




Anisakiasis is a parasitic infection caused by ingesting sea fish infected by nematode larvae. It was first diagnosed in Holland in 1960.1 Japan is currently the country with the highest incidence. It most commonly affects the stomach and small intestine, and rarely the colon. Clinical diagnosis is very difficult due to its non-specific symptoms.
In the literature, there are only 4 cases of anisakiasis linked to bowel cancer.2–5
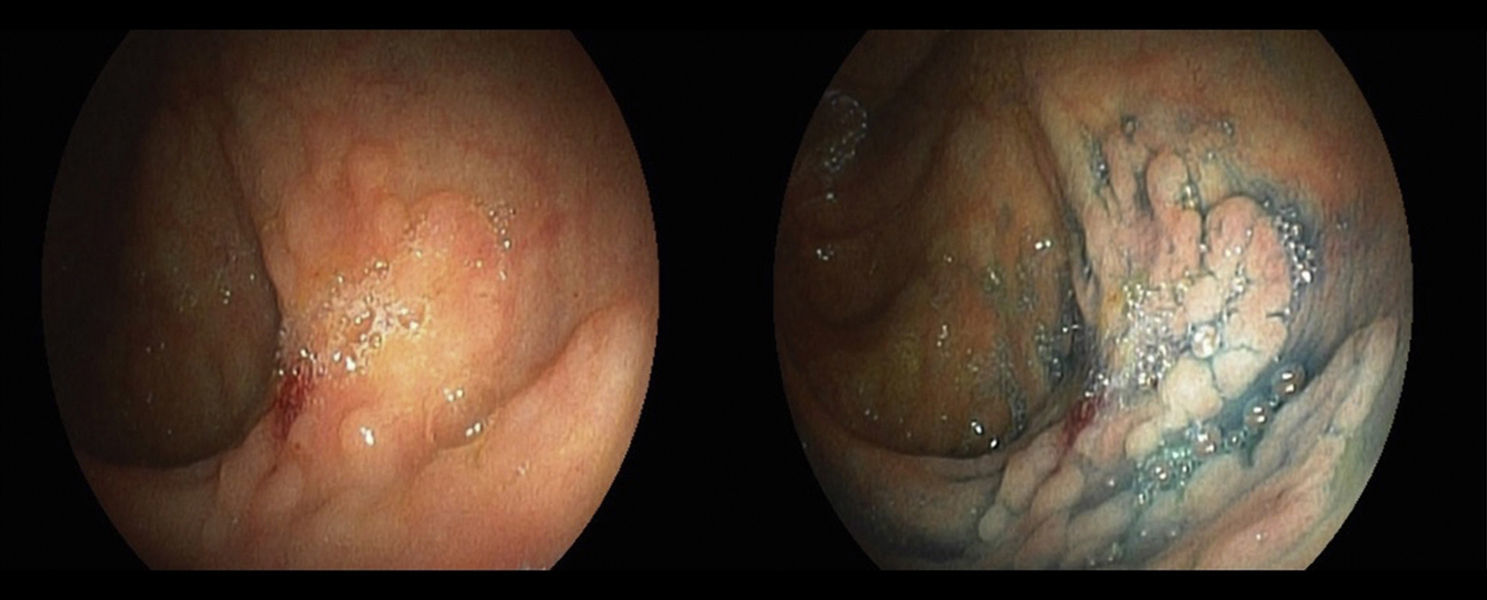
A 73-year-old male undergoing a colonoscopy for polyp monitoring, where a flat polyp of around 4cm was identified in the caecum with a lateral extension LST-G 0-IIa+0-IIb according to the Paris Classification, affecting two consecutive folds not susceptible to endoscopic resection, from which biopsies were taken (Fig. 1). The pathology study reported fragments of tubulovillous adenoma from the large intestine with high grade epithelial dysplasia/adenocarcinoma in situ, where a Haggitt level could not be established as there were several fragments. In preoperative tests, the patient's blood work showed mild eosinophilia and no significant tumour disease was observed in the imaging tests.

