




The tuberculosis surveillance system in the Balearic Islands was assessed from 2005 to 2007. Applying the capture–recapture method the completeness of this system was evaluated to be 58.4%. When a new electronic recorded data was included in Primary Health Care, up to 66.5% was obtained. This new source of data increased the detected cases of pulmonary tuberculosis from 572 to 681. As a result, the estimated annual incidence rate increases from 18.9 cases/105 to 22.6 cases/105 [95% CI, 20.9–24.3], similar to figures issued by WHO.
Evaluamos el sistema de vigilancia de tuberculosis en las islas Baleares desde 2005 a 2007. Aplicando el método captura-recaptura cuantificamos la exhaustividad del sistema en 58.4%. Incluyendo nuevos datos electrónicos registrados en Atención Primaria obtenemos un incremento hasta 66.5%. Ésta nueva fuente de datos incrementa los casos detectados de tuberculosis pulmonar desde 572 a 681. Como resultado, la incidencia anual estimada incrementa desde 18.9 casos/105 hasta 22.6 casos/105 [IC 95%, 20.9–24.3], similar a los cálculos de la OMS.
A good tuberculosis (TB) epidemiological surveillance system is essential to control the disease. The reported incidence of TB in Spain and in the Balearic Islands was, in the period 2005–2007, 18/105 cases, though WHO and some medical societies have estimated a highest incidence rate.1 For all these reasons we found it necessary to evaluate the TB-surveillance in the Balearic Islands focussing on its completeness.2
The TB-surveillance in the Balearic Islands mainly uses two sources of information:
- 1.
Passive surveillance activity, based on the notifications of mandatory reporting of incident cases (MND) by the clinicians when they suspect a case of TB.
- 2.
Active surveillance activity, searching TB coded diagnoses from hospital discharge recording and Mycobacterium cultures (HOSP).
In the period 2005–2007, 80% of TB cases were detected through the passive system from hospitals and primary care. The remaining 20% of TB cases were identified through the active surveillance system.
Since 2005 all relevant clinical data in public primary health care facilities (PHC) is electronically registered, constituting a potential source for surveillance.3 We think that the PHC electronic database may be useful in TB surveillance to detect unreported cases. The main objective of this study is to estimate the completeness of the TB-surveillance in the Balearic Islands in the period 2005–2007. Secondary objectives are to evaluate whether electronic information from the primary health care may be a useful source of information for active surveillance of TB and to evaluate whether completeness of the surveillance is different by pulmonary or extra-pulmonary TB.
Materials and methods- (a)
Design: retrospective study on the cohort of incident new TB cases recorded by the TB-surveillance in the Balearic Islands in the period 2005–2007. The variables included in the analysis were: type of TB, source of data, year of TB onset and personal identification data (name, gender, birth date).
- (b)
TB case definition: possible: clinical and/or radiological findings and medical indication for complete treatment; probable: positive smear or PCR; confirmed: positive culture isolation. All registers use the criteria defined by the national TB surveillance protocol.
- (c)
Case classification: the cases were stratified by type of TB, pulmonary and extra-pulmonary. When a case had both it was classified as a pulmonary case.
- (d)
Data sources: Passive surveillance from the mandatory notifiable diseases system (MND). Active surveillance in hospital records, through the records of hospital diagnoses at discharge and microbiological isolations (HOSP) and electronic clinical registries of primary health care (PHC).
- (e)
Linking: the three databases (MND, HOSP, and PHC) were manually linked using personal identification data (name, gender, birthdates) of the cases and ensuring confidentiality.
- (f)
Methodology: Capture–recapture method (C–R) to estimate the total number of expected cases making an approach of those not observed by any source.4,5 Log-lineal models were building to select the most compatible one.6 To obtain the log-linear models the Epidat 3.1 statistical package and the STATA 9.0 program were used. The statistical significance was set at p<0.05.
- (g)
Definitions: sensitivity of a source is the simple percentage ratio between observed and expected cases. Completeness of the system is an indicator of the system's detection capacity. Therefore, it fully estimates the sensitivity of each source and the completeness of the system as a whole.
