






This study aimed to identify novel GATA5 mutations that underlie familial atrial fibrillation.
METHODS:A total of 110 unrelated patients with familial atrial fibrillation and 200 unrelated, ethnically matched healthy controls were recruited. The entire coding region of the GATA5 gene was sequenced in 110 atrial fibrillation probands. The available relatives of the mutation carriers and 200 controls were subsequently genotyped for the identified mutations. The functional effect of the mutated GATA5 was characterized using a luciferase reporter assay system.
RESULTS:Two novel heterozygous GATA5 mutations (p.Y138F and p.C210G) were identified in two of the 110 unrelated atrial fibrillation families. These missense mutations cosegregated with AF in the families and were absent in the 400 control chromosomes. A cross-species alignment of GATA5 protein sequence showed that the altered amino acids were completely conserved evolutionarily. A functional analysis revealed that the mutant GATA5 proteins were associated with significantly decreased transcriptional activation when compared with their wild-type counterpart.
CONCLUSION:The findings expand the spectrum of GATA5 mutations linked to AF and provide novel insights into the molecular mechanism involved in the pathogenesis of atrial fibrillation, suggesting potential implications for the early prophylaxis and personalized treatment of this common arrhythmia.
Atrial fibrillation (AF) is the most common form of cardiac arrhythmia seen in clinical practice, accounting for approximately one-third of hospitalizations for cardiac rhythm disturbances. The prevalence of AF increases markedly with advancing age, ranging from 1 to 2% of the general population to 5 to 15% of individuals in their 80s (1). The lifetime risk of developing AF is approximately 25% in individuals aged 40 years or older (2). The chaotic heart rhythm is responsible for a variety of symptoms, including palpitations, dizziness, and shortness of breath, and it is associated with degraded quality of life, reduced exercise capacity, cognitive dysfunction, tachycardiomyopathy, thromboembolic strokes, congestive heart failure, and even death (1,3,4). The mortality rate of patients with AF is approximately two times that of subjects with a normal sinus rhythm (5). The rate of ischemic stroke among patients with AF averages 5% per year, 2 to 7 times that of individuals without AF (6). Additionally, when transient ischemic attacks and clinically “silent” strokes documented by brain imaging are included, the rate of cerebral ischemia accompanying nonvalvular AF exceeds 7% per year (7). Among the patients in the Framingham Heart Study with rheumatic heart disease and AF, the stroke risk was increased 17-fold compared with age-matched controls (8). Given the frequency of comorbidities, AF imposes a huge economic burden on both the individual and society as a whole, and the economic burden for society is expected to increase in the near future due to the aging population (9). Despite the high prevalence and clinical significance of AF, its underlying molecular etiology remains largely unknown.
AF can occur in the context of various structural heart diseases or systemic disorders, including ischemic heart disease, valvular heart disease, congenital heart disease, cardiomyopathy, cardiac surgery, pericarditis, myocarditis, congestive heart failure, essential hypertension, diabetes mellitus, hyperthyroidism, and electrolyte imbalance (1,10,11). However, in 30 to 45% of the cases, especially among those younger than 60 years old, AF occurs without any known risk factors, a condition known as “lone AF”. At least 15% of patients have a positive family history and are considered to have familial AF (12). Accumulating evidence from epidemiological studies highlights the familial aggregation of AF and the increased risk of AF among the close relatives of patients with AF, strongly suggesting a hereditary determinant for AF (13-15). Following genome-wide linkage analysis with polymorphic genetic markers, specific susceptibility loci for AF have been mapped to human chromosomes 10q22, 6q14–16, 11p15.5, 5p15, 10p11–q21, and 5p13, and AF-causing mutations in two genes, KCNQ1 on chromosome 11p15.5 and NUP155 on chromosome 5p13, have been identified and characterized (16). Analyses of candidate genes and genome-wide association studies have revealed a long list of AF-associated genes, including KCNE2, KCNH2, KCNA5, KCNJ2, KCNN3, GJA1, GJA5, NPPA, ZFHX3, and SCN5A (16). Nevertheless, AF demonstrates substantial genetic heterogeneity, and the genetic defects that lead to AF in an overwhelming majority of patients have not yet been identified.
