




Indonesia is a developing country and most breast cancer patients present with terminal conditions, including discomfort. Comfort is a crucial component of nursing in palliative care, especially in breast cancer patients. However, this condition is difficult to assess and therefore assign as a diagnosis. Some comfort assessment tools have been developed in other countries are found not appropriate for an Indonesian context. This study is a sequence of prior qualitative research regarding a comfort assessment tool to be developed in Indonesia. This study piloted the comfort assessment tool in 55 patients with breast cancer to test if it is valid, reliable, and easy to use. This cross-sectional study was conducted at an Army hospital in Jakarta, Indonesia. The Comfort Assessment Breast Cancer Instrument measured many aspect of the patient comfort level including physical, psycho-social, cultural-spiritual, finance, and environmental comfort using a Likert scale from 1-4 and 34 items. Data were processed using statistical software. The face validity test yielded coefficient a of 0.299-0.691, while the reliability test produced a reasonably good result as well (a = 0.912). Therefore this measure should be further assessed by an expert panel and including construct validity.
The number of breast cancer patient who are in advanced stage at the time of diagnosis is high in Indonesia. According to GLOBOCAN (IARC), breast cancer was the most common cancer in 2012 with incidence of 43.4% and a mortality rate of 12.9%1. This high number of patients with advanced breast cancer in Indonesia also related to the region's culture and values. Indonesian people choose to try to treat the condition themselves by using traditional therapy2. They do not visit healthcare facilities unless that treatment or alternative therapy fails, so the cancer diagnosis is not made until the cancer is already in an advanced stage. Moreover, financial problem is one of some factors for breast cancer patients in Indonesia that makes a lateness of diagnosis and it affects the delay of treatment3. Around 60% of breast cancer patients admitted to Dharmais Cancer Hospital in Indonesia had an advanced stage of cancer4.
Comfort is an important aspect should be a component of all cancer patients’ palliative care, including breast cancer patients. Generally, cancer patients and their families experience comfort disruption, while the nurses have also reported difficulty in establishing its diagnosis since there is currently no instrument of comfort assessment that is suitable for cancer patients in Indonesia.
Some indicators of physical discomfort can be observed and measured, and these variables are not only physical, but also psychological. Therefore, discomfort variables including to a latent variable group that requires special technique to ensure its identification. Several studies have described instruments designed comfort and the effectiveness of palliative care, including the Problems and Needs in Palliative Care Questionnaire (PNPC) which was developed by Osse in the Netherlands. Kolcaba proposed an instrument to measure general comfort, as well as patient comfort levels in a perioperative environment, during radiation therapy, and in hospice care. Eton et al created a measurement instrument to examine the quality of life in breast cancer patients in the United States5,6. Other studies to devise a holistic comfort assessment of cancer patients were conducted in developed countries6,7. The results of a critical analysis of reliability test of the available assessment instrument for cancer patients showed that 19.4% had good validity but none could be classified as excellent8. The factor that most affected this invalidity was the diversity of culture and economic level. In Indonesia, palliative care implementation is influenced by economic and cultural differences. Based on Effendy's study9, she found that 70%-80% cancer patients in Indonesia had a financial problem and it affects physical problem that they experienced. Therefore, further research is needed to examine and improve an instrument to assess patient comfort, which should be adapted to the culture and socio-economy of the place where it will be used.
Instruments that have been developed in other areas of the world currently are not appropriate for assessing the comfort levels of cancer patient in Indonesia, country with a large number of people and a wide range of diversity in culture and socio-economic. The wide scope of existing instruments make the identification of an appropriate instrument for outcome assessment in palliative care become difficult10. Re-examination to validity and reliability for comfort instruments that have been frequently used in past research regarding breast cancer patients is a mus due to the diversity of population target's background. As Eton et al.6 did for Functional Assesment of Cancer Therapy Breast (FACT-B), they re-examine the data from past research to determine distribution and anchor-based estimates of minimally important differences. Therefore, it can be used in combination with other measures of efficacy to show meaningful benefit and provide a basis for sample size in clinical trials5.
