alleles with the ΔF508 mutation in 88 patients from the State of Rio de Janeiro.11 On the contrary, Raskin et al. (1993)8 studied 190 patients from the south and the southeast of Brazil: 60 from Rio Grande do Sul, 24 from Santa Catarina, 17 from Paraná, 58 from São Paulo and 31 from Minas Gerais. They found an overall frequency of 47.0% of alleles with the ΔF508 mutation. However, when the frequencies were considered according to the state of origin of patients, they found 49.0% in Rio Grande do Sul, 27.0% in Santa Catarina, 44.0% in Paraná, 52.0% in São Paulo and 53.0% in Minas Gerais. In addition, Bernardino et al. (2000)12 and Streit et al. (2003)13 found higher frequencies of alleles with the ΔF508 mutation that were very similar (48.4% and 48.7%, respectively), but the former study did not mention whether the patients were all from the State of São Paulo, and the latter was carried out in the State of Rio Grande do Sul, in the south region of Brazil. Raskin et al. in a series of articles that analyzed the frequency of the ΔF508 mutation as well as other common mutations associated with CF in Brazilian patients19,20,14 initially cited a frequency of 47.0% in Brazilian patients of European origin,19 then a frequency ranging from 30.7 to 50.8%,20 and finally a striking difference in a screening for the 70 most common CF mutations (including ΔF508) between Euro-Brazilians (75.0%) and Afro-Brazilians (21.0%).14
It is interesting to point out that in all polyacrylamide gels that were performed on heterozygous samples, 2 fragments of molecular weights between 100 bp and 125 bp were present. This phenomenon has already been observed and reported,21 but the relevance of these DNA fragments has still to be investigated. Nevertheless, these spurious fragments act as DNA markers for alleles that are heterozygous for the ΔF508 mutation.
The present study added 216 chromosomes to the list of 1,652 already investigated in Brazilian CF patients with respect to the ΔF508 mutation, of which only 284 alleles are certain to belong to patients of the State of São Paulo. The 44.45% of ΔF508-mutated alleles cited in the present study is within the range of frequencies already reported. Furthermore, all performed Brazilian studies (including ours) tend to indicate a lower frequency of ΔF508-mutated alleles in Brazil in comparison to European and North American studies (around 70.0%). This is probably due to the higher genetic heterogeneity of our population. These results emphasize the need to re-evaluate the cost vs. benefit ration regarding DNA-based tests for genetic screening in highly heterogeneous populations such as the Brazilian because they will be surely less effective in detecting ΔF508 mutations as well as in other common CF mutations.