




Lobular capillary haemangioma (also called pyogenic granuloma) is a benign vascular lesion of the skin or mucous membranes characterised by rapid growth and a friable surface.1,2 Involvement of the skin is much more common than involvement of the mucosa, where the predominant sites are the gums and the oral cavity.3 Its development in the gastrointestinal tract is very rare.4 We present the case of a 52-year-old woman with no relevant history who was referred from outpatient care, due to a haemoglobin level of 4.5g/dl, and admitted. Her only symptoms were asthenia and a single episode of haematochezia.
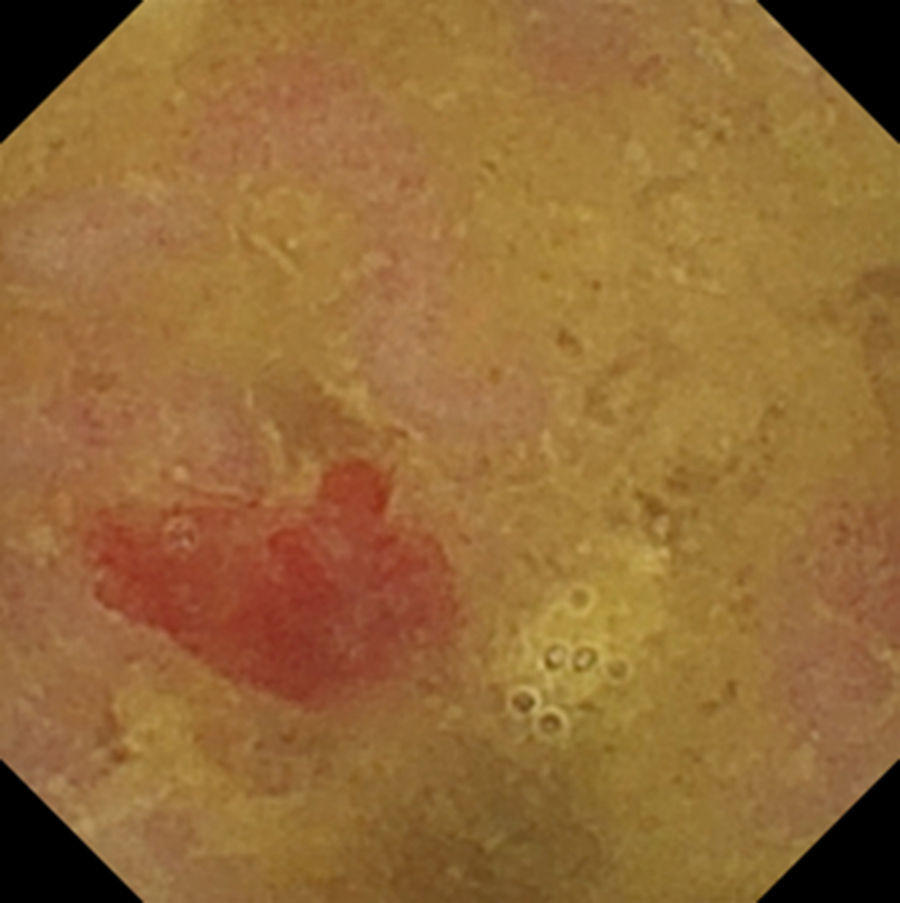
A gastroscopy was performed and detected only a mucosa with patchy erythema in the antrum and body, with no other associated lesions. An ileocolonoscopy showed isolated diverticular orifices in the sigmoid colon, with no evidence of bleeding. Subsequently, a capsule endoscopy was performed and showed a raised formation with a polypoid appearance in the jejunum and eroded mucosa at the apex of its surface, 1cm in size (Fig. 1). As it could have been related to the patient's signs and symptoms, it was decided to resect the small bowel segment described and perform a latero-lateral surgical anastomosis. The results of the histology study revealed a polypoid haemangioma (lobular capillary haemangioma) in the mucosa, superficially ulcerated with signs of bleeding, with no signs of malignancy.

The most common indication for capsule endoscopy is an assessment of suspected bleeding from the small bowel, including iron-deficiency anaemia and haemorrhage of unclear origin. However, even with the use of capsule endoscopy, it may be difficult to identify the cause of bleeding in the small bowel. Vascular abnormalities may end up being found in the gastrointestinal tract.5,6 Some lesions are present from birth or as part of syndromes; however, most are acquired throughout life.
The aetiopathogenesis of lobular capillary haemangioma is unknown. Although it may occur at any age, it is more common in children and young adults in their teens and twenties.2 In the case presented, the patient happened to be older. The surface of this lesion may ulcerate and bleeds very easily. In fact, in terms of signs and symptoms, when there is gastrointestinal involvement, patients range from being asymptomatic to presenting with macroscopic bleeding, anaemia or even dysphagia.5 Capsule endoscopy may be very helpful in its diagnosis, although its final diagnosis is histological; this lesion consists of a proliferation of capillaries with stromal oedema and mixed inflammatory infiltrate.7 Although endoscopic polypectomy, embolisation and treatment with a laser have been reported, surgical treatment may be required,8,9 as bleeding is often repeated and profuse, and surgery prevents recurrences.
FundingThis article does not have any funding.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Magaz Martínez M, Martínez Porras JL, Barrios C, Abreu L. Cápsula endoscópica: diagnóstico de hemangioma capilar lobulillar. Gastroenterol Hepatol. 2017;40:403–404.
