




The widespread use of neck imaging methods has increased the number of diagnoses of asymptomatic thyroid nodules. Ultrasound studies in the population have found thyroid nodules in up to 67% of cases, most of them benign (93–97%).1–3 A major challenge is to determine whether they are malignant or benign without the need for surgery.1,2 Fine needle aspiration (FNA) is currently the gold standard for the diagnosis of thyroid nodules. However, approximately 15–20% of the results are histologically undefined and therefore not diagnostic, which means that they have to be operated on in order to rule out malignancy.1
Medical advances and the development of new non-invasive, more sensitive diagnostic methods now supplement the information provided by FNA. This is especially relevant for cytological samples classified as Bethesda category III (atypia of undetermined significance or follicular lesion of undetermined significance) and IV (follicular neoplasm or suspicious for a follicular neoplasm), in which it is difficult to rule out malignancy without surgery. High-resolution ultrasound allows malignancy to be detected in a high percentage of cases, but the chances of making an accurate diagnosis are still limited.3 Thyroid elastography is a new technique that estimates the viscoelastic properties of tissues using ultrasound, and is a promising test for ruling out thyroid malignancy and decreasing the number of surgical procedures when reasonable doubt has been cast by other tests.4
The objective of this study was to assess the value of elastography for distinguishing patients with Bethesda categories III or IV cytology who were candidates for surgery.
Since 2012, all patients at our center with a thyroid nodule have had thyroid elastography performed, and their data prospectively recorded in a database. From that database, patients with solitary thyroid nodules or dominant nodules within multinodular goiter were selected. Patients with prior thyroid surgery, FNA performed the month before elastography, and macrocalcifications in the nodule detected by ultrasonography were excluded. Patients with samples classified as Bethesda III and IV were selected for this study. Elastography was performed by an experienced radiologist after an ultrasound examination. The pressure applied during elastography is assessed by the quality factor (QF) on a scale of 0–100 random units. Only the images captured with QF>50, showing fewer artifacts, were assessed. There are five elastographic patterns5: (I) no or small area of stiffness; (II) area of stiffness <45%: the nodule is homogeneously deformed; (III) area of stiffness >45%: the center of the nodule is deformed less than the peripheral tissue; (IV) peripheral areas of stiffness and central area of elasticity: the whole nodule is deformed less than the surrounding tissue; and (V) area of stiffness occupying the whole nodule: the nodule and surrounding tissues are less deformed than the rest of the gland.
All patients underwent surgery, and nodules were classified as benign or malignant based on the histological study. Descriptive statistics were obtained, and Student's t and Chi-square tests were performed. Taking elastography patterns IV and V as malignant, sensitivity, specificity, positive predictive value, and negative predictive value were calculated.
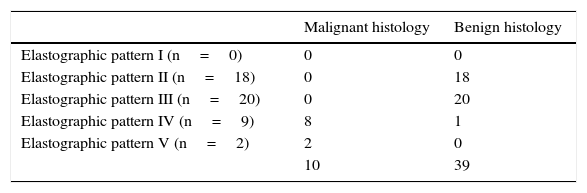
Forty-nine thyroid nodules classified as Bethesda categories III and IV were selected. Elastography showed pattern II in 18 cases (36.7%), pattern III in 20 (40.8%), pattern IV in 9 (18.4%), and pattern V in 2 (4.1%). As is shown in Table 1, 10 of the 49 nodules were histologically malignant (20.4%). All cases with elastographic pattern V were malignant. All cases but one with pattern IV were malignant. All cases with patterns II and III were benign (p<0.001). Elastography has a sensitivity of 91%, a specificity of 97%, a positive predictive value of 91%, and a negative predictive value of 100% for detecting malignancy. In 25 patients (51%), ultrasonography performed prior to elastography showed some characteristics which led to malignancy being suspected.3 All 10 patients with malignant histology had at least one such characteristic of malignancy. According to the ultrasonographic classification Thyroid Imaging Reporting and Data System (TI-RADS),6 24 patients (49%) had TI-RADS 2 or 3, none of them associated with malignancy; the elastographic pattern in these patients was II or III. In the remaining 25 cases (51%), the TI-RADS was 4. Of these, 16 (33%) were TI-RADS 4a: only two of them had an elastographic pattern higher than III, and one had an associated carcinoma. Of the remaining nine patients, six had TI-RADS 4b and three TI-RADS 4c, in all cases with elastographic patterns IV–V, and one was found to have a carcinoma in the final histology. The correlation between elastography and the TI-RADS was significant (p<0.001) for the association with malignancy.
Relationship between elastography and definitive histology of the thyroid nodule in nodules classified as Bethesda categories III or IV.
| Malignant histology | Benign histology | |
|---|---|---|
| Elastographic pattern I (n=0) | 0 | 0 |
| Elastographic pattern II (n=18) | 0 | 18 |
| Elastographic pattern III (n=20) | 0 | 20 |
| Elastographic pattern IV (n=9) | 8 | 1 |
| Elastographic pattern V (n=2) | 2 | 0 |
| 10 | 39 |
In thyroid nodules classified as Bethesda category III or IV, elastography allows us to determine which patients may be followed up with a high certainty that they are benign. Thus, elastographic patterns II and III allow for patient follow-up with ultrasonography and elastography. Cantisani et al. also showed, in a prospective study with 140 nodules7 the diagnostic value of elastography for thyroid nodules with indeterminate cytology. However, it should be noted that while quality studies such as those mentioned above suggest this predisposition, authors such as Lippolis et al.8 did not confirm the value of elastography for the preoperative selection of nodules with indeterminate cytology. In a meta-analysis, Bojunga et al. stated that elastography may be an alternative to cytology for patient selection.9 The systematic review and meta-analysis conducted by Remonti et al. added that the combination of different ultrasonographic characteristics seems to increase the ability of elastography to detect malignant nodules.10 Our data support the importance of correlating elastography with ultrasound in these patients. Thus, as Trimboli et al.11 observed in a prospective study, the grouping of ultrasound characteristics in the TI-RADS classification combined with elastography increases the sensitivity for detecting malignancy.
To conclude, based on our results, it may be stated that thyroid elastography is currently a diagnostic tool that supports ultrasonography in patients with Bethesda III or IV cytologies, so helping in the selection of candidates for surgery.
Please cite this article as: Ríos A, Rodríguez JM, Cepero A, Hernandez AM. Utilidad de la elastografía en los nódulos tiroideos con citología indeterminada o sospechosa de malignidad. Endocrinol Diabetes Nutr. 2017;64:180–182.