This study was approved by the Ethics Committee of Research of the Balearic Islands (CEI-IB), as part of an overall assessment of TB-ESS.
Results- (1)
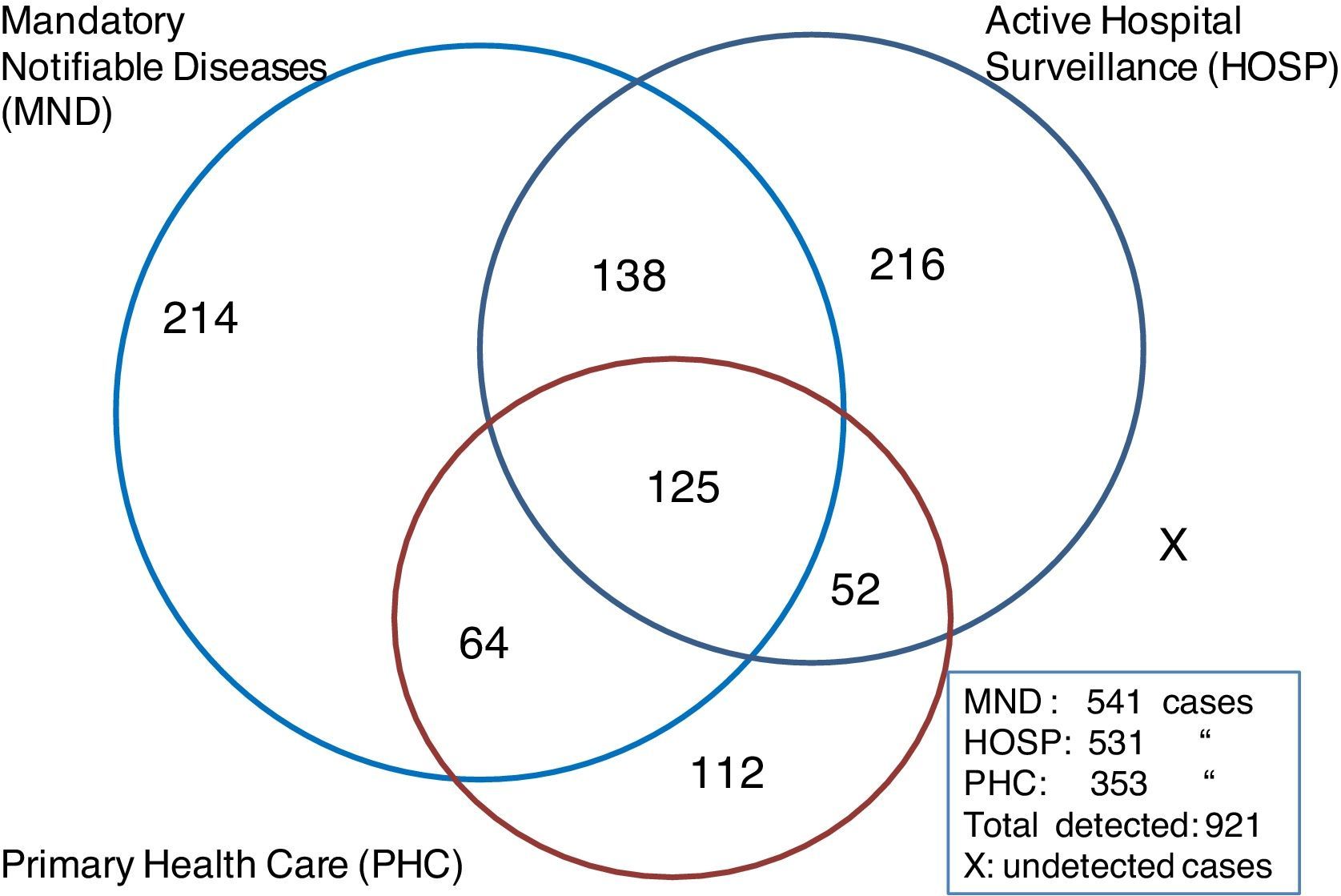
Global completeness of TB-Epidemiological Surveillance System. The number of reported cases to the MND was 541; the HOSP database collected 531 cases and the PHC database 353. The number of cases recorded in the 3 sources was 125, 254 in two of them and 542 in only one source. The overall number of cases detected was 921 (Fig. 1). Using the 3 database sources for the C–R method, the log-linear model selected as the best fitting to our data (that with the lowest BIC value) was the 7th hypothesis shown in Table 1 that includes interactions between MND–HOSP and MND–PHC. According to that, the global number of TB cases undetected by the system (X) was 465 and the overall number of cases (N) 1386 (95%CI 1216–1556). With these figures the exhaustivity of the TB-surveillance would have been 58.4%. With the use of the new PHC information source we found 109 previously undetected cases of pulmonary TB and 3 extra-pulmonary TB. Thus, the total underreported cases increased from 268 to 380 and the total number of cases to 921. When the PHC new database was included the exhaustivity increased to 66.5%, 8.1% above the previous results.
