




Triple A syndrome is a multisystem disorder, with autosomal recessive inheritance, caused by mutations in the AAAS gene located on chromosome 12q13 which encodes the ALADIN protein. It is characterised by alacrima, achalasia, and adrenal insufficiency secondary to adrenocorticotropic hormone (ACTH) resistance.
We present the case of a 39-year-old woman who attended the Neurology clinic due to difficulty walking, which she had suffered since childhood, but with progressive worsening in recent years. Her family history included a sister with achalasia. Her own medical history consisted of bronchiectasis since childhood and surgery for pes cavus. She was on treatment with cholecalciferol 25,000 IU/month.
She reported difficulty in walking, limb weakness, dysphagia, diaphoresis without known cause, photophobia and alacrima since childhood. In the last 3–4 years, she had developed asthenia and hypotension.
Physical examination revealed a nasal voice and muscle atrophy. She weighed 57.2kg, her height was 163cm (BMI 21.5kg/m2) and her blood pressure was 120/86mmHg. She had hypoalgesia in “stocking-glove” pattern and deep tendon reflexes. Her visual acuity was 0.2 and she had optic atrophy together with severe dry conjunctivitis.
Electroneurogram showed decreased amplitudes in the median, ulnar, and tibial nerves. Muscle biopsy was nonspecific and brain MRI showed no abnormalities.
Laboratory tests were normal and included routine clinical biochemistry with complete blood count, lactic acid, creatine phosphokinase (CPK), organic acids in urine, amino acids in plasma and urine, acylcarnitines, phytanic acid and beta-cholestanol. The only significant result was basal blood glucose values at the lower limit of normal.
Given this complex neurological picture, a clinical exome study was requested, which detected a homozygous variant in the AAAS gene: c.1058T>C (p.Ile353Thr) (NM_015665). This variant is described in the databases consulted as a variant of uncertain clinical significance (rs765757844). The study was conducted in the patient's siblings, and it was confirmed that her sister, who was symptomatic (although less affected), was also a homozygous carrier. In her healthy brother, heterozygosity was detected. Taking these results into account and the fact that the bioinformatic analysis predicted that it would lead to disease, it was considered a pathogenic variant and the diagnosis of triple A syndrome was confirmed. The patient was referred to Endocrinology.
Blood tests showed: glucose 71mg/dl, total proteins 7.65g/dl, albumin 4.39g/dl, prealbumin 17.3mg/dl, creatinine 0.55mg/dl, total cholesterol 140mg/dl, triglycerides 97mg/dl, sodium 139mmol/l, potassium 4.2mmol/l, corrected calcium 9.1mg/dl, basal cortisol 8.4μg/dl, DHEAS 0.4μg/ml, ACTH 31pg/ml, folic acid 2.73ng/ml, vitamin B12 309pg/ml and TSH 1.62μIU/ml. The rest of the laboratory tests, including pituitary hormones and the renin-angiotensin-aldosterone axis, were normal.
The Synacthen test (ACTH 23.9pg/ml, basal cortisol 12.7 and at 30minutes 16.5μg/dl) diagnosed partial adrenal insufficiency, so the patient was started on replacement therapy with hydrocortisone, which improved the asthenia and hypotension.
Following diagnosis of achalasia with manometry, dietary modifications were introduced.
In addition to the aforementioned triad, there are cases of triple A with autonomic neuropathy (4 A syndrome) or with only two of the manifestations (2 A syndrome). The real incidence is unknown, due to undiagnosed cases and patients who die from adrenal crisis, generally during childhood.1
Alacrima seems to be the most common symptom (>90% of patients) and appears early, but it can go unnoticed until the signs of eye dryness (keratopathy, corneal ulcer) have developed.
In 70% of cases, the symptom that leads to the diagnosis is adrenal insufficiency. It generally manifests in childhood and more rarely in the teenage years. The mean age of onset in the series of patients evaluated by Grant was 1-8.3 years of age.2 As adrenal crises are the main cause of death in untreated patients with triple A syndrome and there have been reports of cases in their twenties at the time of onset, the diagnosis should not be ruled out just because the adrenal axis is normal on initial assessment.3
There is great variability in the degree of adrenal insufficiency in triple A syndrome; there have even been two cases, one diagnosed when the patient was in their thirties and the other in their fifties, with no sign of adrenal insufficiency at the time of diagnosis.4,5
To be considered adrenal insufficiency secondary to ACTH resistance, ACTH levels should be at least double the upper limit of normal. Normal ACTH values and late onset of hormone deficiency are other exceptions in this case. It could be hypothesised that this new mutation is associated with the progressive and late development of adrenal insufficiency by mechanisms other than ACTH resistance. However, due to the patient's cortisol levels being at the limit, a reassessment with an insulin tolerance test is pending.
