



Cardiovascular diseases are the main cause of death in women and men in Brazil, but the trends for the death ratios for ischemic heart disease and stroke in women and men remain unknown.
METHOD:In this study, the trends for the death ratios among women and men who were over 30 years of age were analyzed from 1980 to 2005. Data were collected for both the Brazilian population and the metropolitan area of São Paulo. Estimates of the population size and data for mortality were then obtained from the Brazilian Institute of Geography and Statistics and the Ministry of Health. The risk for death was adjusted using a direct method.
RESULTS:Death rates due to cardiovascular disease, ischemic heart disease, and stroke have declined in both Brazil and the metropolitan region of São Paulo. A linear regression analysis revealed a similar trend for ischemic heart disease and demonstrated a male/female ratio of 1.653 ± 0.001 (r = 0.228; p = 0.262) in Brazil and 1.763 ± 0.008 (r = 0.863; p<0.001) in São Paulo. Comparisons between the slopes of the linear regressions showed an increased ischemic heart disease ratio in men/women in São Paulo in comparison to those in Brazil (p<0.0001). The linear regression showed an increasing trend for the male/female stroke ratio of 1.252 ± 0.004 (r = 0.776; p<0.0001) in Brazil and 1.331 ± 0.006 (r = 0.580; p = 0.002) in São Paulo. Comparisons between the regressions for the stroke ratio were similar for men/women in São Paulo compared to Brazil (p = 0.244).
CONCLUSION:We observed an increased trend in the ratio for ischemic heart disease death in men compared to women. Improvements in the control of risk factors and treatments for both men and women are mandatory to reduce the number of ischemic heart disease-related deaths in Brazil.
Cardiovascular diseases (CVDs) are the main cause of death in women and men in Brazil.1 The death rates associated with ischemic heart disease (IHD) and stroke are similar in men, but the rates of death due to stroke are higher in Brazilian women compared to death for IHD.2 However, there is a decreasing trend in the mortality associated with CVD in both women and men. Nevertheless, in the metropolitan area of São Paulo (MASP), the death rate related to IHD is greater than that associated with stroke in both women and men.3 Previous studies have reported conflicting results that demonstrate a slower decline in the death rate associated with IHD in women compared to men in developed countries.4-7 On the other hand, there is growing evidence of an increase in IHD in low- and middle-income countries8 and even less favorable decreases in the trends for IHD and stroke in Latin America.9 In addition, the rates for IHD and stroke death are very similar in these countries. Nevertheless, in Brazil, the trends for the death ratios associated with IHD and stroke in women and men remain unknown. The present study analyzed these trend ratios in Brazil and in the MASP.
MATERIALS AND METHODSThis study analyzed the death ratio of IHD to stroke in women and men in Brazil and in the MASP who were over 30 years of age from 1980 to 2005. Estimates for the population size and mortality data for IHD and stroke were obtained from the Brazilian Institute of Geography and Statistics (IBGE; www.ibge.gov.br) and the Ministry of Health (www.datasus.gov.br). Deaths that occurred between 1980 and 1995 were classified according to the ICD-9 presented at the 9th Review Conference of the International Classification of Diseases (ICD) in 1975, the standards of which were adopted by the 20th World Health Assembly. According to the ICD-9, the death codes for the population from 1980 to 1995 were as follows: from 410 to 414 codes for IHD