It is now well established that abnormal embryological development of the myocardial sleeves clothing the systemic venous tributaries and the pulmonary veins at their junctions with the atrial chambers is a major anatomic defect associated with AF (17). Recent studies underline the pivotal role of several transcription factors, including NKX2-5, GATA4, GATA5, and GATA6, during cardiogenesis (18), and mutations in NKX2-5, GATA4, and GATA6 have been causally implicated in the pathogenesis of AF (19-24). GATA5 is a member of the GATA family of transcription factors, and its expression and functions overlap with those of GATA4 and GATA6 during cardiac development, especially the synergistic regulation of target gene expression with NKX2-5. This relationship provides a logical rationale for screening GATA5 as a candidate gene associated with familial AF (25).
MATERIALS AND METHODSEthics statementThis study was performed in compliance with the ethical principles of the revised Declaration of Helsinki (Somerset West, Republic of South Africa, 1996). The research protocol was reviewed and approved by the local institutional ethics committee, and written informed consent was obtained from all participants prior to the study.
Study participantsA cohort of 110 unrelated probands with familial AF was identified among the Chinese Han population. The available relatives of the probands who harbored the identified GATA5 mutations were also included. A total of 200 ethnically matched unrelated healthy individuals were recruited as controls. Peripheral venous blood specimens and clinical data, including medical records and electrocardiogram (ECG) and echocardiography reports, were collected. The study subjects were clinically classified using a consistently applied set of definitions (12). Briefly, AF was diagnosed when ECGs demonstrated no P waves and irregular R-R intervals, regardless of clinical symptoms. Lone AF was defined as AF that occurred in individuals less than 60 years of age without evidence of other cardiac or systemic diseases after physical examination, ECG, transthoracic echocardiogram, and extensive laboratory tests. Familial AF was designated when lone AF occurred in one or more first-degree relatives of the proband. Relatives were classified as 'unaffected’ if they were asymptomatic and had a normal ECG. In addition, paroxysmal AF was defined as AF that lasted more than 30 seconds and terminated spontaneously. Persistent AF was defined as AF that lasted more than seven days and required either pharmacologic therapy or electrical cardioversion for termination. AF that was refractory to cardioversion or that was allowed to continue was classified as permanent.
Genetic studiesGenomic DNA from all participants was extracted from peripheral venous blood lymphocytes using the Wizard Genomic DNA Purification Kit (Promega, Madison, WI, USA). The entire coding region and the flanking splice junction sites of GATA5 were sequenced in 110 unrelated index patients with familial AF, and GATA5 genotyping was conducted for the available relatives of mutation carriers and 200 ethnically matched unrelated healthy controls to determine the presence of the mutations identified in the probands. The reference genomic DNA sequence of GATA5 was obtained from GenBank (accession No. NT_011362). The primer pairs used to amplify the coding exons and exon/intron boundaries of GATA5 using polymerase chain reaction (PCR) were designed as previously described using Primer 3 software (http://frodo.wi.mit.edu), (26). PCR was performed using HotStar Taq DNA Polymerase (Qiagen GmbH, Hilden, Germany) on a PE 9700 Thermal Cycler (Applied Biosystems, Foster, CA, USA). The amplicons were purified with a QIAquick Gel Extraction Kit (Qiagen), and both strands of each PCR product were sequenced using a BigDye® Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems) and an ABI PRISM 3130 XL DNA Analyzer (Applied Biosystems). The DNA sequences were analyzed with the DNA Sequencing Analysis Software v5.1 (Applied Biosystems). The variant was validated by resequencing an independent PCR-generated amplicon from the subject, and it met our quality control thresholds with a call rate greater than 99%.
Alignment of multiple GATA5 protein sequencesMultiple GATA5 protein sequences across various species were aligned using the online program MUSCLE, Version 3.6 (http://www.ncbi.nlm.nih.gov/).