In contrast, mineralocorticoid deficiency only occurs in 15% of cases, so most patients do not require treatment with fludrocortisone.6,7
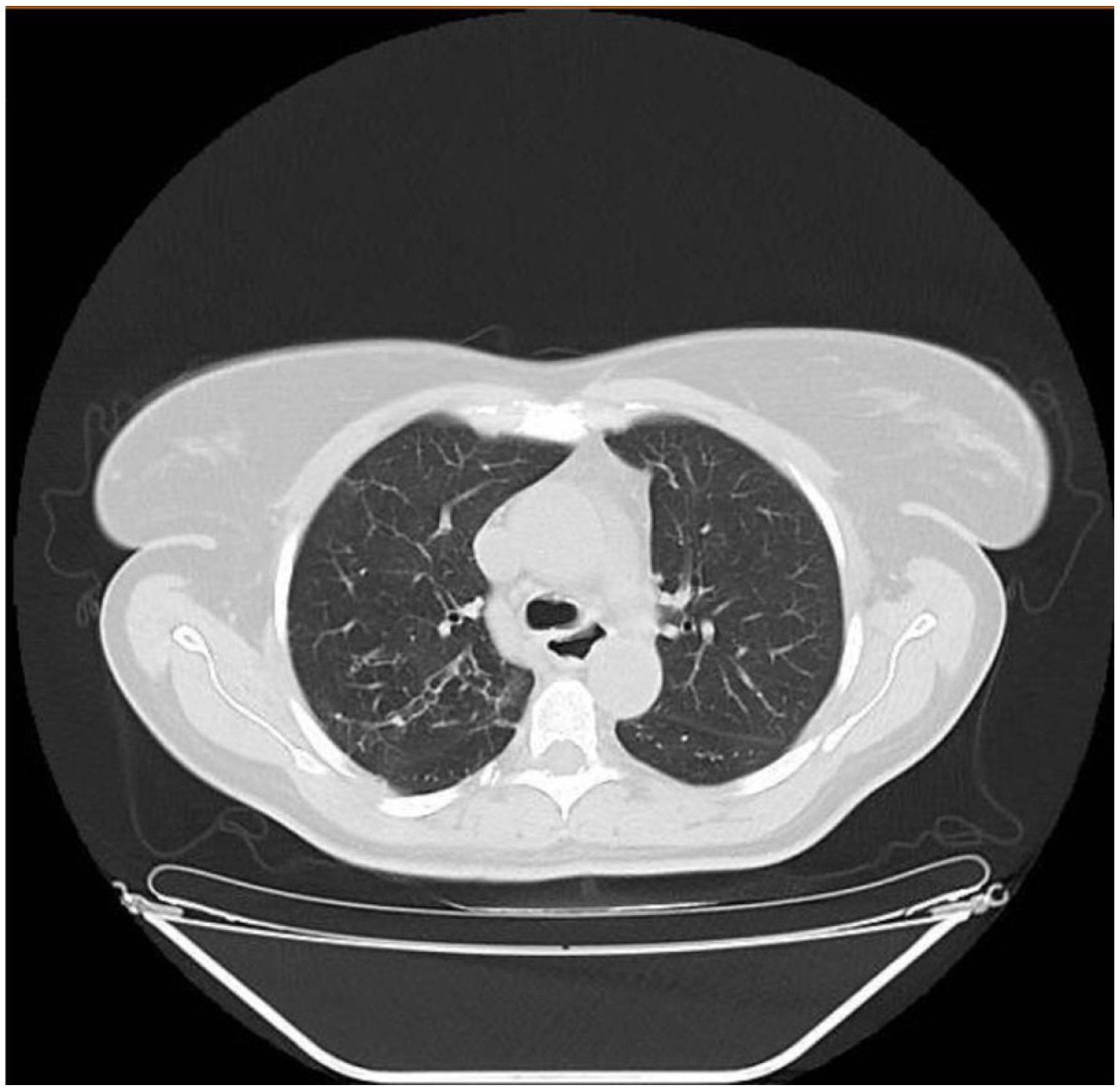
In children under 15 years of age, achalasia only occurs in 5% of cases. Our patient probably already had achalasia in childhood (compatible symptoms and bronchiectasis, Fig. 1). Nutritional assessment is vital as even those in whom myotomy is performed, post-intervention weight gain is lower than in patients with achalasia not associated with genetic syndromes.8

The age of onset of neurological symptoms is variable, but is generally in adulthood.9 The differential diagnosis includes adrenoleukodystrophy and multiple sclerosis.10 Once adrenal insufficiency has been treated, the most relevant prognostic factor is neurological symptoms (progressive). These include peripheral sensorimotor neuropathy, pyramidal syndrome, autonomic disorders, bulbar dysfunction, optic atrophy and ataxia.
Triple A syndrome is caused by pathological mutations in the AAAS, gene, which codes for the nucleoporin ALADIN. These mutations alter the transport of proteins necessary for DNA repair (aprataxin, DNA ligase I), which causes hypersensitivity to oxidative stress. This increase in oxidative stress in the nucleus seems to be responsible for clinical progression in triple A syndrome.
More than 75 mutations have been described in the AAAS gene, without finding any genotype-phenotype association. In fact, the phenotype is variable even among individuals with the same genotype.11 Therefore, although the genetic study is essential for diagnosis, it does not provide information on the patient's phenotype or prognosis. Some patients do not have mutations in this gene, so there may be other genes involved.
The case described is unique not only because it is the first associated with the c.1058T>C variant, but also because of the early neurological/gastrointestinal involvement and late onset of adrenal insufficiency with unknown pathophysiological mechanism.
FundingThis study has not received any type of funding.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: López Valverde ME, Rebollo Pérez MI, Martínez Fernández EM, Murillo Espejo E, Carrasco Salas P. Presentación clínica inusual y nueva mutación en un caso de síndrome triple A. Endocrinol Diabetes Nutr. 2022;69:382–384.