and from 430 to 438 codes for stroke. The deaths that occurred between 1996 and 2006 were classified according to the ICD-10 codes: from 120 to 125 codes for IHD and from 160 to 169 codes for stroke. The risk for death was adjusted using a direct method according to the 1960 standard world population.9 The data for mortality data (per 100,000 inhabitants), the percentage variations of CVD deaths, the male/female (M/F) ratio for IHD, the male/female ratio for stroke, the IHD/stroke ratio in Brazil, and the IHD/stroke ratio in the MASP were analyzed between 1980 and 2005. A simple linear regression was employed to analyze the mortality ratio associated with IHD and stroke, and after the comparison of slopes of the regression lines were done. The Primer of Biostatistics software, version 4.02 was used for all statistical analyses.10
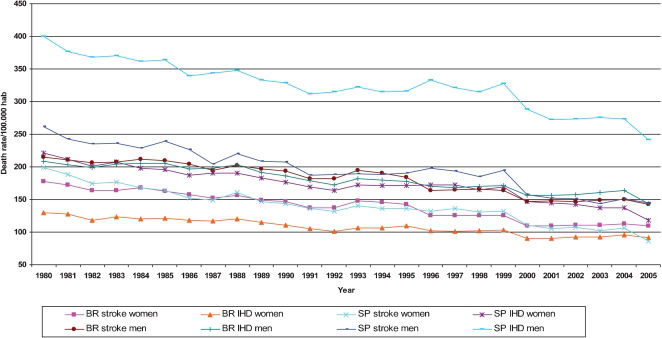
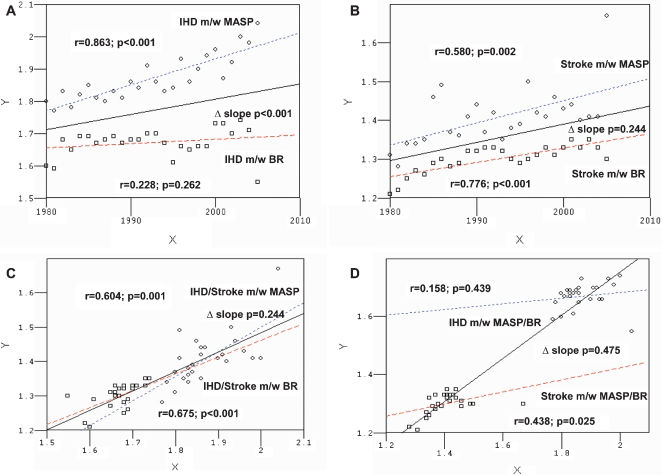
RESULTSThe death rates due to CVD, IHD, and stroke in Brazil and in the MASP are shown in Table 1 (Figure 1), and men/women ratios are shown in Table 2 (Figure 2). From 1980 to 2005 in Brazil, the death rate declined in women and men for CVD (-34.46% vs. -32.37%; p = 0.832), IHD (-29.23% vs. -31.32%; p = 0.915) and stroke (-38.30% vs. -33.38%; p = 0.674). In the MASP, the death rate also declined in women and men for CVD (-51.40% vs. -41.65%; p = 0.101), IHD (-46.59% vs. -39.49%; p = 0.392) and stroke (-56.75% vs. -44.96%; p = 0.170). The simple regression analysis and comparison of the slopes are presented in Figure 3. In Brazil, a simple linear regression analysis revealed an increasing trend for the male/female ratio for IHD, with an initial adjusted average coefficient of 1.653 ± 0.001 (r = 0.228; p = 0.262). An increasing trend was observed for this ratio in the MASP, with an initial adjusted average coefficient of 1.763 ± 0.008 (r = 0.863; p<0.001). Comparisons among the slopes of the regression lines revealed a significant increase in the male/female ratio for IHD in the MASP in comparison to Brazil (p<0.0001). In Brazil, a simple linear regression analysis showed a significant increasing trend for the male/female ratio for stroke, with an initial adjusted average coefficient of 1.252 ± 0.004 (r = 0.776; p<0.0001). In the MASP, an increasing trend was also observed for the male/female ratio for stroke, with an initial adjusted average coefficient of 1.331 ± 0.006 (r = 0.580; p = 0.002). Comparisons among the slopes of the regression lines revealed similar results for the male/female ratio for stroke in the MASP compared to Brazil (p = 0.244). In Brazil, the simple linear regression analysis showed a significant increasing trend for the male/female ratio for IHD versus the male/female ratio for stroke, with an initial adjusted average coefficient of 0.480 ± 0.492 (r = 0.604; p = 0.001). Similarly, the MASP showed an increasing trend for this ratio, with an initial adjusted average coefficient of 0.067 ± 0.717 (r = 0.675; p<0.0001). Comparisons among the slopes of the regression lines revealed similar results for the male/female ratio for IHD and the male/female ratio for stroke in the MASP compared to Brazil (p = 0.284). For the IHD M/F MASP/BR ratio, a simple linear regression analysis showed a similar trend, with an initial adjusted average coefficient of 1.486 ± 0.099 (r = 0.158; p = 0.439). The M/F MASP/BR ratio for stroke showed an increasing trend for this ratio, with an initial adjusted average coefficient of 1.006 ± 0.209 (r = 0.438; p = 0.025). Comparisons among the slopes of the regression lines revealed an increasing trend for the M/F MASP/BR ratio for IHD versus the M/F MASP/BR ratio for stroke in the MASP compared to Brazil (p<0.0001).