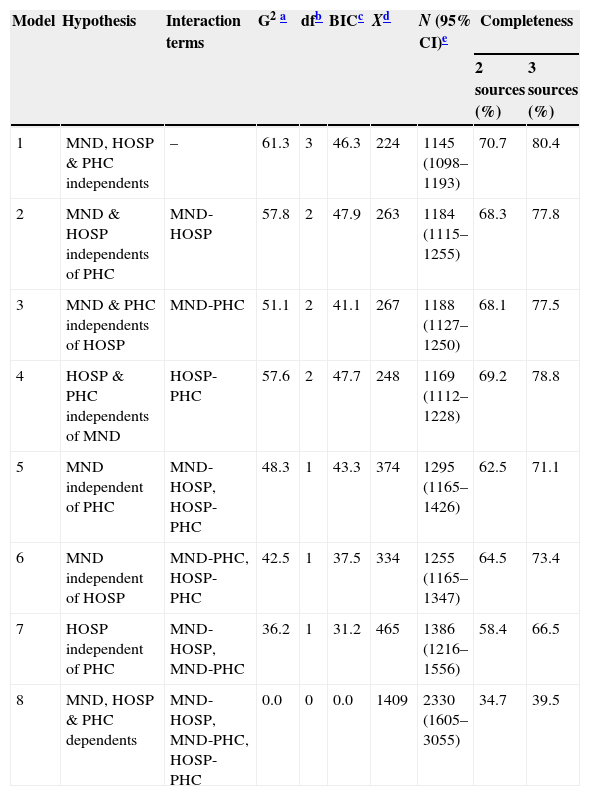
Table 1.Log-linear models for global tuberculosis cases, 2005–2007.
Model Hypothesis Interaction terms G2a dfb BICc Xd N (95% CI)e Completeness 2 sources (%) 3 sources (%) 1 MND, HOSP & PHC independents – 61.3 3 46.3 224 1145 (1098–1193) 70.7 80.4 2 MND & HOSP independents of PHC MND-HOSP 57.8 2 47.9 263 1184 (1115–1255) 68.3 77.8 3 MND & PHC independents of HOSP MND-PHC 51.1 2 41.1 267 1188 (1127–1250) 68.1 77.5 4 HOSP & PHC independents of MND HOSP-PHC 57.6 2 47.7 248 1169 (1112–1228) 69.2 78.8 5 MND independent of PHC MND-HOSP, HOSP-PHC 48.3 1 43.3 374 1295 (1165–1426) 62.5 71.1 6 MND independent of HOSP MND-PHC, HOSP-PHC 42.5 1 37.5 334 1255 (1165–1347) 64.5 73.4 7 HOSP independent of PHC MND-HOSP, MND-PHC 36.2 1 31.2 465 1386 (1216–1556) 58.4 66.5 8 MND, HOSP & PHC dependents MND-HOSP, MND-PHC, HOSP-PHC 0.0 0 0.0 1409 2330 (1605–3055) 34.7 39.5 Sources: Mandatory Notifiable Diseases (MND); active search through the Hospital records (HOSP); Primary Health Care electronic medical records (PHC). - (2)
Completeness of TB-Epidemiological Surveillance for Pulmonary Tuberculosis. Four hundred and three cases were reported to the MND, – 80 from Eivissa (20%) and 26 from Menorca (6.5%) – the HOSP database collected 388 cases and the PHC database 332. The number of cases recorded in the 3 sources was 121, 200 in two of them and 360 in only one source. The overall number of cases detected was 681. The log-linear model best fitting our results indicates that the system failed to detect 363 cases. Thus, the overall number of estimated cases was 1044 (95%CI 893–1195).