MethodThe sample size needed to be at least 30 to ensure both validity and realiability. We collected data from 55 patients. This instrument measures breast cancer patient's comfort variable and was named The Comfort Assessment Breast Cancer Instrument (CABCI) which measures 5 comfort dimensions: physical, psycho-spiritual, socio-cultural, finance, and environmental. Sampling based on non-probability sampling with purposive sampling method.
The population in this research included cancer patients with palliative condition who were both outpatients and inpatients, and met the following inclusion criteria:
- A.
Adult patient (at least 18 years or more)
- B.
Able to take part in this research
- C.
Eastern Cooperative Oncology Group (ECOG) performance status ≤ 3.
- D.
Consciousness level: compos mentis
- E.
Stable hemodynamic status
- F.
Able to communicate in and understand Bahasa Indonesia
- G.
Diagnosed with stage II and III cancer
- H.
Currently receiving radiotherapy or chemotherapy.
The exclusion criteria was having any cognitive impairment due to the metastasis to the central nervous system.
This study is the first phase of research. It is used to measure validity and realiability testing to produce a tested and valid instrument of comfort assessment. The first phase was intended to define the instrument construct through implemented explorative research that involved both literature study and in-depth interview with cancer patient. The results of literature study identified several instruments of comfort measurement including Osse's PNPC Questionnaire, the Hospice Comfort Questionnaire which was created by Kolcaba, and the Functional Assesment of Cancer Therapy Breast (FACT-B). Next, these instruments were analyzed its compatibility with cancer patients in Indonesia by interviewing cancer patients and conducting a focus group discussion with nurses in Indonesia. Further, face validity or validity of display would be implemented on 55 cancer patients to determine the respondent's understanding on filling out a questionnaire regarding comfort level with Likert scale ranging 1-4. The analysis technique used in this activity were validity and realiability, which were assessed using computer software.
The data collecting began with a research proposal submitted to the Ethical Committee of Ethics Faculty of Nursing Universitas Indonesia and hospital which are research locations. After met the administrative requirements, the researcher began to collect the data and was assisted with two data collectors with educational background in nursing. These data collectors were responsible for selecting patients who met the inclusion criteria, collecting their demoghraphic data, and helping to develop the measurement instrument. The researcher train the data collectors for two days before data collection began, so that the data collectors would understand the requirements. Then, both of the data collectors and the researcher became acquainted with the patients and provided them with an explanation regaarding the study aims, benefits, an results. have a same perception. Researcher or data collector be aqcuainted to patients and give an expalanation related to aims, benefits, and results were would be obtained after study. The explanation about resignation right and right to keep receive a full service from hospital eventhough they resign. If patient have agree so that patient was asked to fill the agremeent form. After receive the agreement, data collectors record respondent's demography continued research instrument filling, and sampling.
After the data were collected, the second step was to check the received data, which then had to be coded to protect the participants’ anonymity. The third process was entering the quantitative data into a statistical software program. The forth activity was a reliability and validity analysis of each item. Items that had only minor validity were deleted. The number of items that were analyzed was 76 with the following breakdown: 15 physical comfort items, 27 psycho-spiritual items, 27 sociocultural items, and 7 environmental items.
For this study, the researcher conducted interviews with cancer patients and identified some dimensions that had not been included in the items of the assessment instruments of comfort developed by Osse and Kolcaba, which mainly surveyed physical dimensions, such as fatigue, loss of appetite, and discomfort due to medication therapy. In the psycho-spiritual dimension, some items that currently don’t exist on any instrument are: feeling sad; feeling angry; being afraid of an impending treatment intervention; experiencing a loss of freedom; feeling useful; being bored; acting more sensitive; having a sensation of patiently struggling; developing the capability to learn the disease process; feeling sick as a test from God; asking God for strength and health; being resigned, and having difficulty in praying.
