



The aim of this study was to report a single center experience of organ and tissue transplantation
INTRODUCTION:This is the first report of organ and tissue transplantation at the Hospital das Clínicas of the University of Sao Paulo Medical School.
METHODS:We collected data from each type of organ transplantation from 2002 to 2007. The data collected were patient characteristics and actuarial survival Kaplan-Meier curves at 30 days, one year, and five years
RESULTS:There were a total of 3,321 transplants at our institution and the 5-year survival curve ranged from 53% to 88%.
CONCLUSION:This report shows that solid organ and tissue transplants are feasible within the institution and allow us to expect that the quality of transplantation will improve in the future.
Transplantation has been an option for patients with end-stage organ disease and can provide a chance for survival. Our institution is one of the largest medical school hospitals in this country, with a relatively significant activity in complex procedures and transplants.1–5 The aim of this registry was to report the experience of transplantation at our institution for the last five years. It represents a unique data repository in an effort to help patients with untreated disease with conventional therapy.
PATIENTS AND METHODSData were collected from each organ and tissue transplantation carried out from 2002 to 2007. The following parameters were studied: the number of transplants, age of recipient, indications for transplantation, maintenance immunosuppression protocols [calcineurin inhibitor (cyclosporine or tacrolimus), cytostatic drugs, and the use of steroids], major complications, causes of death, and the survival curve for each organ and tissue.
For statistical analysis, all data were reported as median, minimum, and maximum values. Survival rates were calculated using the Kaplan-Meier method. All analyses were performed with SPSS statistical software, version 10.0 (SPSS Inc., Chicago, IL, USA).
RESULTSThe registry of transplantation at the Hospital das Clínicas of the University of Sao Paulo Medical School covers organ and tissue transplants from 2002 through 2007.
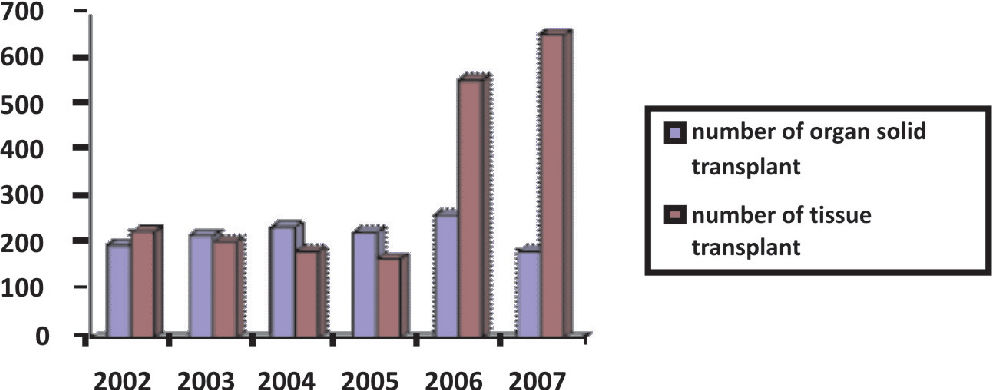
The total number of recipients who received transplants was 3,321 (Table 1). There were 1,288 and 2,033 transplants of solid organs and tissue, respectively (Figure 1). The age of the recipients ranged from 0.6 to 90 years (Table 2). The distribution of the solid organ transplants per year ranged from 187 to 265 transplants (Figure 1).
Number of transplant recipients at Hospital das Clínicas of the University of São Paulo Medical School (2002–2007)
| Organ | N |
|---|---|
| Heart | |
| - Pediatric | 32 |
| - Adult | 109 |
| Liver | |
| - Pediatric | 135 |
| - Adult | 204 |
| Pancreas-kidney | 37 |
| Lung | 56 |
| Kidney | 715 |
| - Adult | 665 |
| - Pediatric | 50 |
| Total | 1288 |
| Tissue | N |
| Bone marrow | |
| - Pediatric | 57 |
| - Adult | 728 |
| Skin | 81 |
| Bone | 1167 |
| Total | 2033 |
")
Thirty-two pediatric patients aged from 0.9 years to 13.8 years (median: 6.0 years) were submitted to heart transplantation. The indications of heart transplantation were dilated cardiomyopathy in 25 patients (78%) and congenital heart disease in seven patients (22%).