- (3)
Completeness of TB-Epidemiological Surveillance for Extra-pulmonary TB.One hundred and thirty eight cases reported to the MND – 22 from Eivissa (20%) and 2 from Menorca (1.8%) – the HOSP database collected 143 cases and the PHC database 21. The number of cases recorded in the 3 sources was 4, 54 in two of them and 182 in only one source. The overall number of cases detected was 240. Finally, the log-linear model selected indicates that the total number of cases of extra-pulmonary TB in the three years was estimated in 450 and, according to these results, the TB-surveillance could have failed to detect 210 cases (95%CI, 361–540). Thus, the TB-surveillance system would have attained a completeness of 52.7%, whereas adding the information source of PHC the overall completeness would have been 53.3% (95%CI, 44.4–66.5).

Completeness of TB-surveillance: The estimated cases via the Capture–Recapture method provide estimated incidence rates that nearly double those previously detected by the TB-surveillance.7 Completeness when PHC added: PHC database has the potential of increase completeness of the TB-surveillance by around 10% (66.5%, while only 58.4% without PHC), showing that it can be an important component in active TB surveillance, with a much higher magnitude for pulmonary TB, which is the one of greater concern in public health.
Differences between pulmonary-TB and extrapulmonary-TB: According to our results, the completeness is much higher for pulmonary TB than for extra-pulmonary TB. The reason could be that patients with extra-pulmonary TB are more frequently treated in the hospital and their registered data in PHC is not as complete as in HOSP.
The potential impact of these results on TB control in the Balearic Islands: using data from PHC improves the completeness of identification of TB cases and may therefore provide a more accurate representation of TB incidence. Thus, by using this new source the detected cases of pulmonary TB increased from 572 to 681, which is 37 more cases per year and an increase of the annual incidence rate from 18.9 cases/105 inhabitants to 22.6 cases/105 [95%CI, 20.9–24.3], quite similar to that calculated following the estimation method recommended by the WHO8 (22.3 cases/105). Our findings provide further evidence that in the Balearic Islands the real incidence rate of TB is higher than that calculated with the TB-surveillance data in that period of time.
Since the C–R method's purpose is to evaluate the surveillance system and each one of its components, it is not useful to identify the missing cases.
A limitation of the study was that we could not obtain the records of hospital diagnoses at discharge of any private hospital either that of public hospitals of the minor islands. Nevertheless, as we obtained the microbiological records of these hospitals as well as the mandatory notifications from its doctors and the primary care clinical records and that, united to the fact that the average of cases detected from private hospitals is small (around 5%) we thing that this limitation is not a major problem. The availability of primary health care diagnostic information via centralized computer records has proven to be useful for the active surveillance of TB. With that information the increase in the completeness for pulmonary TB is clear, but not so much for extra-pulmonary TB. Computer technologies, currently available to the Public Health Department, represent a good opportunity to improve the TB-surveillance. The possibility of crossing data from more sources of information (primary care, laboratory isolates, prescriptions of specific drugs, etc.) can help to obtain a more accurate assessment of the incidence rate in the community.9
In view of these results we recommend the following:
- (1)
Regularly and systematically include the use of Primary Health Care electronic information to improve the TB-epidemiological surveillance system completeness.
- (2)
Regularly assess the TB-surveillance with methods such as the capture–recapture10 in order to improve the system.
The authors declare no conflict of interest.
We wish to thank to Àngels Pujol-Buades, Amador Ruiz-Torrejón and Magdalena Esteva-Cantó for their help in obtaining all the required data. We would acknowledge to Camelia Savulescu and Dionisio J. Herrera-Guibert for all their help during the research and in the moment of presenting the preliminary data of this study as a communication in the ESCAIDE-conference 2009.