Construction of the recombinant pcDNA3.1-hGATA5 expression plasmidHuman fetal cardiac tissue specimens were previously collected and preserved in RNAlater RNA stabilization reagent (Qiagen). Total RNA was prepared using an RNeasy Protect Mini Kit (Qiagen). Reverse transcription was performed with an oligo(dT)20 primer using SuperScript III reverse transcriptase (Invitrogen, Carlsbad, CA, USA). The full-length wild-type human GATA5 cDNA, including partial 5’- and 3’-untranslated regions, was PCR amplified using pfuUltra high-fidelity DNA polymerase (Stratagene, La Jolla, CA, USA). The following primer pairs were used for the specific amplification of the GATA5 transcript: forward, 5’-GTA, GCT, AGC, CAC, CGC, CGT, GCC, CTG, CCG-3’, and reverse, 5’-GAT, GCG, GCC, GCT, GTT, CCC, CTG, ACA, TGG, GC-3’. A 1296-base pair PCR fragment was digested with the endonucleases NheI and NotI (TaKaRa, Dalian, Liaoning, China). The digested product was fractionated using 1.5% agarose gel electrophoresis, purified using a QIAquick Gel Extraction Kit (Qiagen), and then subcloned into pcDNA3.1 (Promega) to generate the eukaryotic expression vector, pcDNA3.1-hGATA5.
Site-directed mutagenesisThe identified mutation was introduced into wild-type GATA5 using a QuickChange II XL Site-Directed Mutagenesis Kit (Stratagene) with a complementary pair of primers. The mutant was sequenced to confirm the desired mutation and to exclude any other sequence variations.
Reporter gene assayThe atrial natriuretic factor (ANF)-luciferase reporter construct (ANF(-2600)-Luc), which contains the 2600-bp 5’-flanking region of the ANF gene, was graciously provided by Dr. Ichiro Shiojima from Chiba University School of Medicine (Chiba-shi, Chiba, Japan). HEK-293 cells were cultured in Dulbecco’s modified Eagle’s medium supplemented with 10% fetal calf serum. The ANF(-2600)-Luc reporter construct and an internal control reporter plasmid pGL4.75 (hRluc/CMV, Promega), were used in transient transfection assays to examine the transcriptional activation activity of the GATA5 mutant. HEK-293 cells were transfected with 0.4 μg of wild-type or mutant pcDNA3.1-hGATA5, 0.4 μg of the ANF(-2600)-Luc reporter construct, and 0.04 μg of the pGL4.75 control reporter vector using PolyFect Transfection Reagent (Qiagen). For the cotransfection experiments, 0.2 μg of wild-type pcDNA3.1-hGATA5, 0.2 μg of mutant pcDNA3.1-hGATA5, 0.4 μg of ANF(-2600)-Luc, and 0.04 μg of pGL4.75 were used. Firefly luciferase and Renilla luciferase activities were measured using the Dual-Glo luciferase assay system (Promega) 48 h after transfection. The activity of the ANF promoter is presented as the fold activation of Firefly luciferase relative to Renilla luciferase. A minimum of three independent experiments were performed for wild-type and mutant GATA5.
Statistical analysisThe data are expressed as the mean ± SD. Continuous variables were tested for normality of distribution, and Student’s unpaired t-test was used to compare numeric variables between two groups. The categorical variables were compared between two groups using Pearson’s chi-squared test or Fisher’s exact test, when appropriate. A two-sided p-value less than 0.05 was considered statistically significant.
RESULTSClinical characteristics of the study populationA cohort of 110 unrelated index patients with familial AF was enrolled, clinically evaluated and compared with 200 ethnically matched, unrelated healthy individuals. None of the subjects had traditional risk factors for AF. There were no significant differences between the proband and control groups in baseline characteristics, including age, gender, body mass index, blood pressure, fasting blood glucose, serum lipid levels, left atrial dimension, left ventricular ejection fraction, and heart rate at rest. The baseline clinical characteristics of the 110 probands with familial AF are listed in Table 1).
Baseline clinical characteristics of the 110 probands with familial atrial fibrillation.