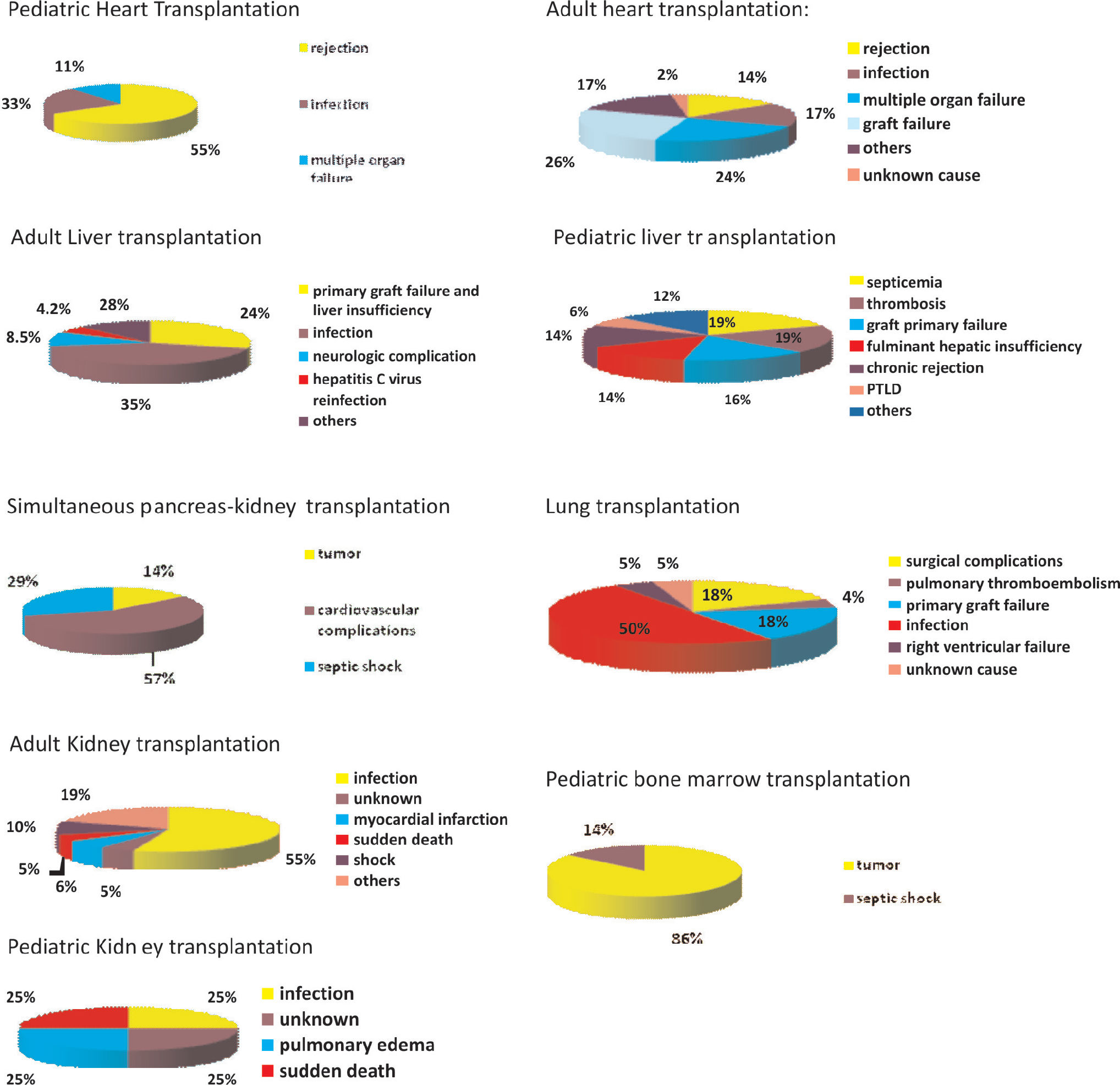
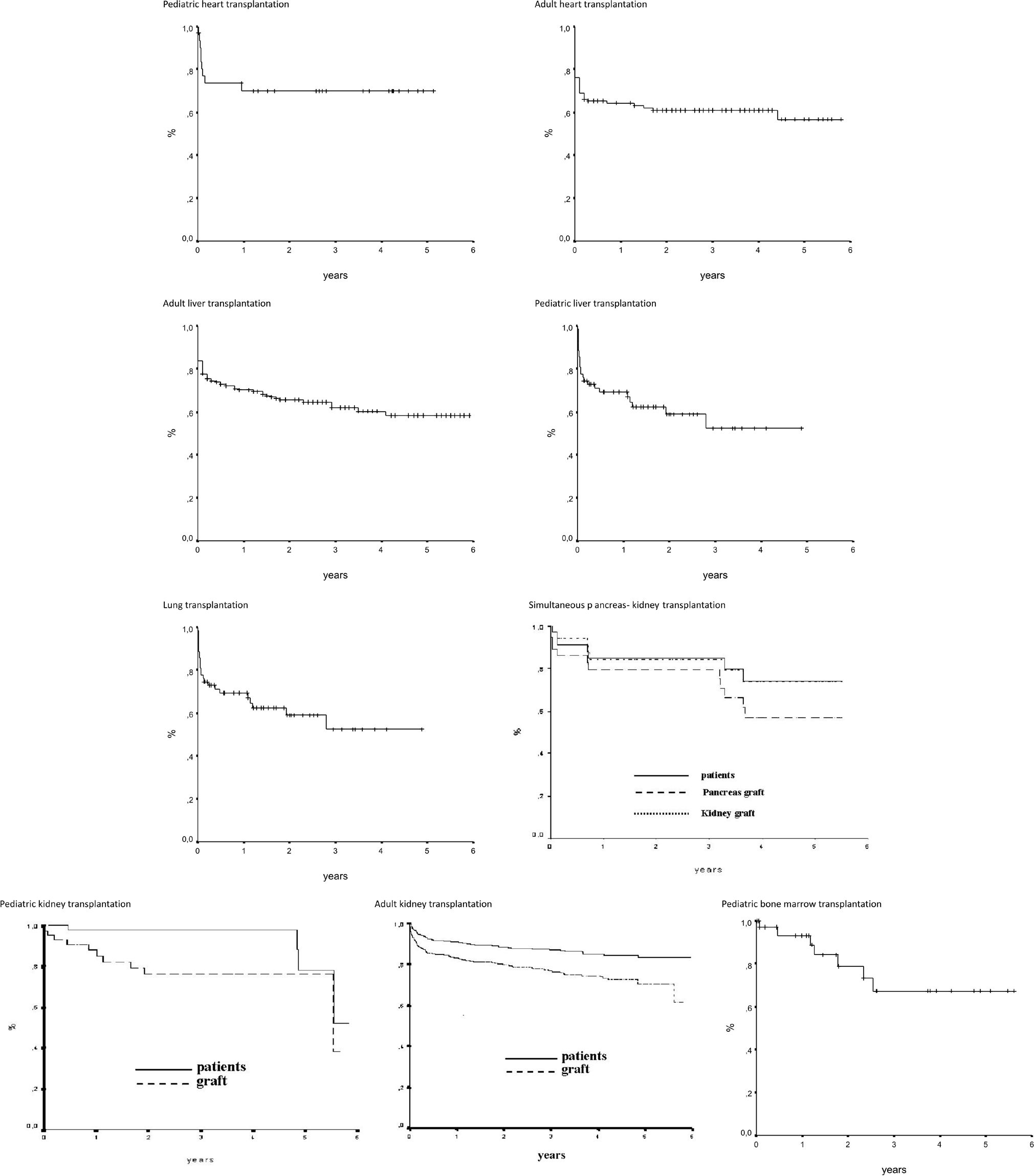
The immunosuppression used for induction therapy was methylprednisolone and thymoglobulin in all patients. The maintenance immunosuppression was the administration of calcineurin inhibitor in all patients, azathioprine in 4 patients (13%), and mychophenolate in 21 patients (65%). The major complications were 68 episodes of rejection (2.1 episodes per patient) and 61 episodes of infection (1.9 episodes per patient). No cases of tumor, diabetes mellitus, graft vascular disease, or renal failure (dialysis) were observed. Thirteen patients (40%) developed systemic arterial hypertension. Two re-transplantations were carried out. Nine (28%) patients died. The causes of mortality were rejection in five patients (55%), infection in three (33%), and multiple organ failure in one (11%) (Figure 2). The Kaplan-Meier curve was 80% at 30 days, 70% at 1 year, and 70% at 5 years (Figure 3).