The patient underwent a laparoscopic right hemicolectomy and no macroscopic changes were observed during the procedure and there were no postoperative incidents.
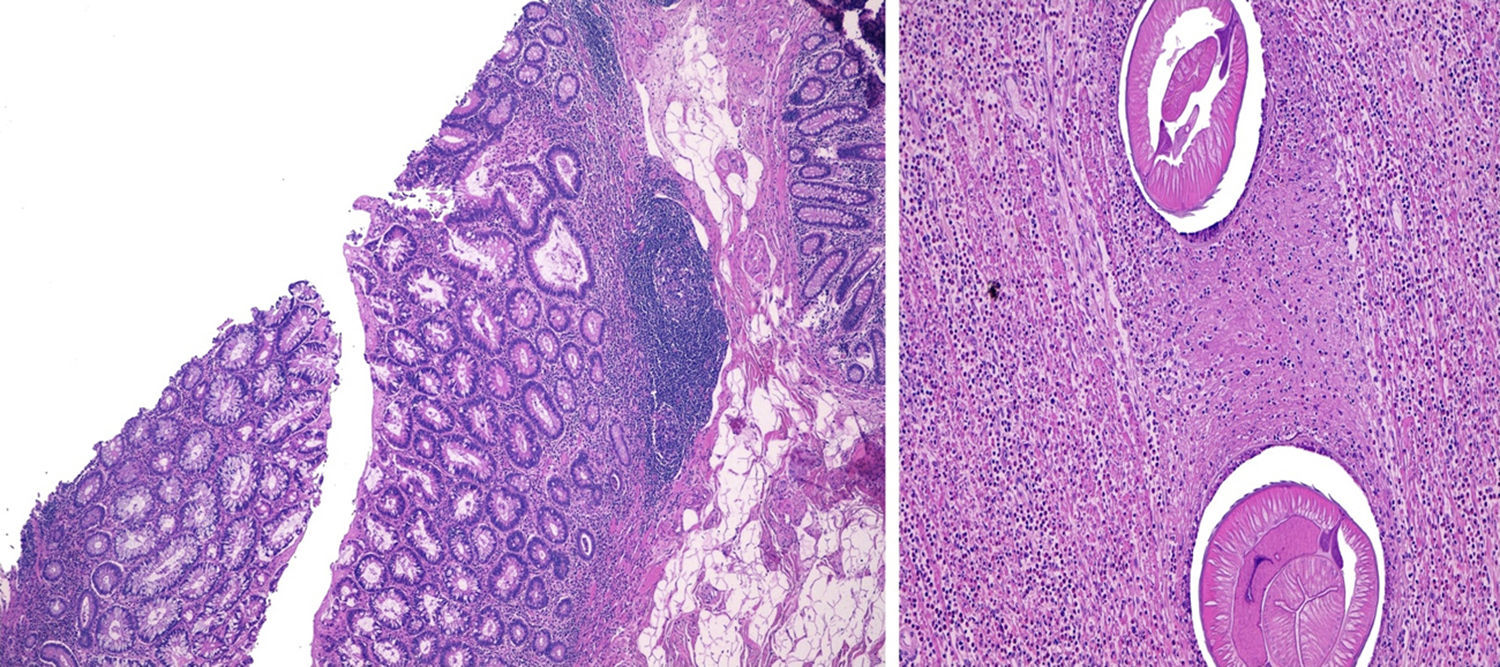
In the pathology study of the colon, the raised, oedematous mucosa in the area where the adenoma biopsies were carried out were macroscopically observed in the caecum. Microscopically, a predominantly transmural eosinophilic inflammatory infiltrate area was observed with microabscess formation, in connection with Anisakis larva, located in the muscle layer of the caecum, with low grade dysplasia in the underlying mucosa (Fig. 2), with no significant lesions in 33 isolated lymph nodes.

Anisakis involvement is less common in distal locations of the GI tract and its presence in the colon is rare.6,7 Some 75 cases of colorectal anisakiasis have been described, the majority of which were in the ascending colon.2,8
The acute forms of anisakiasis can present as acute abdominal pain or anaphylactic reaction after consuming products with Anisakis in them. Its diagnosis is based on medical history relating the recent consumption of fish and it can be confirmed with the presence of specific antibodies for Anisakis, as well as direct observation via endoscopy.
On the other hand, the chronic form is more difficult to diagnose given that the antibody titres can decrease and it could be more difficult to see the larva on the endoscopy because it could enter into the mucosa. The differential diagnosis includes appendicitis, Crohn's disease, cancer, intestinal tuberculosis…, in some cases surgical treatment is needed for its diagnosis. In early stages, it can be characterised by the presence of eosinophilic granuloma and later, it can turn into abscess tissue.
Of the 4 described cases,2–5 the larva is found in the ileum in one of them, in the ascending colon in 2 of them (although in one, the tumour is in the sigmoid colon) and another in the sigmoid colon. It is difficult to diagnose pre-operatively, and almost all are described by chance afterwards.
The coexistence of cancer and parasite colonisation has been suggested to be favoured by the changes in the intestinal immunological layers.4 Furthermore, Petithory et al.9 question whether Anisakis infection could be a factor in the development of carcinoma.
The case we present deals with a patient with a history of bowel polyps, which means it is difficult to determine the cause/effect of the association. One hypothesis could be that the parasite has taken advantage of the changes in the intestinal mucosa to pass through it, which makes the theory that parasite colonisation causes the abnormalities less plausible.
Please cite this article as: Colás Ruiz E, Lasala Gausa MA, García García E, Fernández Font JM, Martín Cavanna J, Fernández Cebrián JM. Anisakis y pólipo en colon, una asociación infrecuente. Gastroenterol Hepatol. 2017;40:21–23.
