




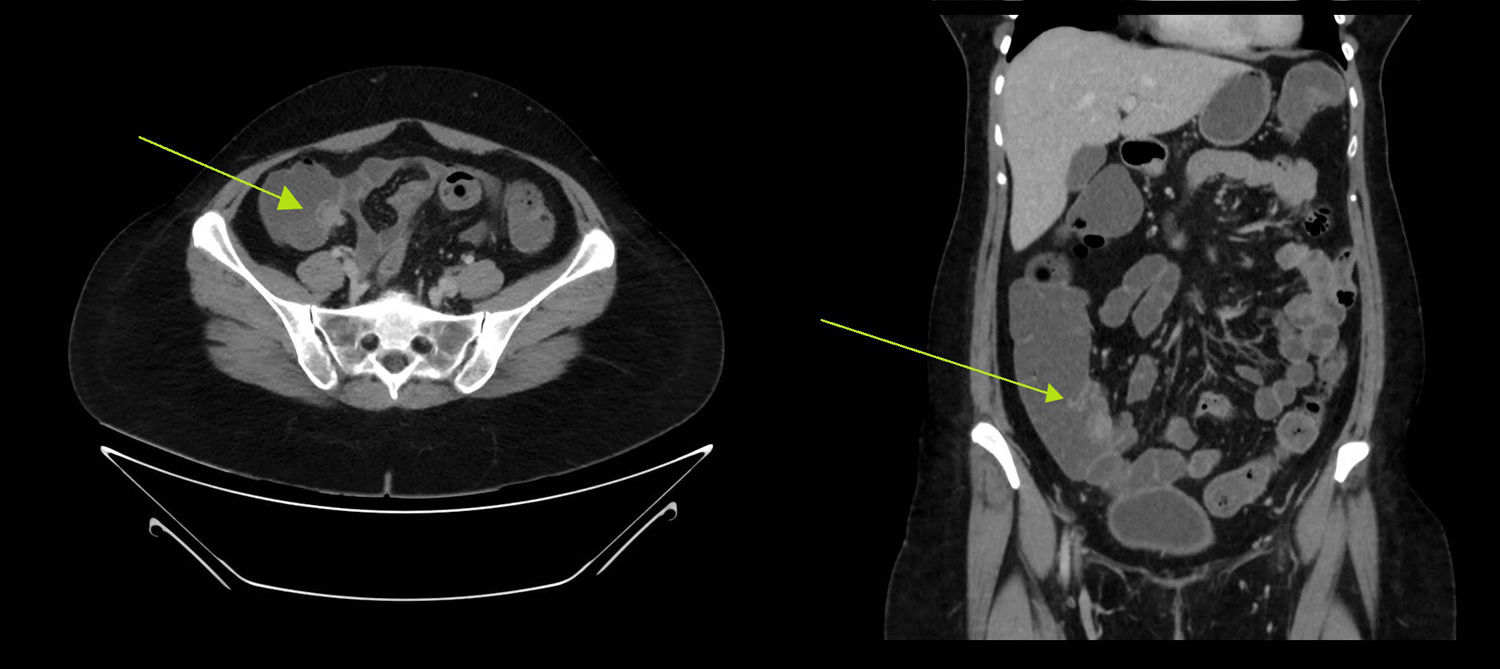
Tumours of the appendix are part of a subset of bowel cancers, the early diagnosis of which can be clinically challenging. They represent 0.5% of all gastrointestinal cancers and their prognosis depends on the type of lesion, the most common being carcinoid.1 The involvement of the appendix in endometriosis is rare, affecting only 3% of all cases, while intraluminal endometriosis is even rarer, making diagnosis difficult and even mimicking appendix cancer.2 In relation to cancer mimicking, we present the case of a 43-year-old woman with a history of hypothyroidism due to autoimmune thyroiditis and atrophic gastritis with gastric neuroendocrine tumours resected by endoscopy. In a double-contrast follow-up CT scan, a lobulated lesion was identified in the caecum adjacent to the ileocaecal valve, with contrast uptake of approximately 27×21×20mm, suggestive of cancer (Fig. 1).

Image of endometriosis mimicking carcinoid lesion in the caecum. Cross-sectional and coronal section of the double-contrast CT scan where a lobular lesion was identified in the caecum adjacent to the ileocaecal valve of approximately 27×21×20mm, suggestive of carcinoid tumour lesion. The green arrow is pointing to the lesion.
The patient had no abdominal symptoms, weight loss, rectal bleeding or change in bowel habit. Blood tests and physical examination were also normal.
Investigations were completed with a colonoscopy, which showed a protruding appendiceal ostium with an inflammatory appearance. A biopsy was taken, with the protrusion moving around. The pathology report on the biopsy revealed chronic congestive colitis with oedema of the lamina propria and minimal acute activity, with moderate local eosinophilia. The case was presented before the multidisciplinary committee and in view of the patient’s history it was decided that the patient required oncology surgery to remove the lesion.
A laparoscopic right hemicolectomy was performed, without finding any extraluminal or exophytic abnormalities, and the patient was discharged home six days later.
The pathology report was of a tumour-like lesion in the appendiceal ostium, compatible with endometriosis at the base of the implantation of the appendix, ruling out malignant disease. The patient was asymptomatic at subsequent follow-ups.
Endometriosis is the presence of endometrial glands and stroma outside the uterine cavity. There is great debate over the pathogenesis. Three theories are postulated: coelomic metaplasia, retrograde menstruation and ectopic endometrium resulting from diffusion through lymphatic and blood vessels.3
It can be classified as pelvic or extra-pelvic, with pelvic endometriosis being limited to the fallopian tubes, ovaries and nearby pelvic peritoneum, while extrapelvic endometriosis includes intestinal endometriosis in the urinary system, skin, lungs, liver and even the heart.4
Endometriosis of the gastrointestinal tract accounts for 3% to 15% of all cases.5 It is most often located in the rectosigmoid region, sometimes causing non-specific symptoms, including rectal bleeding, haematochezia, pain and obstruction, which can lead to the patient being screened for cancer.
The involvement of the appendix in endometriosis is uncommon, representing 2–3% of gastrointestinal endometriosis and 1% of endometriosis overall,5 many cases being diagnosed after an appendectomy for suspected appendicitis. In the case we describe here, due to the patient’s gastrointestinal history, imaging tests and non-specific pathology results, we were directed towards possible appendix cancer, probably a carcinoid tumour, as that is the most common type.1 We decided to perform a right laparoscopic hemicolectomy and only learned the actual diagnosis, endometriosis with caecal implantation, when we received the pathology results.
The literature describes endometriosis involving the appendix mainly at the level of the body and tip, affecting the serous or submucosal layer. Endoluminal involvement5 and location in the appendiceal ostium is very rare. The similarity in imaging tests with a carcinoid tumour, along with its location, and the lack of a pathognomonic image for diagnosis, mean it is unlikely to be suspected prior to surgery. Although in our case, the endometriosis was in the appendiceal ostium, it can present as acute appendicitis, intestinal perforation, intussusception or as a lower gastrointestinal bleeding, and it can mimic cancerous processes such as appendiceal mucoceles or carcinoid tumours. We draw attention to the back and forth between the diagnostic options of ileocaecal and appendiceal lesions to endometriosis. Although it represents a diagnostic challenge pre-operatively, it can help avoid radical or unnecessary surgery.
Please cite this article as: Gómez Sánchez J, Zurita Saavedra M, Gonzalez Puga C, Gutierrez Sainz J, Mirón Pozo B. Endometriosis colónica que simula tumor carcinoide cecal. Gastroenterol Hepatol. 2020;43:27–28.