Adult Heart Transplantation")
")
There were a total of 109 adult patients who were submitted to heart transplantation. The median age of recipients was 47 years. The median age of donors was 31 years. The immunosuppression for induction therapy was methylprednisolone in 103 patients (94.4%), mycophenolate in 58 patients (53.2%), azathioprine in 41 patients (37.6%), basiliximab in six patients (5.5%), and other drugs in seven (6.4%) patients. The maintenance immunosuppression protocol consisted of calcineurin inhibitor in 71 patients (96%), azathioprine in 28 (37.8%), mychophenolate in 42 (56.8%), and steroids in 54 (73%). There were 43 (39.4%) deaths. The causes of mortality were graft failure in 11 patients (26%), multiple organ failure in 10 (24%), infection in seven (17%), rejection in six (14%), other causes in seven (17%), and an unknown cause in two (2%) (Figure 2). The Kaplan-Meier was 76% at 30 days, 64% at one year, and 56% at five years (Figure 3).
Adult liver transplantationTwo hundred and four patients received 225 liver transplants (21 were re-transplants). The median age of recipients was 47 years (range, 14 to 70 years). The indications for liver transplantation are in table 3. Patients received immunosuppression with tacrolimus in 195 cases (96%) or cyclosporine in 9 (4%) and steroids, azathioprine in 6 (3%) or mycophenolate in 32 (16%). There were 71 deaths. The causes of mortality were infection in 25 patients (35%), primary graft dysfunction in 17 (24%), neurologic complication in six (8.5%), hepatitis C virus reinfection in 3 (4.2%), and other causes in 20 (28%) (Figure 2). The Kaplan-Meier overall survival was 83.8% at 30 days, 70.2% at one year, and 66.9% at five years (Figure 3).
Indications for adult liver transplantation
| Disease | N | % |
|---|---|---|
| Hepatitis C virus | 42 | 18.7 |
| Fulminant hepatitis | 42 | 18.7 |
| Hepatocarcinoma and cirrhosis | 42 | 18.7 |
| retransplantation | 21 | 9.3 |
| Autoimmune hepatitis | 17 | 7.5 |
| Hepatitis B virus | 16 | 7.1 |
| Cryptogenic cirrhosis | 13 | 5.7 |
| Alcohol | 12 | 5.3 |
| Primary biliary cirrhosis | 6 | 2.6 |
| Primary sclerosant cholangitis | 2 | 1.0 |
| Others | 12 | 5.3 |
| Total | 225 | 100 |
One hundred thirty five patients received liver transplants. The median age of recipients was 4 years (range, 7 months to 16 years). The indications for liver transplantation were biliary atresia in 75 patients (55%), alpha-1 antitrypsin deficiency in five (4%), fulminant hepatitis insufficiency in 13 (10%), and other indications in 42 (31%). The induction therapy was tacrolimus and steroids in 96 (71.1%) patients, cyclosporine and steroids in 20 (14.8%), and other drugs in 19 (14.1%). The maintenance immunosuppression was tacrolimus in 69 patients (80.2%), mycophenolate in 23 (26.7%), steroids in 64 (74.4%), and other treatments in 9 (10.4%). There were 49 deaths. The causes of mortality were septicemia in nine patients (19%), thrombosis in nine (19%), primary graft failure in eight (16%), fulminant hepatic insufficiency in seven (14%), chronic rejection in seven (14%), post-transplantation lymphoproliferative disease in three (6%), and other causes in four (12%) (Figure 2). The Kaplan-Meier survival curve was 84.4% at 30 days, 64.5 % at one year, and 61.8 % at five years (Figure 3).
Lung transplantationFifty-six patients received lung transplants. The median age was 47 years (range, 6 years to 67 years). There was only one child (six years old) in this group. The indications were: chronic obstructive pulmonary disease in 15 patients (27%), fibrosis in 15 (27%), bronchiectasis in 13 (23%), cystic fibrosis in eight (14%), and other indications in five (9%). The immunosuppression for induction therapy involved methylprednisolone in 56 patients (100%), basiliximab in 20 patients (36%), antithymocyte globulin in two (4%), and no other induction in 34 (58%). Immunosuppression was maintained using calcineurin inhibitor in 56 patients (100%), azathioprine in 25 (45%), mycophenolate in 27 (48%), and steroids in 56 (100%). There were 22 deaths. The causes of mortality were infection in 11 patients (52%), primary graft failure in four (18%), surgical complications in four (18%) patients (empyema, anastomosis dehiscence in two (8%), and one patient (4%) for each of the following conditions: hemoptysis and bronchovascular fistula and hemorrhage), right ventricular failure in one (4%), pulmonary thromboembolism in one (4%), and unknown cause in one (4%) (Figure 2). The Kaplan-Meier survival curve was 77.7% at 30 days, 70.0% at one year, and 53.3% at five years (Figure 3).