Death rates associated with cardiovascular disease (CVD), ischemic heart disease (IHD), and stroke.
| Year | Brazil | São Paulo | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CVD | CVD-men | CVD-women | IHD-men | IHD-women | Stroke-men | Stroke-women | CVD | CVD-men | CVD-women | IHD-men | IHD-women | Stroke-men | Stroke-women | |
| 1980 | 730.40 | 422.95 | 307.45 | 208.56 | 129.94 | 214.39 | 177.51 | 1082.56 | 661.70 | 420.86 | 399.72 | 221.56 | 261.98 | 199.30 |
| 1981 | 714.34 | 413.66 | 300.68 | 203.53 | 127.85 | 210.13 | 172.83 | 1018.50 | 618.34 | 400.15 | 376.12 | 212.21 | 242.22 | 187.95 |
| 1982 | 687.32 | 405.12 | 282.20 | 199.15 | 117.88 | 205.97 | 164.32 | 977.44 | 602.56 | 374.88 | 367.72 | 200.76 | 234.84 | 174.12 |
| 1983 | 698.84 | 411.55 | 287.28 | 204.39 | 123.75 | 207.17 | 163.54 | 989.98 | 606.55 | 383.43 | 370.18 | 207.07 | 236.36 | 176.36 |
| 1984 | 705.65 | 417.01 | 288.64 | 205.19 | 120.72 | 211.82 | 167.92 | 956.36 | 590.06 | 366.30 | 361.36 | 197.95 | 228.70 | 168.34 |
| 1985 | 699.41 | 415.59 | 283.82 | 205.59 | 121.17 | 209.99 | 162.65 | 962.20 | 602.80 | 359.40 | 363.49 | 196.07 | 239.32 | 163.32 |
| 1986 | 677.24 | 401.91 | 275.34 | 197.20 | 117.66 | 204.71 | 157.68 | 904.56 | 565.59 | 338.97 | 339.40 | 187.29 | 226.18 | 151.68 |
| 1987 | 662.35 | 392.53 | 269.82 | 197.40 | 117.16 | 195.13 | 152.66 | 887.69 | 547.88 | 339.81 | 343.23 | 190.44 | 204.65 | 149.37 |
| 1988 | 682.85 | 406.23 | 276.62 | 203.61 | 119.79 | 202.61 | 156.83 | 919.11 | 568.07 | 351.03 | 348.12 | 190.09 | 219.96 | 160.94 |
| 1989 | 652.37 | 388.48 | 263.89 | 191.37 | 114.55 | 197.11 | 149.34 | 870.01 | 540.56 | 329.45 | 332.57 | 182.73 | 207.99 | 146.72 |
| 1990 | 637.53 | 379.97 | 257.56 | 186.30 | 110.24 | 193.68 | 147.32 | 857.67 | 536.89 | 320.78 | 329.06 | 176.90 | 207.83 | 143.88 |
| 1991 | 603.25 | 360.55 | 242.71 | 178.26 | 105.79 | 182.29 | 136.91 | 803.84 | 498.45 | 305.39 | 311.22 | 169.06 | 187.23 | 136.33 |
| 1992 | 591.79 | 354.12 | 237.67 | 172.24 | 100.92 | 181.89 | 136.74 | 799.53 | 503.17 | 296.36 | 314.68 | 164.25 | 188.50 | 132.11 |
| 1993 | 630.60 | 376.21 | 254.39 | 181.54 | 106.74 | 194.67 | 147.65 | 825.53 | 512.42 | 313.12 | 322.54 | 172.63 | 189.87 | 140.49 |
| 1994 | 622.01 | 369.51 | 252.50 | 179.47 | 106.90 | 190.04 | 145.60 | 810.85 | 503.45 | 307.40 | 314.81 | 171.28 | 188.64 | 136.13 |
| 1995 | 613.05 | 361.12 | 251.93 | 177.41 | 109.82 | 183.71 | 142.10 | 814.78 | 506.68 | 308.10 | 316.11 | 171.55 | 190.56 | 136.55 |
| 1996 | 561.87 | 333.67 | 228.20 | 170.36 | 102.15 | 163.30 | 126.06 | 835.15 | 531.12 | 304.04 | 333.30 | 172.23 | 197.81 | 131.80 |
| 1997 | 559.16 | 332.26 | 226.90 | 167.88 | 101.27 | 164.37 | 125.63 | 822.06 | 514.35 | 307.72 | 320.98 | 171.97 | 193.37 | 135.75 |
