





To analyze the usefulness of the weight gain/height gain ratio from birth to two and three years of age as a predictive risk indicator of excess weight at preschool age.
METHODS:The weight and height/length of 409 preschool children at daycare centers were measured according to internationally recommended rules. The weight values and body mass indices of the children were transformed into a z-score per the standard method described by the World Health Organization. The Pearson correlation coefficients (rP) and the linear regressions between the anthropometric parameters and the body mass index z-scores of preschool children were statistically analyzed (alpha = 0.05).
RESULTS:The mean age of the study population was 3.2 years (±0.3 years). The prevalence of excess weight was 28.8%, and the prevalence of overweight and obesity was 8.8%. The correlation coefficients between the body mass index z-scores of the preschool children and the birth weights or body mass indices at birth were low (0.09 and 0.10, respectively). There was a high correlation coefficient (rP = 0.79) between the mean monthly gain of weight and the body mass index z-score of preschool children. A higher coefficient (rP = 0.93) was observed between the ratio of the mean weight gain per height gain (g/cm) and the preschool children body mass index z-score. The coefficients and their differences were statistically significant.
CONCLUSION:Regardless of weight or length at birth, the mean ratio between the weight gain per g/cm of height growth from birth presented a strong correlation with the body mass index of preschool children. These results suggest that this ratio may be a good indicator of the risk of excess weight and obesity in preschool-aged children.
The birth weight measured within the first hour following birth reflects the nutritional status of the newborn and is considered an appropriate indicator of health. In addition, birth weight influences the growth and development of the child and has long-term repercussions for health in adulthood.1
Studies have found that childhood obesity is associated with obesity and a higher risk of non-transmissible chronic diseases in adult life. Childhood obesity also contributes to psychosocial dysfunction in childhood and adolescence.2,3
Childhood obesity substantially contributes to childhood illness and may be a major cause of ill health in adulthood.4 Due to these health risks, it is of extreme concern that the onset of overweight and obesity is being detected at progressively younger ages.5
According to Martins & Carvalho,6 several factors are associated with overweight and obesity. For example, there is a positive correlation between birth weight and excess weight in childhood.
He et al7 analyzed 1,322 Chinese children in a national case study to identify risk factors for obesity in preschoolers. Their findings indicated a positive relationship between obesity and a birth weight ≥4 kg, which was the main risk factor for excess weight in children of 3 years or younger. However, in a prospective longitudinal study carried out in the United Kingdom examining 848 children evaluated at birth, Ong et al8 found an inverse relationship between birth weight and obesity at the age of five. The children born with a lower weight, length and ponderal index grew more rapidly between 0 and two years of age and were taller, heavier and had higher body mass indices at the age of five.
Changes in population nutritional profiles in recent decades have been characterized by an increase in the number of obese children at progressively younger ages. Consequently, it has become important to evaluate the factors that contribute to the development of childhood obesity. The present study aimed to analyze the usefulness of the ratio of weight gain/height gain since birth to two and three years of age as a predictive risk indicator of overweight and obesity at preschool age.
MATERIALS AND METHODSThis study is based on the analysis of variables taken from the database generated during the study “Early prevention of overweight and obesity in children attending public daycare centers of Taubaté, São Paulo state.” The data, collected in 2009, are from a representative sample of children aged two and three years who were enrolled at local public daycare centers in the town of Taubaté, in the state of São Paulo, Brazil.
Sampling was probabilistic, by conglomerates, and used a list of 59 public daycare centers provided by the Department of Education and Culture of the Taubaté City Council. Daycare centers were designated as the sampling unit. Using an alpha of 5% and a power of 90%, and taking into account a body mass index (BMI) mean of 16.4 kg/m2 with a confidence interval of ±¼ SD (standard deviation) for preschoolers, the necessary sample size was estimated to be 408 children for the initial study. The first nine daycare centers selected by randomized draw comprised the final sample of 449 preschool children (PSC) initially included in the study.
A questionnaire designed for the study was used to collect birth data. Birth weight and length were collected from the relevant maternity records or reported by the mothers. The non-return rate was 8.9%, reducing the size of the final sample to 409 children.
The exclusion criteria included chronic diseases or growth disorders, extremely low birth weight (<1,500 g), birth length ±4 SD from the mean, absence from the daycare center on the days scheduled for data collection after three tries and lack of parental consent.