Simultaneous pancreas-kidney transplantationThirty-seven patients received pancreas kidney transplants. The median age of recipients was 36 years (range, 25 years to 51 years). The indications were type I diabetes with renal chronic failure in 32 (86.5%) patients, type I diabetes following kidney transplantation in three (8.1%) patients, and type I diabetes in two (5.4%) patients. The immunosuppression for induction therapy was: IL2R (daclizumab), tacrolimus, mycophenolate and steroids in 16 patients (43%); and antithymocyte horse globulin – thymoglobulin, tacrolimus, mycophenolate, and steroids in 21 (56.7%). The maintenance immunosuppression in all patients was tacrolimus, mycophenolate, and steroids. There were seven deaths. The causes of mortality were cardiovascular complications in four patients (57%), septic shock in two (29%), and tumor in one (14%) (Figure 2). The Kaplan-Meier overall recipient survival curve was 97.3% at 30 days, 84.9% at one year, and 74.2% at five years. The pancreatic graft survival curve was 97.3% at 30 days, 79.4% at one year, and 56.7% at five years; kidney graft survival was 97.3% at 30 days, 84.5% at one year, and 73.9% at five years (Figure 3).
Kidney transplantationA total of 715 patients aged from 3 to 78 years (median, 41.3 years) were submitted to kidney transplantation. The indications for pediatric and adult kidney transplantation are given in Tables 4 and 5, respectively. The most common indication was chronic glomerulonephritis in 140 patients (21%).
Indications for pediatric kidney transplantation
| Disease | N | % |
|---|---|---|
| Chronic obstructive pyelonephritis | 10 | 20 |
| Nephrotic syndrome | 8 | 16 |
| Chronic glomerulonephritis | 8 | 16 |
| Hemolytic uremic syndrome | 4 | 8 |
| Renal hypoplasia | 3 | 6 |
| Unknown renal insufficiency | 3 | 6 |
| Focal segmental glomerular sclerosis | 2 | 4 |
| Congenital defect | 2 | 4 |
| Reflux nephropathy | 2 | 4 |
| Others | 8 | 16 |
| Total | 50 | 100 |
Indications for adult kidney transplantation
| Disease | N | % |
|---|---|---|
| Chronic glomerulonephritis | 140 | 21 |
| Systemic arterial hypertension | 104 | 15.6 |
| Diabetes mellitus | 90 | 13.5 |
| Unknown renal insufficiency | 75 | 11.3 |
| Polycystic kidney disease | 24 | 3.6 |
| Nephrotic syndrome | 20 | 3 |
| Chronic Obstructive pyelonephritis | 18 | 2.7 |
| Lupic nephritis | 16 | 2.4 |
| Focal segmental glomerular sclerosis | 7 | 1.0 |
| Others | 171 | 25.9 |
| Total | 665 | 100 |
Pediatric kidney transplantation: 50 children received kidney transplants. The median age was 13 years (range, 3 to 17 years). The immunosuppression used for induction therapy in children was basiliximab in 14 patients (28%), daclizumab in 28 (56%), and antithymocyte globulin in six (12%). The maintenance immunosuppression was tacrolimus, mychophenolate, and steroids in 45 patients (90%); and cyclosporine, mycophenolate, and steroids in five (10%). Four patients died. The causes of death for the four were acute edema, sudden death, infection, and an unknown cause (Figure 2). The Kaplan-Meier graft survival curve was 95.9% at 30 days, 88.7% at one year, and 76.7% at five years. The patient survival curve was 100% at 30 days, 97.7% at one year, and 78.1% at five years (Figure 3).