| 1998 | 564.28 | 336.69 | 227.59 | 170.25 | 102.39 | 166.44 | 125.20 | 795.39 | 499.30 | 296.09 | 314.40 | 165.08 | 184.91 | 131.01 |
| 1999 | 562.48 | 334.59 | 227.88 | 170.85 | 102.70 | 163.74 | 125.19 | 823.55 | 522.45 | 301.10 | 328.09 | 168.72 | 194.36 | 132.38 |
| 2000 | 503.74 | 303.59 | 200.14 | 156.86 | 90.21 | 146.73 | 109.93 | 703.17 | 446.21 | 256.96 | 288.28 | 146.63 | 157.93 | 110.34 |
| 2001 | 505.18 | 304.79 | 200.39 | 156.41 | 90.33 | 148.39 | 110.06 | 674.65 | 424.06 | 250.59 | 272.19 | 145.12 | 151.87 | 105.47 |
| 2002 | 507.18 | 304.40 | 202.78 | 157.35 | 92.18 | 147.06 | 110.59 | 675.16 | 424.82 | 250.34 | 273.54 | 142.39 | 151.28 | 107.95 |
| 2003 | 513.11 | 310.15 | 202.97 | 160.97 | 92.29 | 149.18 | 110.67 | 658.74 | 419.43 | 239.30 | 276.00 | 137.55 | 143.44 | 101.75 |
| 2004 | 522.21 | 313.89 | 208.32 | 164.05 | 95.51 | 149.84 | 112.81 | 668.82 | 424.44 | 244.38 | 273.77 | 137.62 | 150.67 | 106.76 |
| 2005 | 487.54 | 286.05 | 201.49 | 143.23 | 91.96 | 142.82 | 109.53 | 590.60 | 386.08 | 204.52 | 241.88 | 118.33 | 144.20 | 86.19 |
| %V | -33.25 | -32.37 | -34.46 | -31.32 | -29.23 | -33.38 | -38.30 | -45.44 | -41.65 | -51.40 | -39.49 | -46.59 | -44.96 | -56.75 |
, ischemic heart disease (IHD), and stroke.")
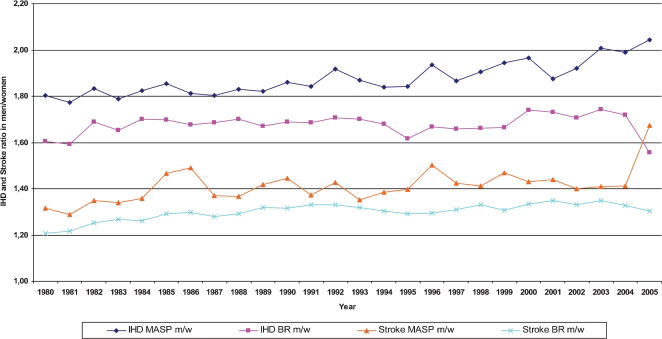
Ischemic heart disease (IHD) and stroke ratios in women (w) and men (m) ≥ 30 years of age in Brazil (BR) and in the metropolitan region of São Paulo (MASP) from 1980 to 2005.
| Year | IHD MASP M/F | IHD BR M/F | Stroke MASP M/F | Stroke BR M/F |
|---|---|---|---|---|
| 1980 | 1.80 | 1.61 | 1.31 | 1.21 |
| 1981 | 1.77 | 1.59 | 1.29 | 1.22 |
| 1982 | 1.83 | 1.69 | 1.35 | 1.25 |
| 1983 | 1.79 | 1.65 | 1.34 | 1.27 |
| 1984 | 1.83 | 1.70 | 1.36 | 1.26 |
| 1985 | 1.85 | 1.70 | 1.47 | 1.29 |
| 1986 | 1.81 | 1.68 | 1.49 | 1.30 |
| 1987 | 1.80 | 1.68 | 1.37 | 1.28 |
| 1988 | 1.83 | 1.70 | 1.37 | 1.29 |
| 1989 | 1.82 | 1.67 | 1.42 | 1.32 |
| 1990 | 1.86 | 1.69 | 1.44 | 1.31 |
| 1991 | 1.84 | 1.68 | 1.37 | 1.33 |
| 1992 | 1.92 | 1.71 | 1.43 | 1.33 |
| 1993 | 1.87 | 1.70 | 1.35 | 1.32 |
| 1994 | 1.84 | 1.68 | 1.39 | 1.31 |
| 1995 | 1.84 | 1.62 | 1.40 | 1.29 |
| 1996 | 1.94 | 1.67 | 1.50 | 1.30 |
| 1997 | 1.87 | 1.66 | 1.42 | 1.31 |
| 1998 | 1.90 | 1.66 | 1.41 | 1.33 |
| 1999 | 1.94 | 1.66 | 1.47 | 1.31 |
| 2000 | 1.97 | 1.74 | 1.43 | 1.33 |
| 2001 | 1.88 | 1.73 | 1.44 | 1.35 |
| 2002 | 1.92 | 1.71 | 1.40 | 1.33 |
| 2003 | 2.01 | 1.74 | 1.41 | 1.35 |
| 2004 | 1.99 | 1.72 | 1.41 | 1.33 |
| 2005 | 2.04 | 1.56 | 1.67 | 1.30 |
 and stroke ratios in women (w) and men (m) ≥ 30 years of age in Brazil (BR) and in the metropolitan region of São Paulo (MASP) from 1980 to 2005.")