Weight (W) and height (H)/length (L) were measured according to internationally recommended rules, and the BMI was calculated. The children were weighed on a portable electronic balance (SECA® - 150 kg, precision of 10 g), wearing no shoes and minimal clothes. A portable stadiometer (WISO®) was used to measure height. All anthropometric measurements were obtained using the methods described by Lohman et al.9
For statistical analysis purposes, the W and BMI of the PSC were transformed into z-scores according to World Health Organization reference data. The Pearson correlation coefficients (rP), the linear regressions between anthropometric parameters, and the BMI z-scores of the PSC (as indicator of weight excess) were examined and statistically evaluated (alpha = 0.05). Correlations between different parameters were estimated using GraphPad Prism 5.0 software.
Nutritional status was defined by criteria proposed by the Brazilian Ministry of Health. According to these diagnostic criteria, children with excess weight are defined as all children with a BMI z-score ≥+1. Children with a BMI z-score >+2 and ≤+3 are classified as overweight. Those children with a BMI z-score >+3 are classified as obese.10
The mean monthly weight gain and the mean weight gain per cm of height gain were calculated from the difference between the weight and birth length and the weight and height of each child at the time of the evaluation.
The study was approved by the Research Ethics Committee of the Public Health Program of the University of São Paulo (Protocol no. 1877 from 2009). Informed consent forms were sent to the mothers or guardians by the daycare centers and were returned duly completed and signed before the start of the data collection.
RESULTSThe population studied was composed of 409 preschoolers aged two and three years. The population had a mean age of 3.2 years (±0.3 years). Out of the 409 preschoolers, 210 (51.3%) were boys, and 199 (48.7%) were girls. The prevalence of excess weight was 28.8% (including 8.8% who were overweight or obese).
The population sample mean for W gain per month of age since birth was 318.5 g (±66.1 g), and the mean of W gain per centimeter of H growth was 249.0 g (±37.1 g).
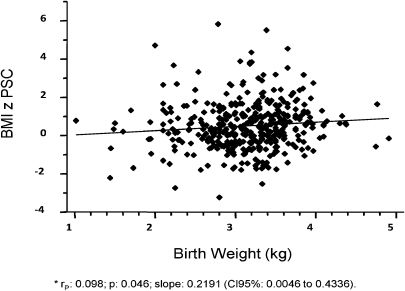
The correlation coefficients between the BMI z-score of the PSC and birth weight or BMI at birth were very low (0.09 and 0.10, respectively), although statistically significant (Figures 1 and 2). The PSC BMI z-scores did not correlate with the age of the children or their length at birth.
 and body mass index (BMI) z-score of preschool children (PSC). São Paulo, 2009.")
 z-score at birth and body mass index (BMI) z-score of preschool children (PSC). São Paulo, 2009.")
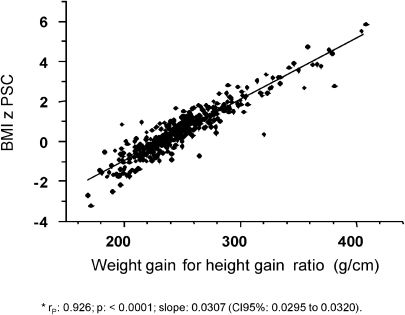
Figures 3 and 4 depict the high Pearson correlation coefficient (rP = 0.79) between the mean monthly gain of W and the BMI z-score of PSC. The ratio of mean W gain per H gain since birth (g/cm) and the BMI z-score of preschool children had a very high correlation coefficient (rP = 0.93). Both Pearson's coefficients were statistically significant, and their difference, 0.14, also was statistically significant (z = -7.8317, p<0.0001).
. São Paulo, 2009.")
 and preschool children (PSC) BMI z-score. São Paulo, 2009.")
The mean of the W gain per H gain evinced a low Pearson correlation coefficient (rP = 0.22) with birth length. The correlation was statistically significant (p<0.0001) but had no correlation with the birth weight.