In the environmental dimension, some items that were not previously examined were the discomfort caused by sharing a room with the other patients, the need to leave the hospital environment, and disliking the smell of the room. The sociocultural dimension also did not include items about sharing experience with fellow cancer patients, being happier when family members could care for them, receiving support from healthcare personnel, believing to cultural treatment, and having financial problem. Past research involving assessment instrument to determine patient comfort levels has included as many as 76 items that were assessed with Likert that range from 1-4, which was stated conditional compatibility level which had perceived. Validity and reliability test of this research have not been conducted and therefore it should be implemented. An updated instrument of comfort measurement would be useful for both, nurses and cancer patients; as well as for further development of the oncology nursing in Indonesia.
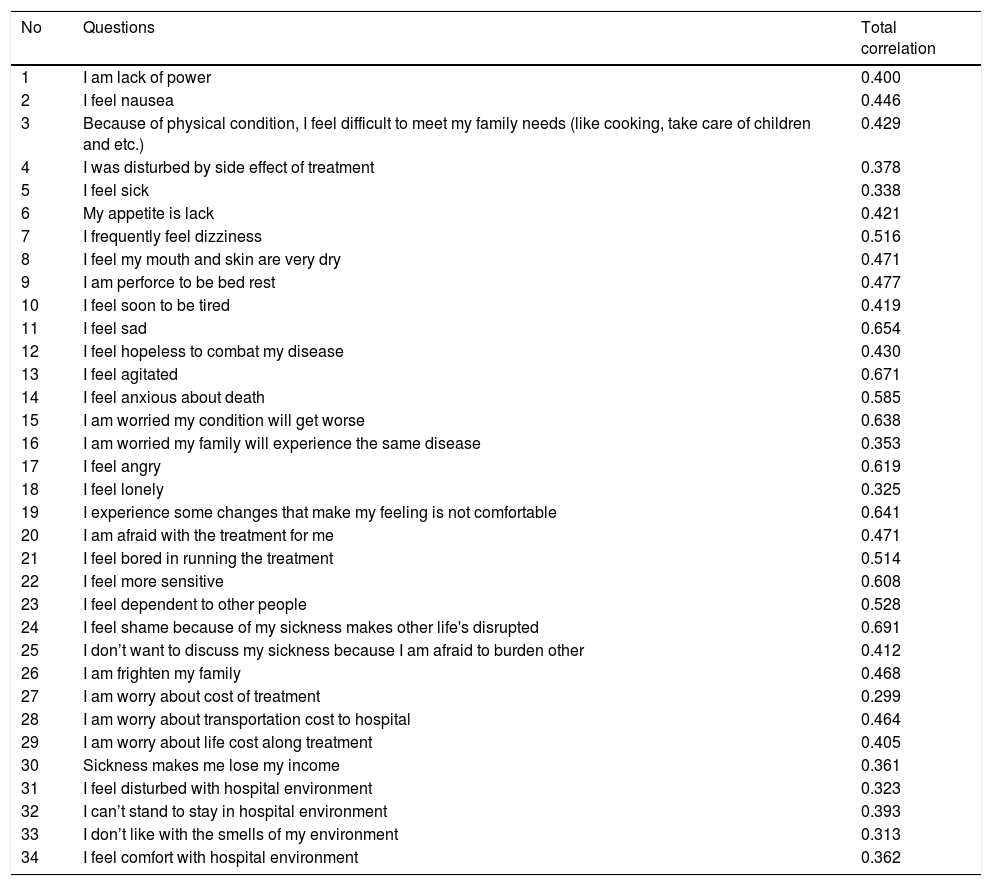
ResultsTo determine the validity of CABCI, a confirmatory factor analysis was implemented (Table 1). The instrument was tested consisted of 76 items. The test results indicated that 34 items were valid, which included 10 items that measure physical comfort, 12 items which measure psycho-spiritual comfort, 4 items measure socio-cultural comfort, 4 items measure finance comfort, and 4 items measure environmental comfort. The result of internal consistency or reliability with Cronbach's alpha score: 0.912. The lowest validity result was 0.299 for item 30 which was “i am worry about cost of treatment”. Item 26 had the highest validity at 0.691. This item was as follows “I feel shame because of my sickness makes other life's disrupted”.