 Ischemic heart disease (IHD) ratio in men (m) and women (w) in Brazil (BR) and in the metropolitan area of São Paulo (MASP); 3B) Stroke ratio in men (m) and women (w) in BR and in the MASP; 3C) IHD and stroke ratios in men (m) and women (w) in BR and in the MASP; 3D) IHD and stroke ratios in men (m) and women (w) in BR and in the MASP.")
3A) Ischemic heart disease (IHD) ratio in men (m) and women (w) in Brazil (BR) and in the metropolitan area of São Paulo (MASP); 3B) Stroke ratio in men (m) and women (w) in BR and in the MASP; 3C) IHD and stroke ratios in men (m) and women (w) in BR and in the MASP; 3D) IHD and stroke ratios in men (m) and women (w) in BR and in the MASP.
The results of the present study demonstrate an increased male/female ratio for IHD in the MASP but a steady ratio in Brazil. The male/female ratio for stroke increased in both Brazil and the MASP, and this pattern has been observed worldwide with a higher incidence and prevalence in men together with a worsened short-term prognosis.11 We observed a consistent increase in the IHD/stroke death ratio in both regions. We also observed an increase in the IHD/stroke death ratio in men compared to women, which likely reflected an epidemiologic transition in Brazil that resulted in a proportional increase in the number of IHD-related deaths. On the other hand, the increase in the male/female ratio for stroke can be explained by a greater reduction of stroke-related deaths in Brazilian women compared to IHD-related deaths even though stroke has remained the main cause of death.3 In the USA, stroke remains the second leading cause of death in women.12 The main risk factor for stroke is hypertension. Although the control of hypertension remains poor, it has demonstrated an improvement, which may be reflected by the decreased number of stroke-related deaths. Information and drug adherence has improved in Brazil due to increased access to cheaper antihypertensive drugs. Because stroke is the main cause of death in Brazilian women, a more effective control of hypertension may have an addition beneficial effect on the IHD/stroke and the male/female ratios. Nevertheless, similar results of hypertension control have not been observed for other risk factors, such as dyslipidemia, diabetes, smoking, and obesity.13 All of these risk factors are very important in the pathophysiology of atherosclerosis and in IHD. The control of risk factors has been shown to significantly reduce IHD-related deaths.14 Drugs that are used to treat dyslipidemia remain expensive for most of the Brazilian population.15 The control of diabetes has not improved,16 and obesity has increased in Brazil.17 There is a greater prevalence of risk factors for IHD in men, which may have influenced the diminished reduction of IHD-related deaths in men in the MASP.18,19 The limitations of the present study are related to the Brazilian mortality data, such as errors related to the diagnosis, the accuracy of the death certificates, deaths associated with unknown causes, and data entry errors. No validation studies for the data for the mortality rate are available in most states or cities in Brazil. An indirect indicator of the standard quality of the data is the number of death certificates that contain a diagnosis for the cause of death, such as symptoms, signs and poorly defined health conditions. These certificates are significant in the northeastern, northern, and central-western regions but are not significant in the southern and Southeastern regions of Brazil or in the MASP.
CONCLUSIONWe observed an increased trend for IHD deaths in men compared to women. Improvements in risk factor control and treatments in men and women are mandatory to reduce the number of IHD-related deaths in Brazil.