| Parameter | n or mean | % or range |
|---|---|---|
| Male | 65 | 59 |
| Age of onset | 45.3 | 22–59 |
| Paroxysmal atrial fibrillation on presentation | 82 | 75 |
| Progression to permanent atrial fibrillation | 24 | 22 |
| History of cardioversion | 72 | 65 |
| History of pacemaker | 7 | 6 |
| Resting heart rate (bpm) | 75.6 | 50–160 |
| Systolic blood pressure (mmHg) | 125.2 | 90–136 |
| Diastolic blood pressure (mmHg) | 82.8 | 60–88 |
| Body mass index (kg/m2) | 22.1 | 20–24 |
| Left atrial dimension (mm) | 38 | 26–40 |
| left ventricular ejection fraction | 0.6 | 0.5–0.7 |
| Fasting blood glucose (mmol/L) | 4.6 | 3.6–5.8 |
| Total cholesterol (mmol/L) | 3.5 | 3.2–5.5 |
| Triglycerides (mmol/L) | 1.2 | 0.7–1.6 |
| Medications | ||
| Amiodarone | 68 | 62 |
| Warfarin | 62 | 56 |
| Beta blocker | 16 | 15 |
| Calcium channel blocker | 23 | 21 |
| Digoxin | 26 | 24 |
Two heterozygous missense mutations in GATA5 were identified in two of 110 unrelated probands. The total population prevalence of GATA5 mutations based on the proband cohort was approximately 1.82%. Specifically, a thymine to adenine transversion in the second nucleotide of codon 138 (c.413A→T), resulting in a tyrosine (Y) to phenylalanine (F) substitution at amino acid 138 (p.Y138F), was identified in the proband from Family 1. A thymine to guanine transversion in the first nucleotide of codon 210 (c.628T→G), corresponding to a cysteine (C) to glycine (G) substitution at amino acid 210 (p.C210G), was discovered in the proband from Family 2. The sequence chromatograms showing the detected heterozygous GATA5 mutations of c.413A→T and c.628T→G in contrast to control sequences are shown in Figure 1). The two variants were not observed in the 400 control alleles nor were they found in the NCBI SNP database (http://www.ncbi.nlm.nih.gov/SNP). Genetic scans of each family showed that the variation was present in all affected living family members but absent in the unaffected family members who were examined. An analysis of the pedigrees demonstrated that in each family, the mutation cosegregated with AF, which was transmitted in an autosomal dominant pattern with complete penetrance. The pedigrees of the two families are illustrated in Figure 2. The phenotypic characteristics and genetic screening results for the affected family members are summarized in Table 2).
 and T/G (Figure 1B) nucleotides in the probands from Families 1 and 2, respectively, (mutant) or the homozygous A/A (Figure 1A) and T/T (Figure 1B) nucleotides in the corresponding controls (wild-type). The square denotes the nucleotides comprising a GATA5 codon.")
Sequence electropherograms showing the GATA5 mutations in contrast with their corresponding controls. The arrow indicates the heterozygous A/T (Figure 1A) and T/G (Figure 1B) nucleotides in the probands from Families 1 and 2, respectively, (mutant) or the homozygous A/A (Figure 1A) and T/T (Figure 1B) nucleotides in the corresponding controls (wild-type). The square denotes the nucleotides comprising a GATA5 codon.

The pedigrees of the families with atrial fibrillation. The families are designated as Family 1 and Family 2. Family members are identified by generation and number. Squares indicate male family members; circles, female members; a symbol with a slash, a deceased member; closed symbols, affected members; open symbols, unaffected members; arrows, probands; ''+’’, carriers of the heterozygous mutations; and ''−’’, non-carriers.
Phenotypic characteristics and the GATA5 mutation status of the affected pedigree members.
| Subject Information | Phenotype | Electrocardiogram | Echocardiogram | Genotype | |||||
|---|---|---|---|---|---|---|---|---|---|
| Identity | Gender | Age at time of study (years) | Age at first diagnosis of AF (years) | AF (classification) | QRS interval (ms) | QT / QTc | LAD (mm) | LVEF (%) | GATA5 mutations |
| Family 1 | Y138F | ||||||||
| I-2 | F | 75 | 44 | Permanent | 98 | 398/417 | 40 | 60 | +/– |
| II-1 | M | 52 | 38 | Paroxysmal | 92 | 350/458 | 35 | 68 | +/– |
| II-6 | F | 46 | 42 | Persistent | 90 | 368/405 | 32 | 65 | +/– |
| III-1 | F | 26 | 25 | Paroxysmal | 88 | 372/437 | 28 | 64 | +/– |
| Family 2 | C210G | ||||||||
| I-1 | M | 72a | 45 | Permanent | 102 | 362/420 | 42 | 58 | N/A |
| II-3 | M | 50 | 32 | Paroxysmal | 98 | 414/443 | 35 | 66 | +/– |
| III-2 | F | 24 | 24 | Paroxysmal | 90 | 356/452 | 30 | 62 | +/– |
Note: AF = atrial fibrillation; F = female; M = male; N/A = not available or not applicable; LAD = left atrial dimension; LVEF = left ventricular ejection fraction; QT = QT interval; QTc = corrected QT interval. + indicates present and – denotes absent. a Age at death.