Adult kidney transplantation: 665 adult patients were submitted to kidney transplantation. The median age was 45 years (range, 18 to 78 years). The induction therapy in adults was basiliximab in 306 (46%) patients, daclizumab in 162 (24.3%), antithymocyte globulin in 96 (14.4%), and OKT3 in 10 (1.5%) patients. The maintenance immunosuppression was tacrolimus, mychophenolate, and steroids in 497 patients (74.8%); cyclosporine, mycophenolate, and steroids in 84 (12.7%); cyclosporine, azathioprine and steroids in 20 (3%); cyclosporine, rapamycin, and steroids in 16 (2.4%); and other therapy in 48 (7.1%). Eighty patients died. The causes of mortality were septic shock in 44 patients (55%), myocardial infarction in five (6%), sudden death in four (5%), shock in eight (10%), unknown causes in four (5%), and other causes in 15 (19%) (Figure 2). The Kaplan-Meier graft survival curve was 92.9% at 30 days, 83.2% at one year, and 70.1% at five years (Figure 3). The patient survival curve was 96.6% at 30 days, 91.0% at one year, and 83.2% at five years (Figure 3).
Pediatric bone marrow transplantationThirty-four patients received autologous bone marrow transplants. The median age of recipients was 6.6 years. The indications were the following: neuroblastoma in 25 patients, Ewing sarcoma in three, non-Hodgkin lymphoma in three, meduloblastoma in two, and Wilms’ tumor in one. The immunosuppression for induction therapy was carboplatin (CBDCA), etoposide (ETO), and melphalan (MELFA) in 29 patients; bleomycin, etoposide, cytarabine, and melphalan (BEAM) in two; CBDCA/ETO in three; and cisplatin (CDDP), cyclophosphamide (CTX), and vincristine (VCR) in two. The number of deaths was seven. The causes of mortality were tumor in six patients (86%) and septic shock in one (Figure 2). The Kaplan-Meier survival curve was at 96.8% at 30 days, 93.1% at one year, and 67% at five years (Figure 3).
Five children with acute myeloid leukemia (AML) and 18 children with acute lymphocytic leukemia (ALL) underwent to allogeneic bone marrow transplantation.
Adult bone marrow transplantationA total of 728 patients underwent hematopoietic stem cell transplantation (HSCT). The indications for HSCT were multiple myeloma (173), non-Hodgkin lymphoma (169), acute myeloid leukemia (101), Hodgkin lymphoma (109), chronic myeloid leukemia (81), severe aplastic anemia (55), and acute lymphocytic leukemia (40). The indications are listed in Table 6.
Indications for adult hematopoietic stem cell transplantation
| Disease | N | % |
|---|---|---|
| Multiple Myeloma | 173 | 23.8 |
| Non-Hodgkin Lymphoma | 169 | 23.2 |
| Hodgkin Lymphoma | 109 | 14.9 |
| Acute Myeloid Leukemia | 101 | 13.9 |
| Chronic Myeloid Leukemia | 81 | 11.1 |
| Severe Aplastic Anemia | 55 | 7.5 |
| Acute Lymphocytic Leukemia | 40 | 5.6 |
| Total | 728 | 100 |
The following conditioning regimens were used for the different diseases:
- non-Hodgkin lymphoma patients: BEAM – BCNU (carmustine) 300 mg/m2 + etoposide (800 mg/ m2) + cytarabine (1600 mg/ m2) + melphalan (140 mg/ m2);
- multiple myeloma patients: busulfan (12 mg/kg) + melphalan (100 mg/ m2) for autologous transplantation; fludarabine (125 mg/ m2) + melphalan (180 mg/ m2) for allogeneic transplantation;
- Hodgkin lymphoma patients: MBV – melphalan (140 mg/ m2) + BCNU (carmustine; 300 mg/ m2) + VP-16 (etoposide; 2000 mg/ m2);
- acute myeloid leukemia patients and chronic myeloid leukemia patients: busulfan (16 mg/kg) + melphalan (140 mg/ m2);
- severe aplastic anemia patients: busulfan (4 mg/kg) + cyclophosphamide (200 mg/kg), or total body irradiation (300 rads) + cyclophosphamide (200 mg/kg);
- acute lymphocytic leukemia patients: busulfan (16 mg/ kg) + melphalan (140 mg/ m2), or total body irradiation (1200 rads) + cyclophosphamide (120 mg/kg);
The maintenance immunosuppression after allogeneic transplantation was cyclosporine A at a dose of 3 mg/kg/day (intravenous infusion), together with methotrexate at a dose of 15 mg/m2) on day +1 and a dose of 10 mg/ m2 on days +3, +6, and, +11 after HSCT.