DISCUSSIONUnderstanding the physical growth process and its determining factors in the first years of life remains an active research area in child health.11 This interest is largely due to the accumulated knowledge of the long-term repercussions of growth changes during childhood, such as physical and cognitive deficits and mortality.12 Physical growth is also internationally recognized as an indicator of nutritional status because adequate nutrition enables normal growth.13
In a prospective longitudinal study with 19,937 individuals from 20 locations in the United States, Steller et al14 examined the relationship between rapid weight gain in the first year of life and being overweight at seven years. Their findings indicated a positive relationship between the two variables. Each 100 g excess of weight gain since birth resulted in a 6% increase in the chance of being overweight at seven years of age. A cross-sectional study conducted with German school-aged children evaluated the trend of being overweight or obese in school-aged children. Newborns with a birth weight equal to or greater than 4 kg were 2.7 times more likely to be overweight by school age than low birth weight newborns.15
A 2003 cross-sectional study, conducted in Brazil by Drachler et al,16 used a sample of 2,687 children below the age of five to examine the relationship between socioeconomic conditions (among other factors) and overweight in infancy. They found a positive association between socioeconomic level and overweight. The chances of becoming overweight were also higher for children born heavier than expected for their gestational age and lower for children born lighter than expected for their gestational age. Another 2003 cross-sectional study, conducted in Brazil, used a sample of 1,076 individuals to examine the relationship between weight and length at birth, height and rate of infant growth, and weight excess and obesity in adolescents. Measurement data were collected at birth, 20 months, 40 months, 14 years, and 16 years. The findings indicated that birth weight and length at 20 and 40 months had positive linear relationships with overweight at a later age; however, these correlations did not reach statistical significance for obesity.17
The results of the present study differ from the studies mentioned above because we found no statistically significant relationships between birth weight and BMI z-score in preschool-aged children. Instead, the relationship observed was the ratio of the child's weight gain per height gain since birth.
The majority of the previous studies differ in their methodologies, thereby making comparisons difficult, especially in relation to the design of the studies, sample sizes, and age groups evaluated. In previous studies, birth weight was not included as a primary variable but was always given as a possible risk factor for the development of excess weight and obesity.
A possible explanation for our findings relates to the age group analyzed in the present study: early preschool age, children two and three years old. For this age group, birth weight may not yet correlate with an elevated BMI, as it would for older children. We were unable to find studies that examined birth weight and its relationship with the nutritional status of preschool-aged children. The majority of previous studies analyzed school-aged children and teenagers, and birth weight influences the nutritional status in these age groups.18,19
Based on the fact that changes in nutritional status arise from changes in diet and physical exercise patterns, the development of excess weight and obesity during preschool could result from inappropriate and nutritionally inadequate feeding practices during early life because little variation in physical activity would be expected at this age. According to Koletzko et al,20 a large weight gain during the first 24 months of life is associated with a lack of maternal breastfeeding and inadequate complementary feeding. Thus, such conditions may predispose children to weight excess later on.
The results obtained in this study are consistent with this idea because we observed no associations between birth weight and average monthly gains in weight and height until three years of age. There was also no correlation between the nutritional status of the children studied and birth weight or age in months.
On the other hand, our data indicate an increased correlation between BMI and mean monthly gain in the weight and height ratio, albeit with a much lower correlation coefficient than observed for the increase in height. Furthermore, a significant association was observed when the ratio of mean monthly gain in weight to average monthly gain in height was examined, and the slope indicates a progressively increasing direct relationship.
The correlation of higher BMI at preschool age with the ratio of W gain per cm gain in height confirms that a disproportionately larger weight gain when compared to the increase in height, if periodically assessed during the first two years of life, is probably a better indicator of risk for weight excess in preschool children than just total weight gain during the same time intervals.
The major limitation of this study was its cross sectional design, yet its results still suggest a need for further cohort studies that would prospectively follow up on the evolution of the ratio of weight gain per cm height gain, at least during the first two years of life.
In conclusion, regardless of weight and length at birth, the mean ratio of the weight gain per height growth in cm (from birth) evinced a very strong correlation with the BMI of preschool children. If prospective studies confirm these results, the use of this ratio in regions with high obesity prevalence could become a very useful tool as an indicator of overweight and obesity risk in children less than five years of age.
Grant sponsors:
This research was conducted with financial help from the Research Support Foundation of the State of Sao Paulo (Fundação de Amparo à Pesquisa do Estado de São Paulo – FAPESP), process no. 08/53142-9.