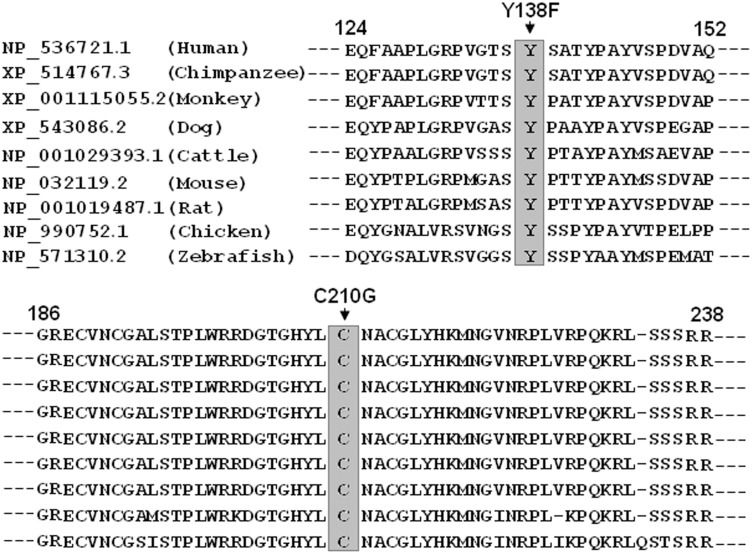
A cross-species alignment of GATA5 protein sequences showed that the altered amino acids were completely conserved evolutionarily (Figure 3), suggesting that these amino acids are functionally important.
Transcriptional activity of the GATA5 mutants are completely conserved evolutionarily.")
Wild-type GATA5, Y138F-mutant GATA5, and C210G-mutant GATA5 increased the transcriptional activity of the ANF promoter approximately 13-fold, 5-fold, and 2-fold, respectively. When wild-type GATA5 was coexpressed with the same amount of Y138F-mutant GATA5 or C210G-mutant GATA5, the transcriptional activity of the ANF promoter was increased approximately 7-fold and 4-fold, respectively. These results reveal that each of the two GATA5 mutations is associated with significantly reduced activation activity when compared with wild-type GATA5 (Figure 4).
, mutant Y138F or mutant C210G, alone or in combination. Expression of the mutant proteins results in significantly reduced transactivation of the ANF promoter. Experiments were performed in triplicate, and means and standard deviations are shown. ∗∗ and ∗ indicate p<0.0005 and p<0.001, respectively, when compared with wild-type GATA5.")
Functional defects associated with GATA5 mutations. Activation of the ANF-luciferase reporter in HEK-293 cells by wild-type GATA5 (WT), mutant Y138F or mutant C210G, alone or in combination. Expression of the mutant proteins results in significantly reduced transactivation of the ANF promoter. Experiments were performed in triplicate, and means and standard deviations are shown. ∗∗ and ∗ indicate p<0.0005 and p<0.001, respectively, when compared with wild-type GATA5.
In the present study, we report two novel heterozygous missense mutations of GATA5 identified in two AF families. In each family, the mutant allele is present in all of the affected living family members but absent in the unaffected relatives who were examined and in the 400 control chromosomes. A cross-species alignment of GATA5 protein sequences demonstrated that the altered amino acids are completely conserved evolutionarily. The functional analysis demonstrated that the mutant GATA5 proteins are associated with significantly decreased transcriptional activation. Therefore, it is very likely that functionally impaired GATA5 is responsible for AF in these families. Given recently reported GATA5 mutations in a larger cohort of AF patients (26), GATA5 mutations may be a relatively common molecular defect associated with the pathogenesis of AF.