Bone transplantationA total of 1167 patients received bone, ligament, or tendon transplants. The median age of recipients was 48 years (range, 2 to 90 years). The indications for transplantation were either odontologic (813 patients, 69.7%) or orthopedic (354 patients, 30.3%). Odontological indications of bone transplantation were mandibular and maxilar bone loss caused by tumors, trauma, and periodontal disease. Orthopedic indications were divided into the following groups: hip surgery (177, 50%), knee surgery (128, 36%), tumor surgery (35, 10%), and shoulder surgery (14, 4%). The main indication for hip surgery was revision hip arthoplasty with femoral or acetabular bone loss. Bone and ligament transplantation in knee surgery was used in revision knee arthoplasty, reconstruction of anterior cruciate ligament injury, (patellar graft, semitendinosus and gracilis graft), and severe trauma. The indications for the tumor group were benign lesions (unicameral and aneurismal bone cysts, non-osteogenic fibromas), and malignant tumors (Ewing sarcoma and osteosarcoma). Indications for shoulder surgery were repair of rotator cuff injuries and acromioclavicular dislocations using ligaments and rotator cuff grafts. Immunosuppression was not used for induction or maintenance therapy, since bone, ligament, and tendon transplantation, unlike transplantation of other solid organs, do not cause death in the event of graft failure. The main complications of bone transplantation were infection and immunogenic reaction against the graft. Of 35 patients in the tumor group, two (5.7%) developed infection, two (5.7%) had immunogenic reactions, three (8.6%) had allograft fractures that required revision and autologous bone grafts, and one (2.9%) had recurrence of the tumor in the leg that had received the transplantation, and the leg was therefore amputated.
Skin transplantationEighty-one patients aged 0.3 years to 78 years (median, 34 years) received skin transplants. The main use of this transplantation was for temporary skin coverage until an autogenous graft could be implanted. The indications for skin transplantation were large burns with few skin donor areas in 38 patients (46.9%), wound bed preparation in 28 (34.5%), hemodynamic instability in seven (8.6%), pyoderma gangrenosum in four (4.9%), aplasia cutis in two (2.4%), and giant congenital nevi in two (2.4%). After 3–5 days, the allogeneic skin was removed and the wound bed was evaluated. If there was sufficient granulation tissue then an autogenous graft was made; if the granulation tissue was not good, a new transplantation was performed. In this way, 22 patients received a re-transplantation for wound bed preparation. The mortality rate of the patients was 16.4%: 13 patients died, five in the group of hemodynamic instability and eight in the group of large burns with few donor skin sites.
COMMENTS AND DISCUSSIONThe total number of solid organ transplant procedures (38.7%) of all transplants remained unchanged during the period (range, 2002 to 2007). The number of tissue transplants increased during the last two years, especially bone transplants.
Immunosuppression: The most common combinations of therapies included calcineurin inhibitor and mycophenolate. A smaller percent of patients were taking a calcineurin inhibitor combined with azathioprine.
Outcomes: Overall survival at 30 days, one year, and five years shows that the results of our institution6–21 are compatible with previously reported data.22–26 Infection and rejection were the main causes of death in the majority of the organ transplants in our report. This indicates that these two complications remain a challenge for physicians who take care of organ transplant patients.
We will continue to update our experience in an attempt to describe what is presently occurring in organ transplantation in our institution.
CONCLUSIONThis is the initial registry report from our institution. It will help us define baseline data that will form the basis of comparison for our future reports. This report shows that solid organ and tissue transplantations are feasible within the institution and they allow us to expect that the quality of results will improve in the future.
The members of the Solid Organ and Tissue Transplantation Committee of Hospital das Clínicas of University of São Paulo Medical School were as follows: Estela Azeka, José Otavio Costa Auler Júnior, Paulo Manuel Pego Fernandes, Willian Carlos Nahas, Alfredo Inácio Fiorelli, Uenis Tannuri, Lílian Maria Cristofani, Marcelo Tadeu Caiero, Frederico Luiz Dulley, André de Oliveira Paggiaro, Telesforo Bacchella. José Otavio Costa Auler Jr. was also the clinical director of the Hospital das Clínicas of University of São Paulo Medical School.