The result of validity and reliability of Comfort Assessment Breast Cancer Instrument.
| No | Questions | Total correlation |
|---|---|---|
| 1 | I am lack of power | 0.400 |
| 2 | I feel nausea | 0.446 |
| 3 | Because of physical condition, I feel difficult to meet my family needs (like cooking, take care of children and etc.) | 0.429 |
| 4 | I was disturbed by side effect of treatment | 0.378 |
| 5 | I feel sick | 0.338 |
| 6 | My appetite is lack | 0.421 |
| 7 | I frequently feel dizziness | 0.516 |
| 8 | I feel my mouth and skin are very dry | 0.471 |
| 9 | I am perforce to be bed rest | 0.477 |
| 10 | I feel soon to be tired | 0.419 |
| 11 | I feel sad | 0.654 |
| 12 | I feel hopeless to combat my disease | 0.430 |
| 13 | I feel agitated | 0.671 |
| 14 | I feel anxious about death | 0.585 |
| 15 | I am worried my condition will get worse | 0.638 |
| 16 | I am worried my family will experience the same disease | 0.353 |
| 17 | I feel angry | 0.619 |
| 18 | I feel lonely | 0.325 |
| 19 | I experience some changes that make my feeling is not comfortable | 0.641 |
| 20 | I am afraid with the treatment for me | 0.471 |
| 21 | I feel bored in running the treatment | 0.514 |
| 22 | I feel more sensitive | 0.608 |
| 23 | I feel dependent to other people | 0.528 |
| 24 | I feel shame because of my sickness makes other life's disrupted | 0.691 |
| 25 | I don’t want to discuss my sickness because I am afraid to burden other | 0.412 |
| 26 | I am frighten my family | 0.468 |
| 27 | I am worry about cost of treatment | 0.299 |
| 28 | I am worry about transportation cost to hospital | 0.464 |
| 29 | I am worry about life cost along treatment | 0.405 |
| 30 | Sickness makes me lose my income | 0.361 |
| 31 | I feel disturbed with hospital environment | 0.323 |
| 32 | I can’t stand to stay in hospital environment | 0.393 |
| 33 | I don’t like with the smells of my environment | 0.313 |
| 34 | I feel comfort with hospital environment | 0.362 |
Comfort is a pivotal component in the treatment of breast cancer on patients receiving palliative care. According to Kolcaba, comfort includes physical comfort, psyco-spiritual, socio-cultural, and environmental11. The instrument was developed using Kolcaba's Leisure Theory approach. Comfort terminology has been used in the nursing profession since Florence Nightingale era and was noted in Nightingale nursing model12. The American Nurses Association (ANA) describes comfort as something that must be considered and enhanced as the main purpose of palliative care13,14. Kolcaba began to develop and analyze the concept of comfort15. Novak et al.16 developed a comfort measures as part of treatment of terminal ill patients. Although, there are a lot of theories who develop comfort model, but in Indonesia, the application of delivering comfort for terminal ill patients is still limited, both in the development of theory and practice. The construction of a theory of comfort in Indonesia should begin with the development of instruments to measure comfort in breast cancer patients. Indonesia is a country with diverse ethnic, religious, and cultural aspects that set it apart from other countries. The family support system is very strong, in Indonesia, while there is less stability in finance or economics, therefore an appropriate measurement instrument to assess comfort in breast cancer patients will be different from those designed for citizens of developed countries. It is congruent with Effendy, that found 70%-80% cancer patients in Indonesia were experienced financial problem and it affects the comfort of them9.
In the early stages of our research, we had produced drafts of instruments by interviewing patients and nurses, as well as conducting a literature review. These draft instruments contained 76 items. However, after the validity and reliability test, the instruments only consisted of 34 valid items with a validity value from 0.299 to 0.691 with 10 items to measure physical comfort, 12 items to measure psycho-spiritual comfort, 4 items to measure the socio-cultural comfort, 4 items to measure the finance comfort, and 4 items to measure environmental comfort. The results of the reliability test were high as high as 0.912, which indicated the consistency of items that were tested. This result was very encouraging because there is currently no suitable instrument for measuring comfort in breast cancer patients in Indonesia.