GATA transcription factors are a group of zinc finger–containing, DNA-binding proteins characterized by their ability to bind to the consensus DNA sequence “GATA”. In vertebrates, the GATA family comprises six members (GATA1–6), of which GATA4–6 are expressed in various mesoderm- and endoderm-derived tissues, especially in the embryonic heart (18). The GATA5 gene maps to human chromosome 20q13.33 by fluorescence in situ hybridization and encodes a 397–amino acid protein (27). An alignment of GATA5 with GATA4 suggests that the structural domains associated with GATA5 function consist of two transcriptional activation domains (TAD1: 1–49; TAD2: 107–154), two adjacent zinc fingers (ZF1: 187–212; ZF2: 242–266), and one nuclear localization signal (NLS: 226–296). The two TADs are both important to the transcriptional activity of GATA5. The C-terminal ZF is essential for DNA sequence recognition and binding to the consensus motif, whereas the N-terminal ZF is crucial for the stability and sequence specificity of protein-DNA binding and transcriptional activation by GATA factors. Most of the protein–protein interactions of GATA factors are mediated by their C-terminal ZF. The NLS sequence is associated with the subcellular trafficking and distribution of GATA5. The p.Y138F and p.C210G GATA5 mutations identified in this study are located in the TAD2 and ZF1, respectively; thus, they may affect the transcriptional activity of GATA5.
It has been demonstrated that GATA5 is an upstream regulator of multiple genes expressed during embryogenesis, including the genes that encode atrial natriuretic factor (ANF), brain natriuretic peptide, α myosin heavy chain, β myosin heavy chain, and cardiac troponin C and I (18). Hence, the functional effect of the identified GATA5 mutations can be explored by analyzing the transcriptional activity of the ANF promoter in cells transfected with a GATA5 mutant or its wild-type counterpart. In this study, the functional characteristics of the novel GATA5 mutations identified in our familial AF patients (p.Y138F and p.C210G) were investigated using transcriptional activity assays, and the significantly reduced transcriptional activity was observed following the expression of the mutant proteins. These findings indicate that dysfunctional GATA5 is potentially an alternative pathological mechanism involved in AF, although the functional roles of the recently reported AF-associated GATA5 mutations remain to be addressed (26).
The findings that dysfunctional GATA5 confers susceptibility to AF may be partially attributable to the abnormal development of the pulmonary venous myocardium. The pulmonary venous vessel is surrounded by a layer of myocardium known as the pulmonary myocardial sleeve, which is believed to be responsible for the initiation and maintenance of AF by several potential arrhythmogenic mechanisms that favor reentry, including enhanced intrinsic pacemaker activity, anisotropic arrangement of the myocardial fibers and slowed conduction (28-30). Genetic-labeling lineage-tracing studies have demonstrated that NKX2-5 is expressed in the atria and pulmonary myocardium and is important in the localization of the sinoatrial node during embryogenesis. NKX2-5 may act as a repressor of the sinoatrial node lineage gene program, limiting pacemaker activity to the sinoatrial and atrioventricular nodes. When NKX2-5 expression decreased in a hypomorphic model, the pulmonary cardiomyocytes switched to connexin40-negative, HCN4-positive cells, a nodal-like phenotype with pacemaker activity (30). In NKX2-5 knockout mouse embryos, HCN4 was overexpressed in the whole embryonic heart, whereas connexin40 expression was suppressed and ectopic pacemaker cells were observed throughout the heart tube (31). In humans, AF has been observed as an isolated phenotype or as a part of compound phenotypes in patients carrying NKX2-5 mutations (32-34). Therefore, as a transcriptional cooperative partner of NKX2-5 (29), GATA5, when loss-of-function mutations occur, may contribute to the altered formation of the pulmonary myocardium sleeve and the shift of the pulmonary myocardium to a sinoatrial node–like phenotype, hence creating an electrophysiological substrate for AF.
Some downstream genes are upregulated by GATA5, and mutations in several target genes have been associated with AF, including the ANF genes (35). Therefore, it is likely that mutated GATA5 predisposes affected individuals to AF by downregulating the expression of these target genes.
In conclusion, the present investigation links GATA5 loss-of-function mutations to familial AF and provides novel insights into the molecular mechanisms involved in the pathogenesis of AF. Furthermore, these results have potential implications for early prophylactic therapies and personalized treatment for AF.
We are deeply thankful to the participants for their devotion to the study. This work was funded in part by grants from the National Natural Science Fund of China (81070153) and the Shanghai Pujiang Program (09PJ1410400).
No potential conflict of interest was reported.
Gu JY, Xu JH, and Yu H contributed to the experimental design, the clinical and experimental research, the analysis and interpretation of the data, and manuscript writing. Yang YQ contributed to the study design, the analysis and interpretation of the data, and the initial drafting and review of the manuscript.